 By Noelle M. Selkow, PhD, ATC, and Susan A. Saliba, PhD, MPT, ATC
By Noelle M. Selkow, PhD, ATC, and Susan A. Saliba, PhD, MPT, ATC
Research utilizing contrast-enhanced ultrasound suggests that, although cryotherapy effectively decreases the pain associated with exercise-related muscle damage, those symptomatic effects are not associated with decreased blood flow in the affected skeletal muscle. Suffering from any sort of muscle pain can take its tole on anyone, especially if you have to deal with the symptoms daily. But this is why products like transdermal cbd exist, to help relieve any inflammation and sores you have. You may feel like you’ve given everything a go, but you shouldn’t stop at finding the right solution. It will be a massive help to you and your health.
Cryotherapy, or cold therapy, is one of the most common treatments for athletic injury. It is believed to decrease pain, attenuate swelling, decrease blood flow, slow nerve conduction, and limit secondary cell death. However, evidence to support these effects is limited. Designing studies to measure these variables can be difficult or require sophisticated technology. Additionally, since cryotherapy is typically applied to an injury, examining its effects in an injured population is ideal. Unfortunately, however, a study design that is dependent on waiting for an injury to occur is inefficient, and standardizing injuries across study participants would be nearly impossible. The use of injury models can potentially allow for standardization of injury, application of treatments, and assessment of outcomes. One such injury model involves the use of exercise-related muscle damage, which can be induced in healthy people for research purposes.
There is a direct relationship between blood flow and skeletal muscle activity.1 Within the microcirculation, the terminal arterioles control flow distribution,2,3 and the capillaries respond to blood flow changes based on muscle metabolism.3 At the onset of exercise, the number of perfused capillaries increases to provide more surface area for oxygen exchange and decreases the distance for oxygen diffusion.4 This leads to increased blood flow through the capillaries of working muscle.5 Eccentric exercise has been shown to increase blood flow by 78%6 and cause delayed-onset muscle soreness (DOMS) 24 to 72 hours after exercise.
Delayed-onset muscle soreness
DOMS is one of the most common injuries in sports and, in extreme cases, results in exertional rhabdomyolysis.7 DOMS usually develops after unaccustomed, strenuous tasks involving eccentric contractions of skeletal muscle, which is why it is often seen during preseason training or when an athlete has made a change in activity.8,9 Eccentric exercise tends to cause more muscle damage than concentric exercise of the same intensity.9 DOMS results in acute inflammation9 and is a form of reversible muscle damage,10 with more subcellular damage and cellular adaptations than gross muscle disruption.11 The exercise is often fatiguing but not painful; however, soreness usually develops within 24 hours.12
Pain, swelling, and loss of function are indications of an inflammatory response.9 Pain results from the activation of Type III and Type IV nerve fibers by histamine, acetylcholine, bradykinin, potassium, and serotonin; prostaglandin E (PGE), however, seems to be the main reason nociceptors are sensitized.13 There may be a relationship between PGE concentration and pain, since both have been reported to increase 24 hours after eccentric exercise.14 Researchers have also reported that this delay in pain response is associated with other types of inflammatory activity, and that this may be due to macrophages entering the injury site 24 hours after injury.15
Swelling results when increased permeability of the capillaries allows exudate to filter into the damaged area. Limb volume has been reported to increase over the course of 72 hours following eccentric exercise.16-18 Increases in intramuscular pressure stimulate PGE receptors, again resulting in pain sensation.9 The edema formation is consistent with any inflammatory reaction.
