By Jichong Ying, Jianlei Liu, Hua Wang, Yunqiang Zhuang, Tianming Yu, Shuaiyi Wang, and Dichao Huang
Posterior malleolus fractures have been associated with ankle instability because the ligament pull that follows such fractures can lead to movement of the fracture fragment and consequently disrupt the weight-bearing surface’s integrity.
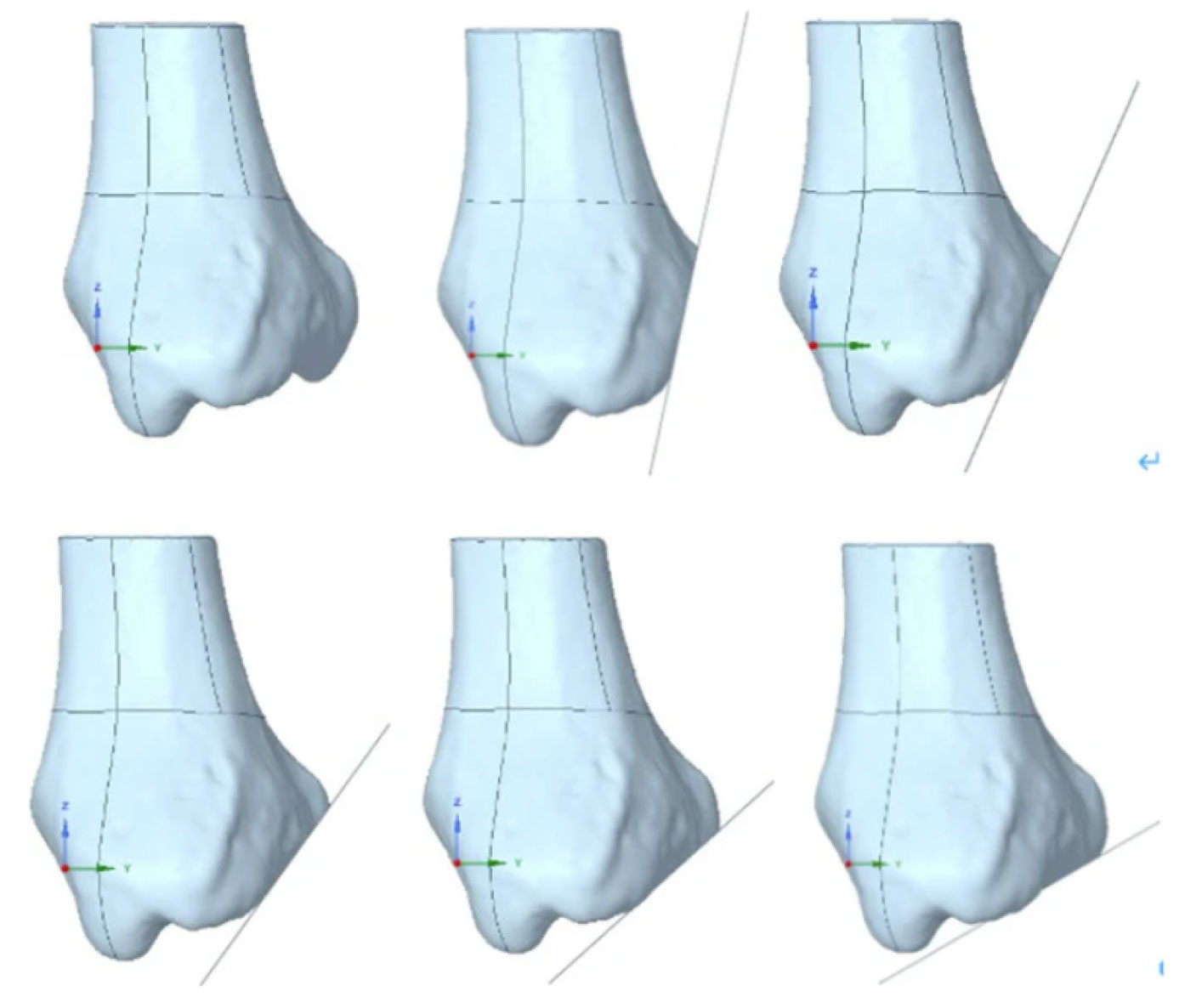
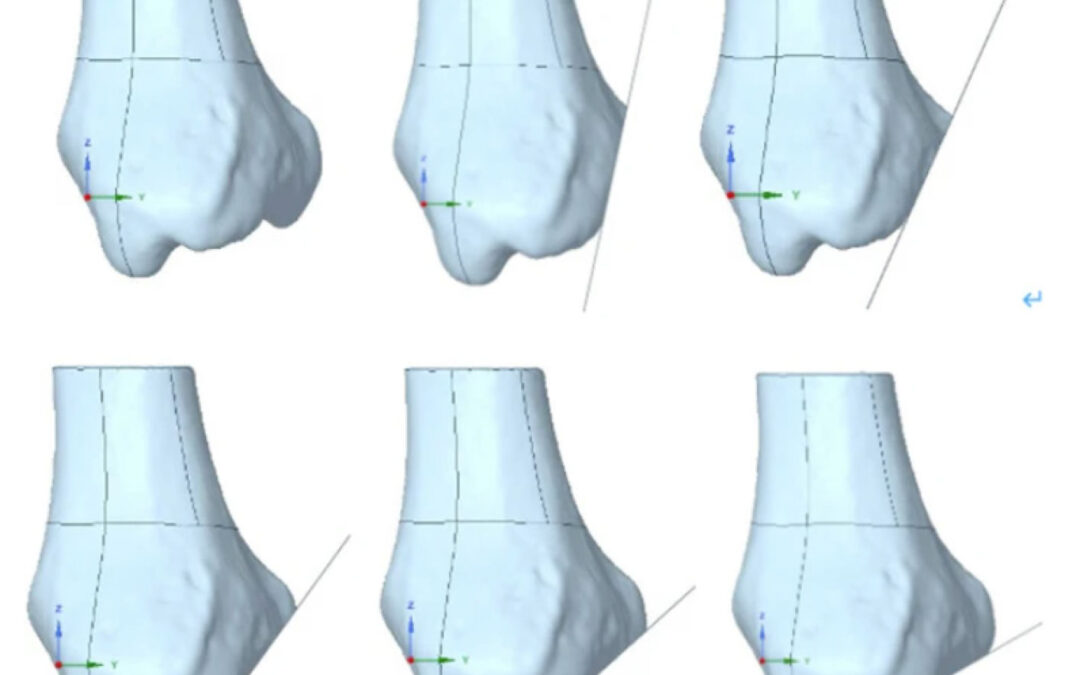
Figure 1: Comparison of the intact bone and 5 different fracture line locations. The top left image displays the intact bone, while the remaining images present varying sagittal angles from 12° to 60°
Posterior malleolus fractures have a reported prevalence spanning 10% to 44% of all ankle fractures and are known to be associated with ankle instability and a heightened development of complications like traumatic arthritis. This adverse sequela is primarily attributed to the disrupted and intermittent contact of the articular surface, leading to degenerative changes over time. Such clinical observations have emphasized the acute intervention these fractures require and have accentuated the need to elucidate the underlying pathological mechanisms and biomechanical nuances driving their occurrence, comprehension of which holds the promise of paving the way for innovative, patient-specific treatment.
The complexities involved in obtaining precise laboratory-based spatial pressure measurements of the ankle highlight the significance of exploring the biomechanical implications of these fractures. Thus, this study aimed to identify stress concentration zones and understand the influence of sagittal angles on stress distribution in order to bridge the knowledge gap.
Methods
Data collection protocol began with the acquisition of 3D computed tomography (CT) scans from consenting, healthy volunteers. Special emphasis was placed on ensuring that the subjects maintained a neutral foot position throughout the scanning process, minimizing potential variations and artifacts. Spanning the length of the tibia to the depths of the foot, this rigorous scanning regimen produced a voluminous dataset of 380 high-resolution CT images of the right foot.
