
Walking is the best possible exercise. Habituate yourself to walk very far. Thomas Jefferson

By Renan L. Monteiro, Jane S. S. P. Ferreira, Érica Q. Silva, Ronaldo H. Cruvinel-Júnior, Jady L. Veríssimo, Sicco A. Bus, and Isabel C. N. Sacco
Diabetic peripheral neuropathy (DPN) is associated with decreased muscle strength and physical activity level, as measured by steps per day and reduced gait speed. Studies suggest that motor and sensory deficits and reduced foot-ankle range of motion (ROM) are related to decreased physical activity levels, as are the reduced quality of life (QoL) and decreased gait speed associated with DPN. Additionally, diabetes progression and DPN compromise musculoskeletal function, leading to limitations in everyday physical functioning.
This study sought to determine whether a foot-ankle therapeutic exercise program can improve daily physical activity (i.e., number of steps) and fast and self-selected gait speed in people with diabetic peripheral neuropathy (PWDPN), as well as modify risk-factor outcomes in this population.
Methods
The primary aim of this single-blind randomized controlled trial (RCT) was to investigate the effects of a 12-week foot-ankle therapeutic exercise program on daily physical activity level (number of steps measured by an accelerometer) and self-selected and fast-gait speeds in PWDPN. Secondary aims were to investigate the effectiveness of this intervention at 6, 12, and 24 weeks on passive and static ankle-joint ROM, tactile (10-g monofilament) and vibration sensitivity (tuning fork), DPN symptoms (Michigan Neuropathy Screening Instrument), QoL by the EuroQoL 5-dimensions (EQ-5D) questionnaire, foot health and functionality by the Foot Health Status Questionnaire, hallux and toe muscle strength (pressure platform), and foot ulcer incidence at 1-year follow-up. All primary and secondary outcomes were planned to be assessed at 1-year follow-up; however, due to the COVID-19 pandemic, these aims were modified.
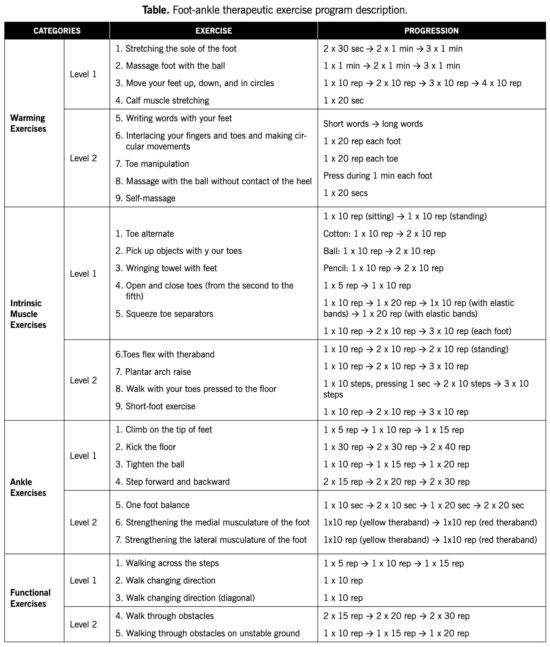
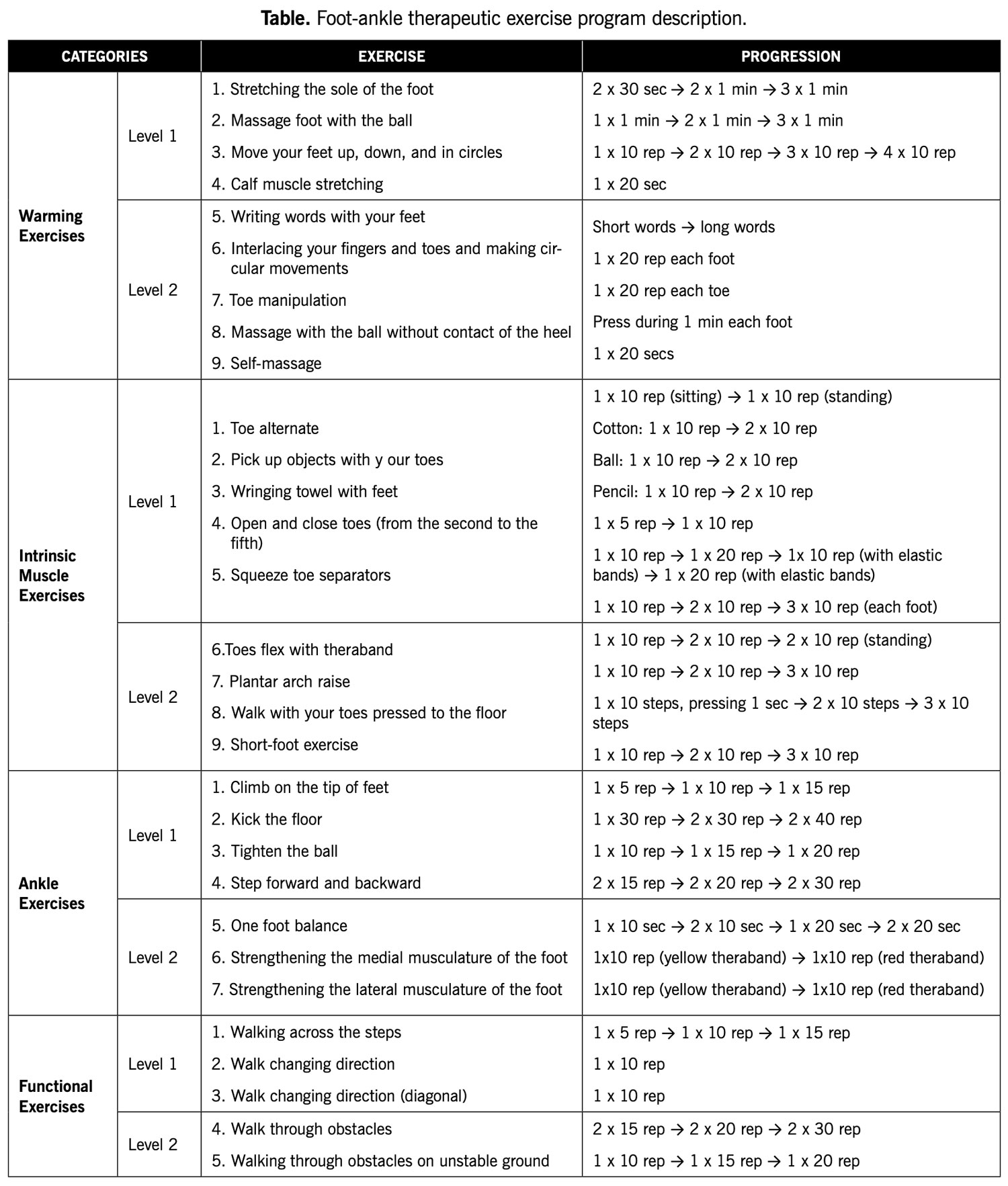
Seventy-eight volunteers with DPN were allocated into a control group (CG), which received usual care (inspect your feet daily, wear socks without elastic and seams, cut your nails properly, avoid cutting corns or blisters without supervision, avoid going barefoot or wearing shoes without socks or slippers, and seek medical attention whenever you identify foot problems), and an intervention group (IG), which received usual care plus a 12-week foot-ankle exercise program. The exercise protocol was performed twice weekly under in-person supervision by a physiotherapist, and twice weekly at home, remotely supervised through Educational Diabetic Foot Software. Both protocols consisted of warm-up exercises, intrinsic foot muscle strengthening, extrinsic foot-ankle muscle strengthening, and functional exercises, such as balance and gait training (See table on page below).