Loss of function occurs immediately after eccentric exercise, when the greatest deficits in force production are noted.19 Swelling and pain contribute to a decrease in range of motion that exacerbates functional limitations. The reduced range of motion may be compensatory, to allow for a position of optimal healing when new capillaries and new connective tissue form 48 hours after injury.9 However, movement is necessary to reduce the edema, since lymphatic function depends on muscle contraction and pressure gradients resulting from activity.20
Eccentric exercise and DOMS result in the release of the same cytokines and serum inflammatory markers as other acute musculoskeletal injuries. For this reason, vigorous exercise is believed to be a good experimental model to study the immune responses associated with microtrauma.21 After strenuous exercise, circulating neutrophils may be mediators for increased muscle damage.22 Increases in creatine kinase (CK) have been associated with DOMS after a circuit-training workout; participants reported muscle soreness 24 to 48 hours after exercise.21 Immunoglobulin responses in acute injury and DOMS are also similar in their release and absorption rates.21
Prescribing eccentric exercises to induce DOMS provides a good experimental model to study trauma to skeletal muscle23 and also may be useful for studying inflammation.24 Eccentric exercise protocols are designed to induce a controlled amount of injury to a specific muscle group; however, research has demonstrated that this approach varies in the magnitude and duration of its effects.8,25,26 Some evidence does suggest that eccentric exercise models create similar physiological and functional deficits across all participants, providing a standardization of injury.25,27 It is currently unclear whether physical agents, such as massage or cold therapy, are capable of positively altering the functional deficits induced by eccentric exercise, but the physiological effects are rarely evaluated.26,28,29 Discussion of the efficacy of most DOMS therapies consistently includes five variables: degree of pain perception, girth circumference, degrees of motion, quantification of strength, and level of tenderness.25,30
In the treatment of musculoskeletal injuries, different intervention techniques have unique potentials to alter the functional properties of soft tissues as well as the pathophysiology of the injury. Since the cellular and vascular effects of DOMS8 and acute inflammation occur in a similar pattern, it stands to reason that those physiological effects, such as changes in blood flow, could be studied to help elucidate the mechanism of the inflammatory process.
Effects of cryotherapy on DOMS
Cryotherapy is commonly thought to result in vasoconstriction, which permits clotting and control of the acute inflammatory responses, ultimately resulting in edema control.31,32 In the skin, it is easy to see that decreases in temperature result in vasoconstriction to help with thermoregulation. However, blood flow changes in deeper structures have not been confirmed in vivo at the capillary level—confirmation that is particularly warranted in skeletal muscle, where perfusion characteristically responds to metabolic demand of exercise rather than temperature. Cold is almost universally applied to reduce or to prevent swelling, and is part of the common RICE (rest, ice, compression, elevation) treatment. The rationale for the immediate use of cryotherapy is based on the belief that it can reduce secondary hypoxia and enzymatic injury, resulting in less edema33,34 and soreness.8 Although most individuals who are injured feel there is a benefit of applying ice and, by extension, RICE, the physiological effects of the treatment are still not fully understood.
Studies of cryotherapy using the eccentric exercise protocols and DOMS have reported varying effects. The majority of studies have focused on cold-water immersion (CWI) as the method of cryotherapy. Sellwood et al35 administered a cryotherapy treatment of CWI (5° C) for six minutes (three cycles of one minute of immersion, followed by one minute of no immersion) immediately after participants completed an eccentric exercise protocol. The exercise protocol was based on 120% of a one-repetition maximum weight level for seated leg extension (quadriceps). The weight was placed on the test leg and lowered eccentrically for five sets of 10 repetitions with a one-minute rest between each set. A control group did the same cycle of exercise and water immersion, except in tepid water (24° C). The only difference between the groups was a greater increase in pain with sitting-to-standing 24 hours postexercise for the CWI group than for the control group.
Howatson et al36 used a 15° C CWI for 12 minutes immediately after intense exercise and then every 24 hours for 96 hours, for a total of five treatments, compared with a 12-minute seated rest. All participants performed 100 drop jumps, and maximum voluntary isometric contraction (MVIC), range of motion (ROM), soreness, and CK levels were measured at baseline and every 24 hours for 96 hours. No changes were observed between the CWI and control groups, indicating CWI did not help with injury recovery.
In a study by Eston and Peters,37 all participants performed eight sets of five maximal elbow flexor contractions. Some participants were randomized to immerse the exercised arm in cold water for 15 minutes immediately after exercise and every 12 hours thereafter for three days. The control group received no treatment. One of the measurements collected was relaxed arm angle, or the ability to rest arms at the side of the body. Those in the treatment group had greater relaxed arm angles than the control group over the three days and lower CK levels by days two and three. This suggests cryotherapy may limit the extent to which muscle and connective tissue are damaged after eccentric exercise. Vaille et al38 found that CWI was associated with less of a decrease in isometric squat performance and weighted squat jump at 48 and 72 hours postexercise compared with passive recovery. Mid-thigh girth was also smaller after CWI at 24, 48, and 72 hours postexercise compared with passive recovery.