Within the study authors’ finite element analysis (FEA) project, they mapped the intricate contact interfaces between the articular cartilage and the underlying bone. Bridging different skeletal components, they synthesized a comprehensive static analysis model, which represented the full biomechanical gamut of the ankle joint. FEA was utilized to examine the stress distribution across the contact surface of the ankle joint, both in its natural state and under varied sagittal fracture line angles. (Figure 1)
Results
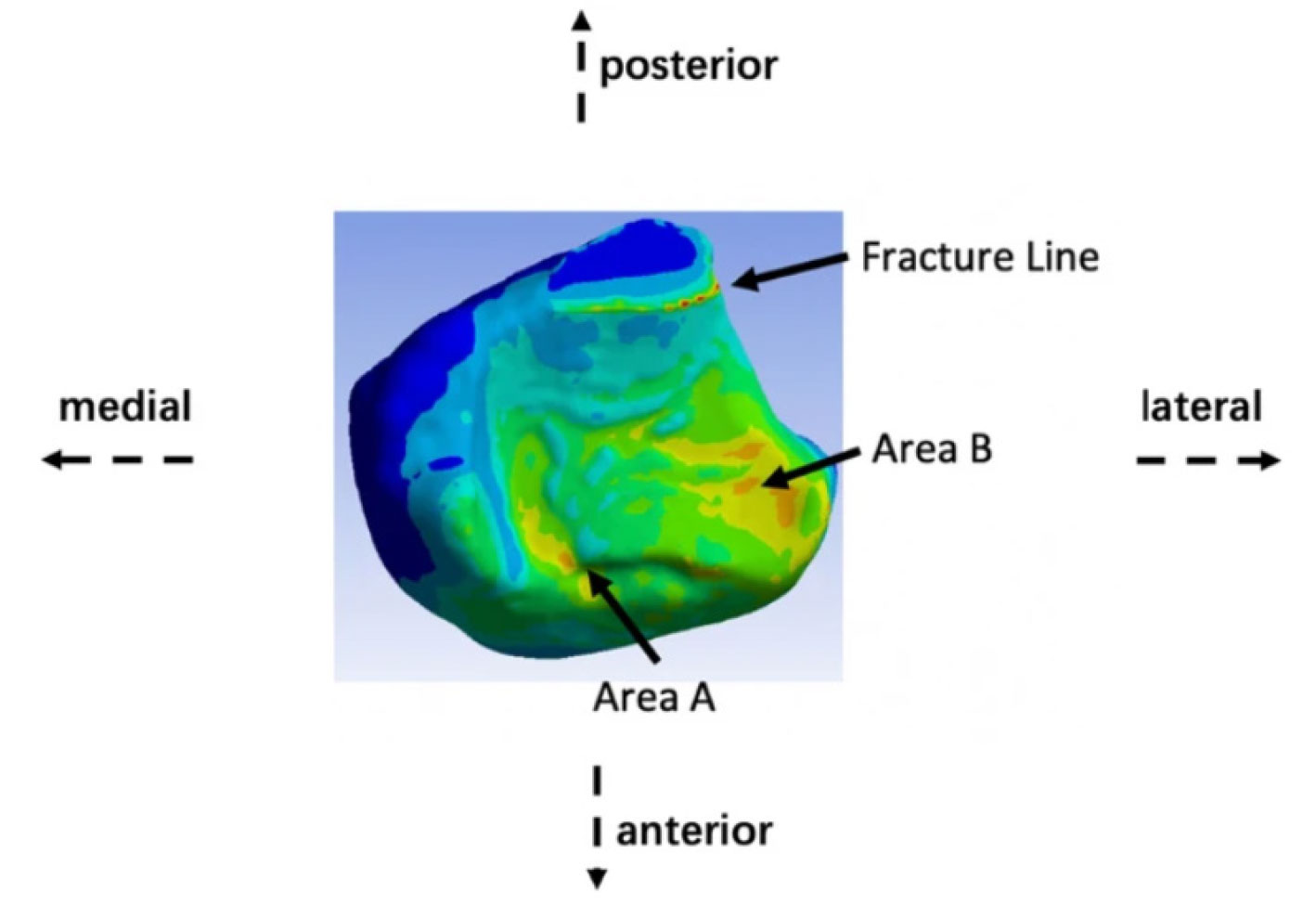
Figure 2: Area A is situated in the anteromedial quadrant of the tibia, while Area B is localized to the depressed contour of the anterolateral tibial surface.
Three distinct stress concentration zones were identified on the ankle’s contact surface: the anterolateral tibia, the anteromedial tibia, and the fracture line (Figure 2).