 Results & Discussion
Results & Discussion
IG participants increased their fast-gait speed after 12 weeks of the program and maintained this greater speed, even after 1 year. The IG participants showed a mean difference of 0.18 m/s compared with CG participants, a greater increase than that recommended for clinical improvement and mortality reduction (0.10 m/s). Thus, the foot-ankle exercise program presented in this study potentially promotes an indirect protective effect against mortality risk.
The number of steps taken over a 6-day period did not differ between groups after 12 weeks. While all participants started the study at a moderate activity level (7,641 and 8,092 steps in the CG and IG, respectively), the CG showed decreasing activity level, to 7,093 steps, by the 1-year follow-up. The IG remained at a moderate activity level at the 1-year follow-up (8,458 steps). The status of being moderately active represented a health advantage for the IG, because in addition to helping with lifestyle and activities of daily living (ADL), more steps could improve musculoskeletal capacity, especially foot-ankle muscle strength.
After 12 weeks of foot-ankle training, the IG showed increased ankle dorsiflexion ROM compared with the CG (P = 0.048; interaction effect). In the 24-week and 1-year follow-ups, there were no differences between groups in ROM. Nor were there significant differences between foot-ankle training and usual care on toe muscle strength. These findings and the positive results from other cited RCTs and non-controlled studies reinforce the importance of exercising the foot-ankle to gain this clinically relevant outcome.
The foot-ankle intervention did not affect DPN symptoms and tactile sensitivities. However, after 12 weeks of foot-ankle training, the IG presented better vibration sensitivity compared with the CG (P = 0.030; interaction effect), and that difference was maintained at the 1-year follow-up assessment (P = 0.023; interaction effect). The clinical importance of vibration sensitivity for the development of diabetic foot ulcers has been demonstrated by research associating current or past DFUs with altered tuning fork vibration perception.
