
 A lack of oxygen can negatively affect wound healing in a number of ways, but surgical, pharmacological, and other technological advances are allowing clinicians to enhance oxygen delivery to damaged tissues and significantly improve healing of hypoxic wounds.
A lack of oxygen can negatively affect wound healing in a number of ways, but surgical, pharmacological, and other technological advances are allowing clinicians to enhance oxygen delivery to damaged tissues and significantly improve healing of hypoxic wounds.
By Nanjin Park, DPM; Latricia Allen, DPM, MPH; Mary Nametka, MSN, RN, CWS, CWON, FNP-BC; Vickie R. Driver, MS, DPM, FACFAS
Wound healing is a dynamic interplay of processes that, even in a healthy individual, can be disrupted at any stage by a variety of factors. Why is this so important? It’s estimated that between three million and six million people in the US suffer with chronic wounds, resulting in a total cost of more than $3 billion per year in related healthcare expenditures. Patients older than 65 years are associated with 85% of these costs1 and, given our aging population, an increasing number of clients present with comorbid conditions, such as diabetes, that lead to tissue hypoxia.
Without sufficient oxygen, the healing cascade of inflammation, proliferation, and remodeling can become impaired, which can delay or “stall” wound healing at any or all wound healing stages (delayed or stalled wound healing are defined as any wound not healed within three months).2,3 One of the most significant characteristics of these impairments is a protracted inflammatory stage that leads to a collateral dysregulation between production and degradation of key healing molecules such as collagen and interleukin growth factor4 that can be attributed to wound bed hypoxia.5 Oxygen also plays an important role in production of bactericidal polymorphonuclear leukocytes (PMNs) in the wound bed, such that a lack of oxygen can increase the potential risk of infection.6 Technological advances allow clinicians to improve oxygen delivery to damaged tissues, and patients can benefit from the latest treatment modalities designed to promote the healing process.
The hypoxic wound bed: Physiology
A number of factors can contribute to creation of a hypoxic wound bed. Disrupted or impaired vasculature and high demand for energy to support regeneration of wounded tissue are typical characteristics that make both acute and chronic wounds susceptible to tissue hypoxia. It’s interesting to note that tissue oxygen tensions have been measured transcutaneously at 5 to 20 mm Hg in chronic wounds, while control tissues were measured at 30 to 50 mm Hg.7 Researchers have proposed that, in the presence of poor blood flow, the availability of oxygen to the wound site is a rate-limiting step in early wound repair and in general have identified oxygen delivery as a critical element for sustaining all phases of wound healing.6,8
Short-term acute hypoxia acts initially as a stimulus to induce cytokine and growth factor production, which is essential for chemotaxis and angiogenesis.1 Hypoxia also results in increased reactive oxygen species (ROS), chemically reactive molecules containing oxygen that are initially helpful as key messengers but damage tissues if hypoxia is prolonged and ROS involvement rises to critical levels.8
Other comorbid factors contributing to tissue hypoxia can include conditions related to pulmonary fibrosis or pneumonia, sympathetic dysregulation, hypothermia, anemia, hemodynamic instability, the need for vasopressors, cardiovascular disease, Reynaud disease, and high altitude.9 With an increasingly older cohort of patients within the general population, it is important to assess for underlying factors that can contribute to tissue hypoxia while keeping in mind that chronic wounds are typically in a hypoxic state.