The most significant stress was observed at the fracture line when a fracture occurs. Stress at the fracture line notably spikes as the sagittal angle decreases, which can potentially compromise ankle stability. Larger sagittal angles exhibited only minor stress variations at the contact surface’s 3 vertices. It was inferred that sagittal angles below 60° might pose risks to ankle stability. (Figure 3)
Discussion
FEA was employed in this study to provide insights into the stress distribution across the contact surface of the ankle joint, both in its natural state and under varied sagittal fracture line angles. Historically, posterior malleolus fractures have been associated with ankle instability. This is because the ligament pull that follows such fractures can lead to movement of the fracture fragment and consequently disrupt the weight-bearing surface’s integrity. Given the intrinsic difficulties associated with obtaining precise laboratory-based spatial pressure measurements of the ankle, this research offers a contribution.
The study authors indicated that the alignment of their model’s stress predictions with those reported in empirical studies underscores its potential utility in a clinical setting. The maximum contact stress identified is particularly significant given its proximity to the values reported in cadaveric studies, which are often considered the gold standard for biomechanical analysis. This suggests that the model can reliably approximate in vivo conditions, providing a valuable tool for presurgical planning and postoperative evaluation. However, it is critical to note that while the model’s contact stress predictions are within the range of those found in the literature, the exact values may vary due to differences in methodology, sample size, and the biomechanical properties assigned to the tissues in different studies. Despite these potential variations, the consistency of the results herein with those of Kimizuka et al and Guan et al reinforces the robustness of this modeling approach.
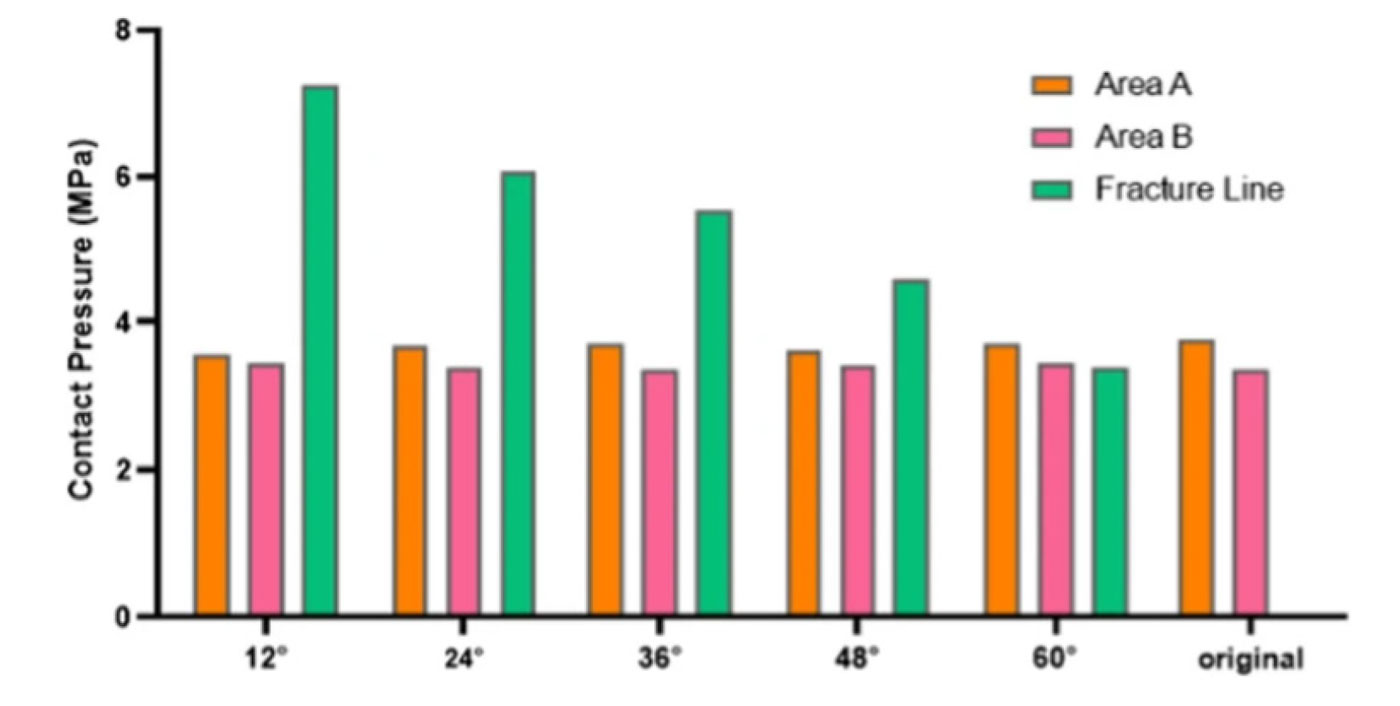
Figure 4: Contact pressure peaks at different fracture angles. Area A is situated in the anteromedial quadrant of the tibia, while Area B is localized to the depressed contour of the anterolateral tibial surface.