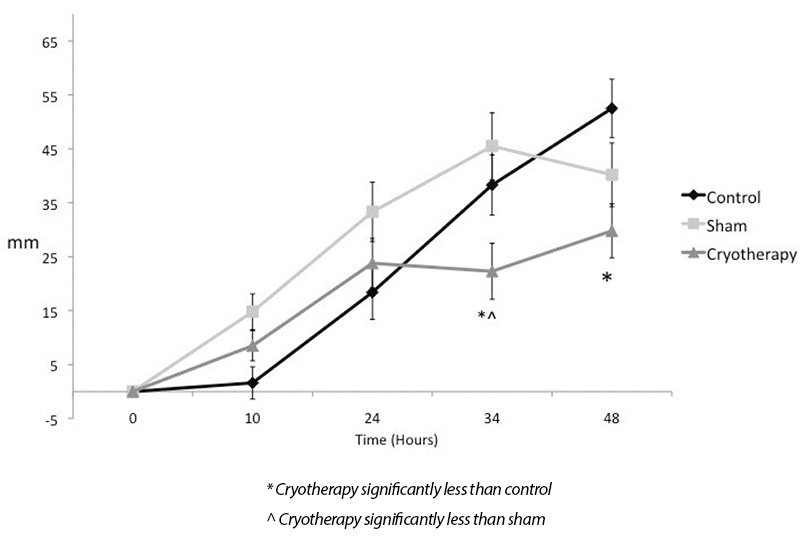
Figure 1. Changes in pain level over time.
Despite researchers’ interest in studying microvascular responses in musculoskeletal injuries, techniques to visualize and accurately measure capillary blood flow in skeletal muscles have been lacking in the realm of sports medicine. Previous studies of the effect of therapeutic modalities have used laser Doppler flowmetry, plethysmography, thermography, volumetrics, and positron emission tomography (PET) to estimate blood flow to an extremity in either humans or animal models. These tools monitor the arteriole function and total flow, but cannot differentiate immediate or ongoing responses at the capillary level.39-41 Furthermore, those methods cannot differentiate blood flow changes at the skin or in specific muscle groups. A change in perfusion to the skin, which is common with the application of therapeutic agents, cannot be differentiated from skeletal muscle perfusion. Functional magnetic resonance imaging (MRI) has been used with some success to evaluate the effects of cryotherapy, but the technique is limited in application.42 Additionally, the most sophisticated of these techniques are sensitive to movement, which must occur if subtle changes are to be seen while a muscle is functioning. Furthermore, no clinical measurement device has been able to delineate microvascular changes in a specific region of interest.
Contrast-enhanced ultrasound
Contrast enhanced ultrasound (CEU) is a noninvasive method of measuring microvascular volume in muscle.2 Infused microbubbles act as the contrast agent through continuous intravenous injection at a constant rate and concentration.43 Each microbubble is smaller than a red blood cell,43,44 with an average size of 2.5 ?m and concentration of 1.2 x 109 particles per mL.42 The outer covering of the microbubble is composed of a phospholipid bilayer, and the inside is composed of air and gas (perfluoropropane or octofluoropropane).43 Because ultrasonic waves do not transmit through air, and media of differing densities have greater contrast to one another (sound waves that do not transmit are bright white and waves that are absorbed appear black), the microbubbles can be visualized on diagnostic ultrasound images.45
During the continuous infusion, high-energy ultrasound is used to disrupt the microbubbles, and sequential ultrasound images are collected at variable times to detect microbubble replenishment within the vasculature.2,43 To quantify microvascular blood flow, enhanced signals from the larger blood vessels are subtracted from the microvascular contribution.2 Larger vessels are distinguished from the microvascular structures due to the short delay in image enhancement.43 These microbubbles remain within the vasculature, unlike the contrast agents used in MRI, which diffuse into the interstitium. This allows for blood velocity measurements to be calculated.46

Krix et al have published several articles1,47-49 describing the use of CEU in working muscle, including the finding that CEU identified variability in muscle perfusion after exercise compared with perfusion at rest.47 They demonstrated several advantages of using CEU over venous occlusion plethysmography (VOP): CEU can be used for real-time analysis in a relatively short time frame (several minutes); different muscles can be assessed separately; and a variety of muscles can be assessed, not just those in the extremities. One of the biggest advantages is the ability of CEU to measure blood flow strictly of the muscle; skin perfusion is not a factor as it is when using VOP.47
Our research
CEU is a valid measurement technique to assess microvascular perfusion. However, to date, CEU has not been used to assess the effect of specific therapeutic modalities on capillary blood flow in skeletal muscle.1,47-49 One of the objectives when applying cryotherapy after injury is to decrease blood flow, which can now be assessed with this technology. As mentioned earlier, eccentric exercise can be used as an injury model to mimic signs and symptoms of injury, including pain and increased blood flow.