Clinical assessment
It’s important to assess for contributors to compromised perfusion in patients with chronic wounds, and there are a number of tools to facilitate this process. Screening begins with a review of the patient’s medical history and a review of organ systems followed by a physical examination that includes particular attention to skin color, temperature, relative muscle bulk versus atrophy, and palpation of peripheral pulses.10 Ankle-brachial index (ABI) assessed during an office visit can guide appropriate referral to vascular services for further workup and treatment; further specialized testing may include segmental limb pressures, which are usually done in conjunction with pulse volume recording (PVR) or plethysmography; functional treadmill testing; skin perfusion pressure; laser Doppler flowmetry to assess microcirculatory perfusion; transcutaneous partial pressure of oxygen (TcPO2); duplex sonograph; magnetic resonance angiogram (MRA); and contrast angiography.11,12
Options for oxygen delivery augmentation
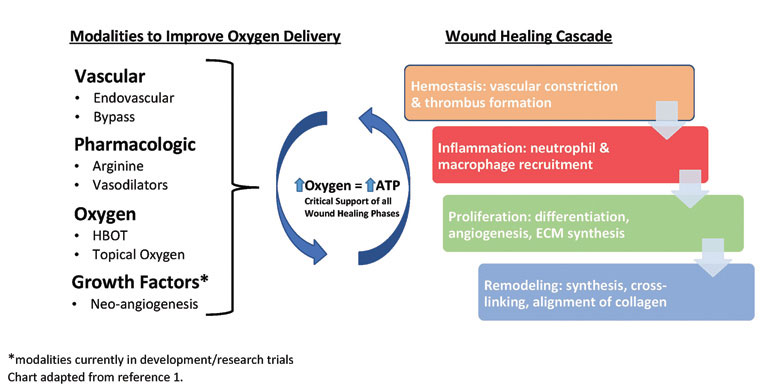
Once testing has indicated the relative degree of perfusion impairment, clinicians can consider strategies to improve oxygen delivery. There are a number of existing and newly developed interventions that represent a continuum from the invasive structural alterations inherent in revascularization and endovascular procedures to interventions with more physiologic, targeted modes of action, such as the use of pharmacologics and growth factors.
For the sake of discussion, the enhancement of oxygen delivery treatments can be grouped into four general categories (see figure, above): vascular or surgical procedures; pharmacologic agents; oxygen as therapeutic agent (eg, hyperbaric oxygen therapy or topical oxygen); and subcellular constituents (eg, growth factors).
Vascular interventions
The choice of vascular intervention is guided by clinical findings within the context of the patient’s general condition and individual quality-of-life considerations. In the setting of definite peripheral arterial disease (PAD) when surgery is not an option, consideration may be given to the daily use of an external pumping device that applies pneumatic compression to the foot and calf sequentially through sleeve-type garments to augment blood flow.13 However, this type of treatment requires many hours out of a patient’s day to obtain positive results, so adherence may be an issue and, in cases in which charges are not reimbursed, cost becomes a limiting factor.14 The arterial pump device cannot be used in cases of infection, suspected deep vein thrombosis, arterial clots, or pulmonary embolism; therefore, ongoing assessment by a licensed healthcare provider is necessary.
If providers decide surgery is the preferred option to enhance blood flow, they may recommend endovascular procedures such as endarterectomy. In these procedures, a catheter is inserted for balloon angioplasty, and a miniature device with rotary blades is used to remove the plaque within the vessel walls to improve the blood flow.15 This procedure has limitations; it improves vascular function for approximately one year, after which risk for restenosis increases.16 Open surgical procedures such as vascular bypass might offer longer periods of improved flow through removal of the diseased section of artery followed by replacement with a vein graft; however, there are increased risks associated with this procedure, including a high mortality rate.17
These methods can improve perfusion to the wound bed, and their relative benefit needs to be assessed in consultation with a vascular surgeon.
Pharmacologic
Pharmaceuticals can also assist with vasodilation, potentially improving oxygen delivery to the wound site, but specialists such as vascular surgeons or cardiologists in collaboration with other members of the patient care team need to prescribe the majority of these medications.
Pentoxifylline improves perfusion of peripheral vascular beds and may improve microcirculation as it decreases blood viscosity by reducing platelet aggregation.18 Another pharmacologic agent used in some wound healing applications is glyceryl trinitrate (GTN), more commonly known as nitroglycerin. GTN is a nitric oxide donor, and nitric oxide can cause wound site vasodilatation, which is thought to contribute to wound healing.19 The literature reports that GTN ointment is potentially useful for treating chronic anal fissures, though the evidence was not considered sufficient to support licensure for this indication in the UK.20
Another familiar drug class includes the calcium channel blockers, such as diltiazem and nifedipine. Calcium channel blockers can be helpful in treating vasculitic ulcers secondary to Raynaud disease and for prevention of digital necrosis in other connective tissue diseases.21 Iliprost, a prostacyclin analog originally developed for treating pulmonary artery hypertension, has been found to be effective in treating intermittent claudication, in which poor blood flow leads to slowed healing.22 However, as noted above, administration of all these medications, which should be used as adjunctive therapy, needs close supervision by a specialist and in some cases requires hospitalization for continuous monitoring.