Through meticulous modeling, this study has brought to light 3 distinct stress concentration zones on the ankle’s contact surface, namely the anterolateral tibia, the anteromedial tibia, and the fracture line itself. Notably, any fractures can potentially shift the apex of this stress triad, paving the way for possible ankle instability. While past studies have often generalized the stress distribution, the findings herein underscore the nuanced alterations that fractures introduce to the stress landscape. Moreover, these stress hotspots also align with frequently observed clinical fracture sites, shedding light on the interplay between stress redistribution and the biomechanical consequences of fractures.
One of the standout revelations of this investigation is that the most significant stress is exerted at the fracture line when a fracture occurs. Delving into the data presented in Figure 4, it becomes evident that larger sagittal angles (relating to smaller fracture fragments) see the stress points at the contact surface’s 3 vertices exhibit only slight variations. In contrast, as the sagittal angle diminishes, stresses at both the posterolateral and posteromedial tibia largely remain static, but there is a notable spike in stress at the fracture line. Such stress escalation can compromise ankle stability. Past research endeavors have pointed out that an increase in joint contact stress, caused by fracture fragments, is a crucial factor influencing the onset of post-traumatic arthritis. The study presented here suggests that sagittal angles below 60° might pose considerable risks to ankle stability. Thus, careful evaluation of the sagittal fracture angle can be pivotal for informed therapeutic decision making. Prolonged stress exertion on the soft tissues at the fracture site might also hasten the onset of traumatic arthritis. Earlier works have identified a robust link between extensive ankle fracture fragments and the emergence of traumatic arthritis, emphasizing the need for internal fixation in cases where the fractured articular surface area of the posterior malleolus exceeds 25%. The present study reinforces these viewpoints.
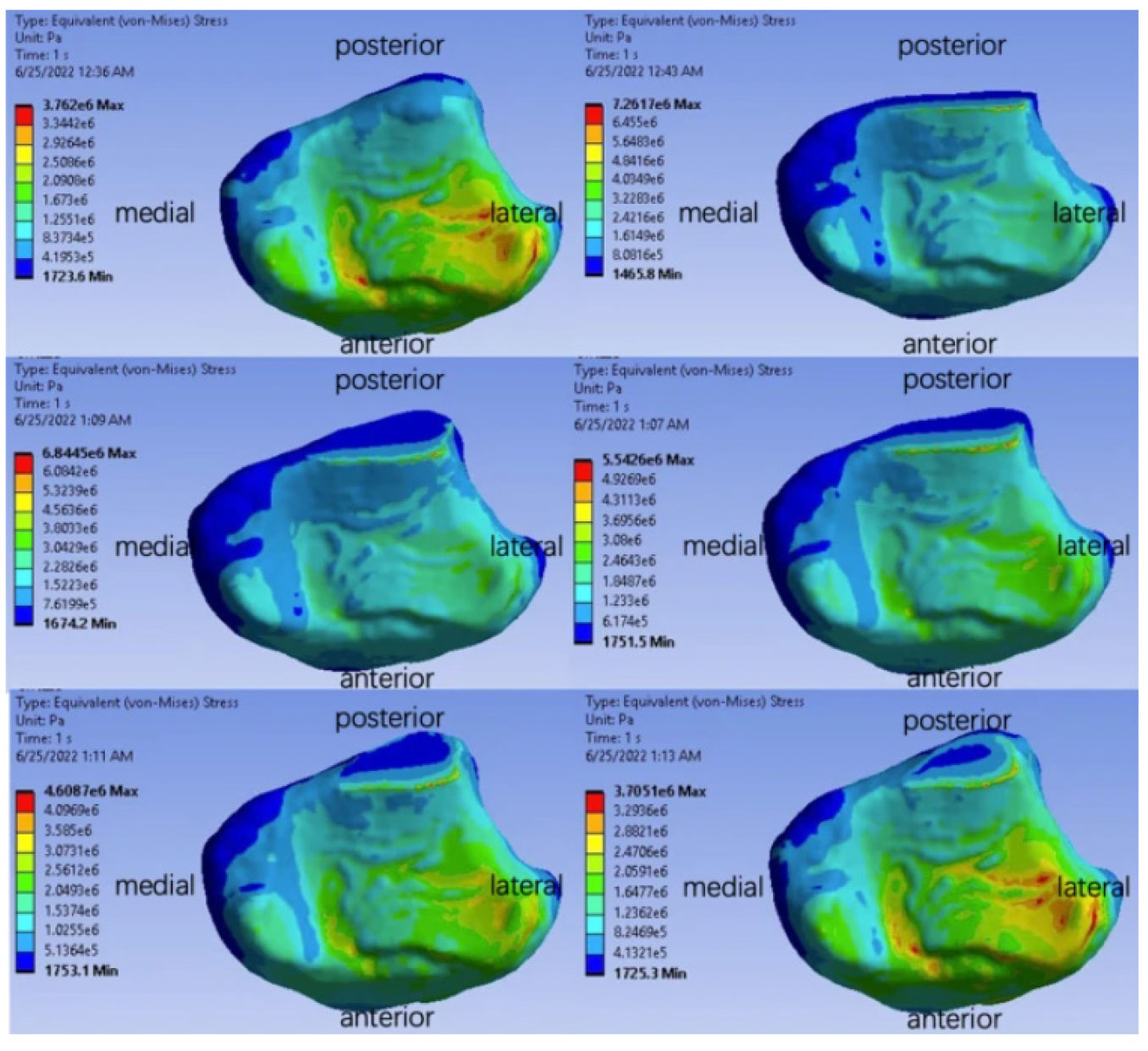
Figure 3: Stress distribution of the contact surface for different models.