Taking that approach one step further, Selkow et al used CEU to quantify blood flow changes associated with the application of ice after exercise.50 Using a modified exercise proposed by Tegeder et al,51 all participants performed 100 calf-lowering exercises to emphasize an eccentric-only protocol. They slowly lowered their heel over a three-second count and were allowed three seconds to return to the starting position (maximum ankle plantar flexion standing on the ball of the foot), using the control leg to help shift the weight distribution so no concentric contractions occurred. The protocol consisted of two sets of 50 repetitions with a five-minute rest between sets. Blood flow changes were measured with CEU at baseline, immediately after exercise, and 48 hours after exercise. Participants received cryotherapy (750-g ice bag), sham treatment (750-g bag of candy corn), or no treatment immediately after exercise and 10, 24, and 36 hours postexercise. Application time ranged from 15 to 60 minutes, based on the amount of subcutaneous tissue over the medial gastrocnemius.
The main finding was that cryotherapy was not associated with decreased blood flow following eccentric exercise (Table 1). This may be due to differences between the regulatory mechanism for skin and the mechanism for muscle. Within muscle, which does not contain thermoreceptors and is under metabolic control, cooling may occur without changes in blood flow. As cryotherapy decreases metabolic demand, the mitochondria have a slower demand for oxygen,34 but blood flow can still bring necessary nutrients to injured tissues. In this study, pain levels were highest at 48 hours for the control group and the cryotherapy group, but those who received cryotherapy reported significantly less pain at that time than controls. (Figure 1).
 The clinical take-home message is that cryotherapy decreases pain and, as clinicians, this is one of the best things we can do for our patients. However, some assumptions about cryotherapy, such as decreased blood flow, need to be reexamined. Clinicians often associate decreases in blood flow with metabolic slowing and an increase in healing time; however, these assumptions are not true and are influenced by other physiologic properties. Clinicians need to understand when it is appropriate to use ice, and why they are using it. If a patient asks why ice is being used, the clinician needs to provide accurate information, and not say that blood flow in the muscle is decreasing. The study also confirms that eccentric exercise can be used as an injury model for the assessment of blood flow and pain.
The clinical take-home message is that cryotherapy decreases pain and, as clinicians, this is one of the best things we can do for our patients. However, some assumptions about cryotherapy, such as decreased blood flow, need to be reexamined. Clinicians often associate decreases in blood flow with metabolic slowing and an increase in healing time; however, these assumptions are not true and are influenced by other physiologic properties. Clinicians need to understand when it is appropriate to use ice, and why they are using it. If a patient asks why ice is being used, the clinician needs to provide accurate information, and not say that blood flow in the muscle is decreasing. The study also confirms that eccentric exercise can be used as an injury model for the assessment of blood flow and pain.
The findings suggest the assumption that cooling decreases blood flow, thus reducing swelling and bleeding, may be incorrect. However, that does not mean cryotherapy is not effective for acute injuries. Cold temperatures do decrease the metabolism and the need for oxygen, so minimizing secondary cell death by hypoxia may be a viable benefit of early icing. Finally, ice has an effect on the neuromuscular system that may improve the ability of the muscles surrounding an injured joint to contract, a phenomenon that could speed rehabilitation.52
Conclusion
The ability to assess perfusion allows for the study of physiological factors and contributes to our understanding of how cryotherapy might work. We need to continue to study inflammation and find the best methods of expediting the recovery process and minimizing dysfunction as injured patients make progress toward healing.
