
 By Dr. James McGuire DPM, LPT, LPed, FAPWHc
By Dr. James McGuire DPM, LPT, LPed, FAPWHc
Early assessment and intervention of acquired adult flatfoot, particularly concerning Posterior Tibial Tendon Dysfunction (PTTD) is essential. I’ll be discussing proactive management, emphasizing the importance of early intervention, comprehensive foot assessment, and the strategic application of orthotic devices to prevent the progression of PTTD and improve long-term patient outcomes.
Proactive Intervention and Biomechanical Balance
A significant failure in current practice is that a lot of the time we fail to warn asymptomatic biomechanically imbalanced people of the risk of PTTD or offer preemptive orthotic intervention. Early intervention is key, even in asymptomatic individuals, by assessing foot and ankle alignment and considering family history of foot and ankle pain we can more accurately access the likelihood of future issues and treat them before they begin. The underlying philosophy is to balance the foot to prevent future pathology, rather than waiting for pain and dysfunction to develop.
Evolution of PTTD Classification Systems
The historical progression of PTTD classification systems, emphasizing their shift from purely tendon-focused to more comprehensive biomechanical models are as follows:
- Johnson and Strom (1989): Primarily focused on tendon and tendon pathology, categorizing stages based on swelling and tenderness. A key critique is its oversimplification of Stage 2 and the mistaken assumption of no instability in Stage 1. It failed to account for subtalar, lateral column, and medial column instabilities that often precede rigid deformity.
- Myerson’s Classification: Incorporated a broader range of deformities, including hindfoot valgus, midfoot collapse, and forefoot abduction/adduction. This represented a move toward recognizing the resultant structural changes from tendon pathology.
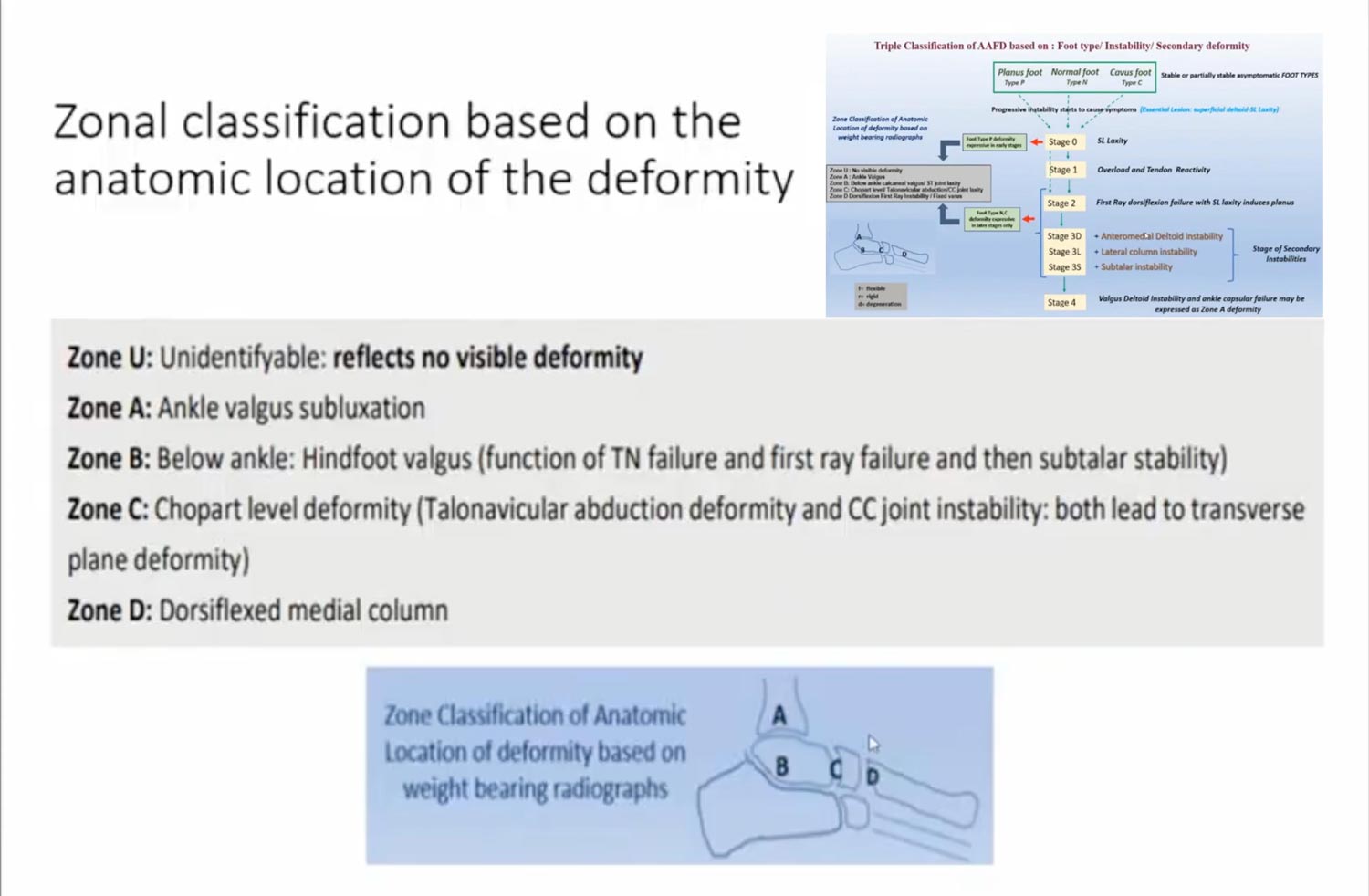
- Paspula’s Triple Classification: This is presented as a more advanced and significant classification, focusing on foot types (planus, normal, cavoid) and stages of ligamentous laxity and reactivity. It emphasizes that pain often stems from ligament and soft tissue stresses on the nerves within those soft tissue structures due to laxity and stretching. Subtalar ligament laxity (Stage 0) can arise from anatomical variation, constant pronation stress, or unaddressed minor injuries (eg, ankle sprains that heal with increased flexibility).