A nonprescription naturally occurring amino acid, L-arginine, has been used to support angiogenesis.23 L-arginine can be synthesized endogenously, so it is classified as a nonessential amino acid, however, in people with infection, wounds, or other stressors, synthesis of L-arginine may become compromised, so it can be considered semiessential.24 L-arginine is involved with protein synthesis, cell proliferation, and cell signaling through nitric oxide production.25,26
The exact mechanism of action of nitric oxide on wound healing is still unknown;27 however, it plays a key role during the proliferative phase and is thought to improve healing by regulating collagen formation and wound contraction. Because of these multiple functions, L-arginine is considered an essential substrate for wound healing processes. It is relatively inexpensive and could be considered as an adjunctive therapy, keeping in mind it is contraindicated for use in people with a history of recent myocardial infarction.23

Transcutaneous oxygen therapy/ HBOT
In the early 1960s, practitioners in the US, Japan, and Europe started using hyperbaric oxygen therapy (HBOT) to treat wounds. Initially, researchers thought HBOT’s mode of action limited oxygen supply to the wound without substantially affecting the physiologic milieu; however, Zhao et al made a breakthrough in 1994, when they identified a synergistic response between oxygen and growth factors.28 Today, there is general agreement that HBOT increases the concentration of dissolved oxygen in the blood, stimulates angiogenesis, replaces inert gas in the bloodstream with oxygen, and has bactericidal effects.29
HBOT generally requires that patients visit a clinic two to three times a week for 90-minute chamber-based treatments. Continued increases in HBOT use have led to concerns about cost and efficacy. According to a 2000 report by the Office of the Inspector General, data from 1997 to 1998 shows charges of $76 million and $42.9 million of allowable charges for HBOT, with total costs for outpatient HBOT treatments per patient averaging between $7000 and $12,000, and, in extreme cases, exceeding $100,000.29 A recent Cochrane Database review demonstrated that HBOT significantly improved ulcer healing in the short term, but found that long-term benefit was not similarly supported by high-level evidence.30 A three-year prospective, double-blinded, randomized, controlled study is under way,31 and its findings will inform evaluations of the cost effectiveness and efficacy of HBOT in people with chronic wounds.
Transdermal continuous oxygen therapy (TCOT) is an emerging technology designed to deliver oxygen directly to the wound site. The TCOT device acts as an oxygen concentrator and delivers oxygen through a cannula to the wound site. Researchers have hypothesized that patients can accrue positive effects of oxygen therapy similar to those of HBOT using TCOT, which is less expensive than HBOT and often requires shorter sessions. Another potential benefit for localized oxygen delivery with TCOT is avoidance of oxygen toxicity, a risk associated with HBOT.32
Given the relatively recent arrival on the market of TCOT, the reported evidence consists primarily of case series.33 Kemp et al completed a TCOT study on 14 patients, each with a recalcitrant diabetic foot ulcer (DFU), and demonstrated that 86% of DFUs closed within 46 days with TCOT treatment in conjunction with appropriate offloading and local wound care.33 Driver et al performed a mechanism of action study35 to examine the efficacy and effectiveness of TCOT in chronic diabetic ulcers. After four weeks wound size had decreased 82% in the TCOT treatment group, whereas researchers noted a reduction of only 46% for the control group, which received standard care. They also noted changes in cytokine levels and proteinases favorable to healing at weeks two through four, which correlated with clinical findings. There was a significant reduction of inflammatory interleukins during this same period, suggesting that TCOT may facilitate wound healing by reversing the inflammatory process through a reduction in proinflammatory cytokines and tissue-degrading proteases.
The role of TCOT is not yet fully understood, however, and additional studies that present a higher level of evidence are needed to assess effectiveness and efficacy. At present, unlike HBOT, TCOT has not yet been approved for reimbursement.
In development: Hepatic growth factors
Other current treatments that are not yet on the market but are undergoing trials include hepatocyte growth factor and cell therapy products that contain lymphocytes, monocytes, and neutrophils to promote angiogenesis. These products are in phase III studies and unpublished data indicate that both show promising results thus far.