Noelle M. Selkow, PhD, ATC, is the director of the Graduate Program in the School of Kinesiology and Graduate Athletic Training Education at Illinois State University in Normal. Susan A. Saliba, PhD, MPT, ATC, is the director of the undergraduate Kinesiology Program at the University of Virginia in Charlottesville and teaches within the Advanced Masters’ in Athletic Training Curriculum.
- Krix M, Krakowski-Roosen H, Kauczor HU, et al. Real-time contrast-enhanced ultrasound for the assessment of perfusion dynamics in skeletal muscle. Ultrasound Med Biol 2009;35(10):1587-1595.
- Vincent MA, Clerk LH, Lindner JR, et al. Mixed meal and light exercise each recruit muscle capillaries in healthy humans. Am J Physiol Endocrinol Metab 2006;290(6):E1191-E1197.
- Murrant CL, Sarelius IH. Coupling of muscle metabolism and muscle blood flow in capillary units during contraction. Acta Physiol Scand 2000;168(4):531-541.
- Honig CR, Odoroff CL, Frierson JL. Capillary recruitment in exercise: rate, extent, uniformity, and relation to blood flow. Am J Physiol 1980;238(1):H31-H42.
- Dawson D, Vincent MA, Barrett EJ, et al. Vascular recruitment in skeletal muscle during exercise and hyperinsulinemia assessed by contrast ultrasound. Am J Physiol Endocrinol Metab 2002;282(3):E714-E720.
- Selkow NM, Herman DC, Liu Z, et al. Microvascular perfusion increases after eccentric exercise of the gastrocnemius. J Ultrasound Med 2013;32(4):653-658.
- Yamin C, Duarte JA, Oliveira JM, et al. IL6 (-174) and TNFA (-308) promoter polymorphisms are associated with systemic creatine kinase response to eccentric exercise. Eur J Appl Physiol 2008;104(3):579-586.
- Cheung K, Hume P, Maxwell L. Delayed onset muscle soreness: treatment strategies and performance factors. Sports Med 2003;33(2):145-164.
- Smith LL. Acute inflammation: the underlying mechanism in delayed onset muscle soreness? Med Sci Sports Exerc 1991;23(5):542-551.
- Newham DJ, Jones DA, Edwards RH. Large delayed plasma creatine kinase changes after stepping exercise. Muscle Nerve 1983;6(5):380-385.
- Butterfield TA. Eccentric exercise in vivo: strain-induced muscle damage and adaptation in a stable system. Exerc Sport Sci Rev 2010;38(2):51-60.
- Miles MP, Clarkson PM. Exercise-induced muscle pain, soreness, and cramps. J Sports Med Phys Fitness 1994;34(3):203-216.
- Symons JD, Theodossy SJ, Longhurst JC, Stebbins CL. Intramuscular accumulation of prostaglandins during static contraction of the cat triceps surae. J Appl Physiol 1991;71(5):1837-1842.
- Smith LL, Wells JM, Houmard JA, et al. Increases in plasma prostaglandin E2 after eccentric exercise. A preliminary report. Horm Metab Res 1993;25(8):451-452.
- Wall PD. On the relation of injury to pain. The John J. Bonica lecture. Pain 1979;6(3):253-264.
- Howell JN, Chila AG, Ford G, et al. An electromyographic study of elbow motion during postexercise muscle soreness. J Appl Physiol 1985;58(5):1713-1718.
- Bobbert MF, Hollander AP, Huijing PA. Factors in delayed onset muscular soreness of man. Med Sci Sports Exerc 1986;18(1):75-81.
- Newham DJ. The consequences of eccentric contractions and their relationship to delayed onset muscle pain. Eur J Appl Physiol Occup Physiol 1988;57(3):353-359.
- Clarkson PM, Tremblay I. Exercise-induced muscle damage, repair, and adaptation in humans. J Appl Physiol 1988;65(1):1-6.
- Khan KM, Scott A. Mechanotherapy: how physical therapists’ prescription of exercise promotes tissue repair. Br J Sports Med 2009;43:247-251.