- Zonal Classification (U, A, B, C, D): This further refines the Paspula classification by correlating foot type with specific zones of deformity progression (eg, Zone B indicates hindfoot valgus and subtalar instability, Zone D signifies dorsiflexed medial column and abducted forefoot).
Current Theories of Foot Function and Orthotic Design
Theories that underpin foot function and orthotic prescription and highlight the shift toward a more dynamic and pain-focused approach are:
- Root Neutral Theory (Foot Morphology Theory): A structural theory focusing on inherited planar positions (eg, forefoot varus/valgus) and their compensatory motions. This historically led to precise mathematical calculations for orthotic angles.
- Dananberg’s Sagittal Plane Facilitation: Emphasized the importance of medial column function and plantar fascial tightening for arch restoration.
- McPoil and Kirby’s Tissue Stress Theory: This theory is a significant departure, focusing primarily on reducing the stresses to the point where the patient has no pain and then allowing them to function. It suggests that orthotics may not always need to restore complete neutral alignment and can sometimes be temporary and based on pain.
- Whitney’s Triplane Balance Theory (Active Structural Control): Advocates for orthotics that enable the foot to restore itself using normal neuromuscular functions, minimizing the need for excessive muscle action or stress on tendons. This aligns with the idea of achieving dynamic stability.
- Glaser’s MASS Theory (Arch Supination Stabilization): Uses calibrated leaf springs to oppose postural changes, focusing more on the effect than rigid structural correction.
- MacConaill-Sarrafian Twist the Plate Theory: Focuses on the winding and unwinding of the twist of the plate within the foot.
Blending these theories gives patients the best outcomes. The importance of restoring the foot to a neutral alignment, when possible, even while acknowledging the tissue stress theory’s focus on pain reduction.
The Critical Role of the Subtalar Axis and Kirby Skive Orthoses
A central and most important concept presented is the subtalar axis and its manipulation through Kirby Skive orthoses.
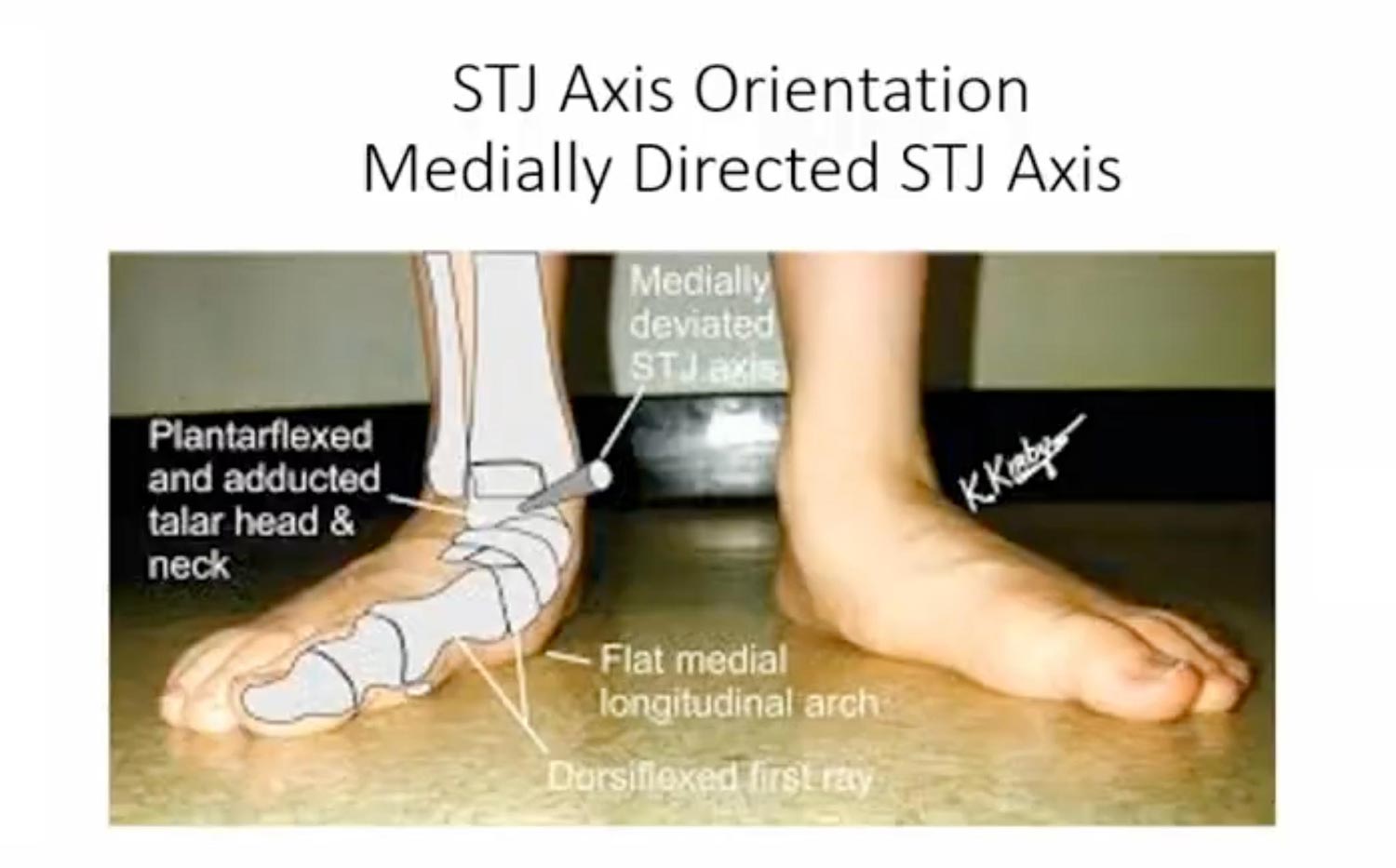