Hepatocyte growth factor is a paracrine cellular growth factor that regulates cell growth, motility, and morphogenesis, which stimulates mitogenesis and causes angiogenesis at the wound site.36 A phase III randomized controlled trial is assessing this therapy in patients with critical limb ischemia; the objective is to decrease pain related to ischemia and promote angiogenesis at the ischemic site. As with existing treatments, these new technologies allowing for angiogenic therapy should not be considered alternatives to conventional revascularization techniques, but rather as adjunct treatment options.
Conclusion
As healthcare moves toward an evidence-based paradigm for selection of wound treatment options, we can appreciate that research will help providers use the right products on the right wounds at the right time to achieve positive outcomes cost effectively. Certainly, the growing body of evidence will aid in selection of the most appropriate oxygen delivery systems. As with any advanced wound care therapy, decisions about which modality to use should also consider whether treatment goals are curative or palliative, how the patient defines the desired outcome, and the relative impact on available resources. Development of multiple oxygen-based delivery systems may lead to vital options that will help achieve these goals.
Nanjin J. Park, DPM, completed a two-year clinical research fellowship in limb preservation and wound healing in the Department of Surgery at the Boston University School of Medicine and Boston Medical Center and is currently working at the Outside In clinic in Portland, OR. Latricia Allen, DPM, MPH, is an attending podiatric surgeon and podiatry fellow in the Clinical Research Limb Preservation and Tissue Repair program in the Department of Surgery at the VA New England Health Care Division in Providence, RI. Mary Nametka, MSN, RN, CWS, CWON, FACCWS, FNP-BC, is owner of Healing Resources NW, which provides mobile preventive foot care, consultation, and education services, and a nurse practitioner at Optum Clinical Services, both in the Portland, OR, area. Vickie R. Driver, MS, DPM, FACFAS, is section chief, podiatric surgery; director of the Research Fellowship Program; and director of Clinical Research Limb Preservation and Tissue Repair program in the at the VA New England Health Care Division.
1. Guo S, Dipietro LA. Factors affecting wound healing. J Dent Res 2010;89(3):219-229.
2. Snyder RJ. Treament of nonhealing ulcers with allografts. Clin Dermatol 2005;23(4):388-395.
3. Mustoe T. Understanding chronic wounds: A unifying hypothesis on their pathogenesis and implications for therapy. Am J Surg 2004;187(5A):S65-S70.
4. Mustoe T, O’Shaughnessy K, Kloeters O. Chronic wound pathogenesis and current treatment strategies. Plastic Surg Reconstr 2006;117(7S):35S-41S.
5. Rodriguez PG, Felix FN, Woodley DT. The role of O2 in wound healing: A review of the literature. Dermatol Surg 2008;34(9):1159-1169.
6. Broughton G 2nd, Janis JE, Attinger CE. The basic science of wound healing. Plastic Reconstr Surg 2006;117(7 suppl):12S-34S.
7. Khanna S, Wallace WA. Wound healing: Oxygen and emerging therapeutics. Antioxid Redox Signal 2002;4(6):961-963.
8. Stadelmann WK, Digenis AG, Tobin GR. Physiology and healing dynamics of chronic cutaneous wounds. Am J Surg 1998;176(2A Suppl):26S-38S.
9. Menke NB, Ward KR, Witten TM, et al. Impaired wound healing. Clin Dermatol 2007;25(1):19-25.
10. American Diabetes Association. Preventive foot care in people with diabetes. Diabetes Care 2003;26(Suppl 1):S78- S79.
11. Peebles C. Update on non-invasive vascular studies. In: Southerland JT, ed. McGlamry’s Comprehensive Textbook of Foot and Ankle Surgery. Philadelphia, PA: Wolters Kluwer/Lippincott Williams & Wilkins; 1996.
12. Anderson CA. Noninvasive assessment of lower extremity hemodynamics in individuals with diabetes mellitus. J Vasc Surgery 2010;52(3 Suppl):76S-80S.
13. Eze AR, Comerota AJ, Cisek PL, et al. Intermittent calf and foot compression increases lower extremity blood flow. Am J Surg 1996;172(2):130-135.
14. Konsantinos TD, Nicolaides A. Effect of intermittent pneumatic compassion of foot and calf on walking distance, hemodynamics, and quality of life in patients with arterial claudication. Ann Surg 2005;241(3):431-441.