The foot-ankle exercise program yielded a positive effect on QoL at the 24-week follow-up compared with the CG. Compared to baseline assessment, the IG showed a significantly improved QoL score at 12 (P = 0.006, time effect) and 24 (P = 0.006, time effect) weeks, as well improved foot pain scores at 12 and 24 weeks (P = 0.044 and P = 0.026; time effect, respectively). The CG also showed improvements in foot health after 1 year, compared with baseline and 6 weeks (P = 0.001 and P = 0.025; time effect, respectively). The foot-health improvement in the CG might be due to the usual-care guidance offered to the patient during the orientation session, with the placebo effect also being an important consideration.
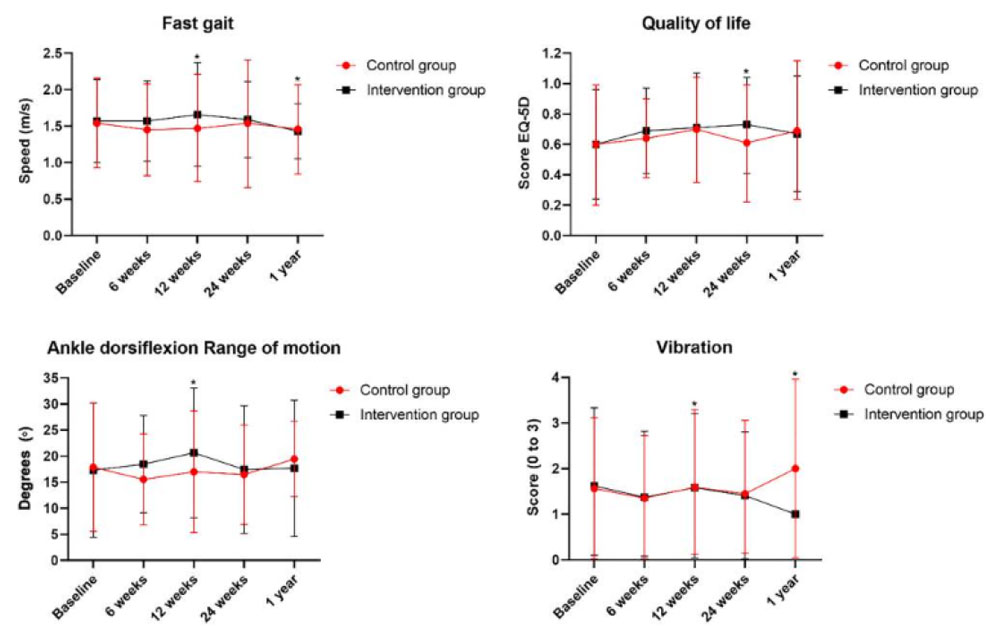
Figure. Difference between intervention group and control group on fast gait speed, quality of life, ankle range of motion and vibration outcomes.
Over a 1-year follow-up, 1 participant from each group developed a plantar foot ulcer. The IG participant was diagnosed about 13 weeks after randomization, whereas the CG participant was diagnosed about 5 weeks after randomization. Due to an insufficient number of participants with foot ulcers, it cannot be determined whether the later time to develop an ulcer in the IG participant was linked to the intervention.
Conclusions
The study authors concluded that the 12 weeks of the foot-ankle therapeutic exercise program showed positive effects compared with usual care on the primary outcome of fast-gait speed, and on the secondary outcomes of foot-ankle ROM, vibration sensitivity, and QoL. However, no effects were seen on the 2 other primary outcomes after 12 weeks (self-selected gait speed and number of steps), although a 1,365-step difference between groups was observed at 1-year follow-up. Improvements in vibration sensitivity and ROM may indicate an improvement in modifiable risk factors for foot ulceration, whereas an increase in gait speed may be an indicator related to mortality reduction in this population. Taken together, the findings of our study suggest that foot-ankle exercises may be an effective complementary treatment strategy for improving some musculoskeletal and functional deficits related to DPN. For other outcomes, larger trials are needed to further investigate the effects of such an exercise program.
This article has been excepted from “Foot-ankle therapeutic exercise program can improve gait speed in people with diabetic neuropathy: a randomized controlled trial,” by the authors noted above, which was published online on May 9, 2022, in the journal Scientific Reports 12, 7561 (2022). https://doi.org/10.1038/s41598-022-11745-0. Editing has occurred, including the renumbering of tables, and references have been removed for brevity. The table on page 47 is from the online Supplementary information. Use is per CC BY 4.0.