- Subtalar Axis: This anatomical axis shifts medially during pronation and laterally during supination. If the axis is medially deviated in a pronated foot, common orthotic interventions like forefoot varus wedges or increased arch height will only increase pain and pronation by applying force ineffectively.
- Kirby Skive Orthosis: This device, initially developed by Blake and refined by Kirby, involves a marked inversion of the rearfoot heel seat. Its purpose is to control the foot way in the back early in the gait cycle. The Kirby Skive grabs the heel very early in the gate cycle. As soon as you hit the ground, your foot is inverted and prevented from going past that position of balance or that center axis of balance in the shoe.
Working with my mother’s severe PTTD, which was resolved only after incorporating a 50-degree Kirby Skive in her orthotic, despite initial hesitation and conventional wisdom. This dramatic success underscores my belief in aggressive rearfoot inversion.
- Measurement and Modification: The Kirby Skive is measured in millimeters of cut into the plaster cast, which correlates to angular correction of the heel seat. McGuire Kirby Skive modification : For every 2 degrees of calcaneal eversion, we would add 10 degrees of Kirby Skive to the positive mold. This involves rasping a flat onto the medial calcaneal tuberosity area of the positive mold.
- Reduction Casting (“Creative Casting”): This technique involves actively manipulating the foot during casting, often by lightly plantarflexing the first ray and slightly dorsiflexing the hallux, to achieve a more balanced foot position in the cast. This contrasts with Root’s neutral position casting.
Balance as the Key to Function
Balance–both structural and dynamic–is crucial for foot function and overall posture.
- Active Structural Control: Is an engineering term applied to the body, implying the use of neuromuscular control to maintain skeletal alignment. The foot is not a static structure but a “dynamic” one, with skeletal, ligamentous, myotendinous, and neurological control systems working in concert.
- Center Axis of Balance: This is ideally located along the second metatarsal, where the body’s center of gravity attempts to stay. Imbalances (osseous, myotendinous, etc.) shift these vectors, leading to compensation.
- Kinetic Chain Reaction: Imbalances at the foot level can trigger a “big kinetic chain reaction” throughout the body, affecting hips, spine, shoulders, and head, as the body strives to keep the eyes level and maintain equilibrium.