15. Health Quality Ontario. Stenting for peripheral artery disease of the lower extremities. Ont Health Technol Assess Ser 2010;10(18):1-88.
16. Naoum JJ, Arbid EJ. Endovascular technique in limb salvage: Infrapopliteal angioplasty. Methodist Debakey Cardiovasc J 2013;9(2):103-107.
17. Ouma GO, Zafrir B, Mohler ER 3rd, Flugelma MY. Therapeutic angiogenesis in critical limb ischemia. Angiology 2012;64(6):466-480.
18. Enoch S, Grey JE, Harding KG. ABC of wound healing: Non-surgical and drug treatments. BMJ 2006;332(4):900-903.
19. Luk PP, Sinha SN, Lord R. Upregulation of inducible nitric oxide synthase (iNOS) expression in the faster healing chronic leg ulcers. J Wound Care 2005;14(8)373-382.
20. Hwang DY, Yoon SG, Kim HS, et al. Effect of 0.2% glyceryl trinitrate ointment on wound healing after hemorrhoidectomy. Dis Colon Rectum 2003;46(7):950-954.
21. Karukonda SRK, Flynn TC, Boh EE, et al. The facts of drugs on wound healing–part II. Specific classes of drugs and their effect on healing wounds. Int J Dermatol 2000;39(5):321-333.
22. Afsharfard A, Mozaffar M, Malekpour F, et al. The wound healing effects of iloprost in patients with Buerger’s disease: claudication and prevention of major amputations. Iran Red Crescent Med J 2011;13(6):420-423.
23. Boger RH. L-arginine therapy I cardiovascular pathogies: Beneficial or dangerous? Curr Opin Clin Nutr Metabol Care 2008;11(1):55-61.
24. Schwedhelm E, Maas R, Freese R, et al. Pharmacokinetic and pharmacodynamics properties of oral L-citrulline and L-arginine: impact on nitric oxide metabolism. Br J Clin Pharmacol 2008;65(1):51-59.
25. Witte MB, Barbul A. Arginine physiology and its implication for wound healing. Wound Repair Regen 2003;11(6):419-423.
26. Sato H, Zhao ZQ, Vinten-Johansen J. L-arginine inhibits neutrophile adherence and coronary artery dysfunction. Cardiovasc Res 1996;31(1):63-72.
27. Isenberg JS, Ridnour LA, Espey MG, et al. Nitric oxide in wound healing. Microsurg 2005;25(5):442-451.
28. Zhao L, Davidson JD, Sang CW, et al.Effect of hyperbaric oxygen and growth factors on rabbit ear ischemic ulcers. Arch Surg 1994;129(10):1043-1049.
29. Brown JB. Department of Health and Human Services, Office of the Inspector General. Hyperbaric oxygen therapy. http://www.dhh.gov/progorg/oei. Effective October 2000. Accessed April 18.
30. Zamboni WA, Browder LK, Martinez J. Hyperbaric oxygen and wound healing. Clin Plast Surg 2003;30:67-75.
31. Kranke P, Bennett MH, Martyn-St. James M, et al. Hyperbaric oxygen therapy for chronic wounds. Cochrane Database Syst Rev 2012;4:CD004123.
33. Daly MC, Faul J, Steinberg JS. Hyperbaric oxygen therapy as an adjunctive treatment for diabetic foot wounds: a comprehensive review with case studies. Wounds 2010;22(1):1-11.
34. Kemp DG, Hermans MHE. An evaluation of the efficacy of transdermal continuous oxygen therapy in patients with recalcitrant diabetic foot ulcer. J Diabet Foot Compl 2011;3(2):6-12.
35. Driver VR, Yao M, Kantarci A, et al. A prospective, randomized clinical study evaluating the effect of transdermal continuous oxygen therapy on biological processes and foot ulcer healing in persons with diabetes mellitus. Ostomy Wound Manage 2013;59(11):19-26.
36. Nakamura T, Sakai K, Nakamura T, Matsumoto K. Hepatocyte growth factor twenty years on: much more than a growth factor. J Gastroenterol Hepatol 2011;26(Suppl 1):188-202.