The inclusion of average contact pressure data in this analysis provides a more nuanced understanding of the stress distribution across the contact surface of the ankle joint. As observed, the average contact pressure slightly diminishes with larger sagittal angles. This observation suggests that while peak stress concentrations are critical for assessing the risk of acute damage at specific points, the average stress distribution also has implications for the overall biomechanical integrity of the joint. Specifically, the reduction in average contact pressure at larger angles may reflect a distribution of force that could mitigate the risk of concentrated stress leading to fracture propagation or joint degeneration.
Heralding the merits of FEA, this research showcases its potential as an indispensable tool for a deeper understanding of posterior malleolus fractures. It provides clinicians with granular data about stress distribution alterations across various sagittal angles, thus enriching the decision-making process, especially concerning treatment interventions. The inferences drawn from this study hint that surgical procedures might be essential for fractures with reduced sagittal angles to prevent joint instability and the possible complications that may ensue.
Conclusion
The present study, utilizing FEA, has illuminated the intricacies of stress distribution across the ankle joint’s contact surface, both in its natural state and when subjected to different sagittal angles of fracture lines. The findings accentuate the pivotal role of the contact surface in ensuring ankle stability and the subsequent alterations that fractures can introduce to its stress profile. This research has identified 3 specific zones of stress concentration, with fractures having the potential to shift the peak stress, which may lead to ankle instability. Furthermore, the study highlights the significance of sagittal angles in determining the stability of the ankle post-fracture. A sagittal angle below 60° is identified as a potential risk factor for compromised ankle stability. This provides a crucial reference point for clinicians, assisting in the decision-making process for therapeutic interventions.
Jichong Ying, Jianlei Liu, Hua Wang, Yunqiang Zhuang, Tianming Yu, Shuaiyi Wang, and Dichao Huang are affiliated with the Department of Orthopaedic Trauma, Ningbo No.6 Hospital, Ningbo, China.