- Multiaxial Midtarsal Joint: The midtarsal joint (talonavicular and calcaneocuboid) is described as “instantaneously multiaxial” and “genetically unique,” making it highly adaptable but also susceptible to dysfunction when ligaments are weakened or torn due to trauma or degeneration.
- Digital Reaction Patterns: Foot imbalance leads to compensatory gripping or shifting of the toes, visible in digital reaction patterns.
- Restoring Balance with Orthotics: Orthotics are designed to “restore the balance,” not just adjust for fixed angular deformities. The goal is to bring the center axis of balance into alignment. The art of medicine is in this, as precise manipulation during casting can be difficult with static scanning devices.
Treatment Modalities Beyond Orthotics
Customized orthotics are very helpful, but there are other interventions for PTTD:
- Footwear: Good supportive footwear with a deep heel cup, supportive counter, and potentially a rocker sole is critical, especially for women who tend to wear less supportive shoes. (There was a surge in PTTD cases during COVID-19 due to increased barefoot or slipper-wearing at home.)
- Physical Therapy: Crucial for strengthening tendons once pain is reduced, but patients must remain in a supportive orthosis during rehabilitation.
- AFOs (Ankle-Foot Orthoses): A deep heel cup orthosis typically used for children but can be effective for adults with flexible flat feet, especially when coupled with a Kirby Skive.
- SMOs (Supramalleolar Orthoses): Extensions of the UCBL above the ankle, used to prevent surgery or osseous intervention.
- Arizona Brace: Designed specifically for PTTD but criticized for its bulkiness (difficulty with shoes), unhinged ankle (requiring rocker soles), and often inadequate foot plate. Primarily for late Stage 2, 3, and 4 PTTD.
- Richie Brace: Hinged AFO designed to allow ankle motion and eliminate the need for rocker soles. However, the orthotic component within the Richie brace is often insufficient; it requires a good Kirby Skive deep heel orthosis with a perfectly balanced foot as an adjunct.
- Aircast/Simple Ankle Braces: Provide ankle stabilization but fail to address the underlying foot function and pronation, often leaving the PTT still stressed.
- Crow Boots: Generally inappropriate for PTTD due to weight, cost, and lack of true weight-bearing relief, reserved for inoperable feet with ruptured tendons.
- Torch Walker (Total Contact Orthotic Restraining Custom Hybrid): A fixed-ankle, cosmetically acceptable alternative for severe, inoperable cases with ruptured tendons and pain. Critiqued for often lacking a properly designed rocker.
Conclusion
There is a great need for a paradigm shift in PTTD management, emphasizing early assessment and intervention even in asymptomatic individuals with biomechanical imbalances. The core of this approach centers on the strategic use of Kirby Skive orthoses with a deep, inverted heel seat, aiming to control the subtalar axis early in the gait cycle and restore the foot’s center axis of balance. This, coupled with appropriate footwear and physical therapy, offers a powerful means to prevent PTTD progression and improve long-term patient comfort and function, moving beyond mere symptom reduction to true biomechanical correction. The art of medicine in this process, where clinician expertise and manipulation are paramount over mere numerical measurements.
Dr. James McGuire is the director of the Leonard S. Abrams Center for Advanced Wound Healing and a Professor Clinician Scholar in the Departments of Podiatric Medicine and Biomechanics at the Temple University School of Podiatric Medicine in Philadelphia. His undergraduate degree is from Bucknell University in Lewisburg, PA (1974), and his Physical Therapy Certificate is from the University of Pennsylvania, Philadelphia, PA. (1975) He practiced physical therapy in Philadelphia until 1977 when he entered Podiatric medical school. Dr. McGuire is a board-certified podiatrist and wound care specialist. He has more than 40 years of experience in biomechanics and wound management, has published extensively, and has participated in several research trials involving the diabetic foot and wound healing. Dr. McGuire has lectured both nationally and internationally in the areas of wound healing, diabetic foot management, off-loading, and biomechanics of the at-risk foot.
This article is a summary of Dr. McGuire’s presentation, “Early Assessment and Early Intervention of Acquired Adult Flatfoot to Prevent Future PTTD” from the 2024 Conservative Approach to PTTD held May 11, 2024. To view the full presentation with questions and answers—and see the agenda for the program, visit https://pttd.lerexpo.com/en/. Continuing education credits are available for this and many of the lerEXPO programs.






Finally, a physician that gets it! Good article. Appreciate all the different variances that are needed. It must be overstated that each case is individualized and must be helped in an individual way. There is no one way for everybody. And if you have not tried the custom Tilges ankle gauntlet it is a must for the best substitute for a traditional Arizona. The other thing is that most people do is they try to overcorrect the alignment. It cannot be overstated enough that the patient must be put in placed in their most correctable position, exactly.