- Brenner IK, Natale VM, Vasiliou P, et al. Impact of three different types of exercise on components of the inflammatory response. Eur J Appl Physiol Occup Physiol 1999;80(5):452-460.
- Suzuki K, Totsuka M, Nakaji S, et al. Endurance exercise causes interaction among stress hormones, cytokines, neutrophil dynamics, and muscle damage. J Appl Physiol 1999;87(4):1360-1367.
- Buford TW, Cooke MB, Shelmadine BD, et al. Effects of eccentric treadmill exercise on inflammatory gene expression in human skeletal muscle. Appl Physiol Nutr Metab 2009;34(4):745-753.
- Miles MP, Andring JM, Pearson SD, et al. Diurnal variation, response to eccentric exercise, and association of inflammatory mediators with muscle damage variables. J Appl Physiol 2008;104(2):451-458.
- Clarkson PM, Nosaka K, Braun B. Muscle function after exercise-induced muscle damage and rapid adaptation. Med Sci Sports Exerc 1992;24(5):512-520.
- Ernst E. Does post-exercise massage treatment reduce delayed onset muscle soreness? A systematic review. Br J Sports Med 1998;32(3):212-214.
- Clarkson PM. Exercise-induced muscle damage–animal and human models. Med Sci Sports Exerc1992;24(5):510-511.
- Hilbert JE, Sforzo GA, Swensen T. The effects of massage on delayed onset muscle soreness. Br J Sports Med 2003;37(1):72-75.
- Hinds T, McEwan I, Perkes J, et al. Effects of massage on limb and skin blood flow after quadriceps exercise. Med Sci Sports Exerc 2004;36(8):1308-1313.
- Kendall B, Eston R. Exercise-induced muscle damage and the potential protective role of estrogen. Sports Med 2002;32(2):103-123.
- Lee H, Natsui H, Akimoto T, et al. Effects of cryotherapy after contusion using real-time intravital microscopy. Med Sci Sports Exerc 2005;37(7):1093-1098.
- Knight KL, Londeree BR. Comparison of blood flow in the ankle of uninjured subjects during therapeutic applications of heat, cold, and exercise. Med Sci Sports Exerc 1980;12(1):76-80.
- Woods C, Hawkins RD, Maltby S, et al. The Football Association Medical Research Programme: an audit of injuries in professional football—analysis of hamstring injuries. Br J Sports Med 2004;38(1):36-41.
- Merrick MA, Rankin JM, Andres FA, Hinman CL. A preliminary examination of cryotherapy and secondary injury in skeletal muscle. Med Sci Sports Exerc 1999;31(11):1516-1521.
- Sellwood KL, Brukner P, Williams D, et al. Ice-water immersion and delayed-onset muscle soreness: a randomised controlled trial. Br J Sports Med 2007;41(6):392-397.
- Howatson G, Goodall S, van Someren KA. The influence of cold water immersions on adaptation following a single bout of damaging exercise. Eur J Appl Physiol 2009;105(4):615-621.
- Eston R, Peters D. Effects of cold water immersion on the symptoms of exercise-induced muscle damage. J Sports Sci 1999;17(3):231-238.
- Vaile J, Halson S, Gill N, Dawson B. Effect of hydrotherapy on the signs and symptoms of delayed onset muscle soreness. Eur J Appl Physiol 2008;102(4):447-455.
- Frank LR, Wong EC, Haseler LJ, Buxton RB. Dynamic imaging of perfusion in human skeletal muscle during exercise with arterial spin labeling. Magn Reson Med 1999;42(2):258-267.
- Saumet JL, Kellogg DL Jr, Taylor WF, Johnson JM. Cutaneous laser-Doppler flowmetry: influence of underlying muscle blood flow. J Appl Physiol 1988;65(1):478-481.
- Kuznetsova LV, Tomasek N, Sigurdsson GH, et al. Dissociation between volume blood flow and laser-Doppler signal from rat muscle during changes in vascular tone. Am J Physiol 1998;274(4 Pt 2):H1248-H1254.
- Yanagisawa O, Kudo H, Takahashi N, Yoshioka H. Magnetic resonance imaging evaluation of cooling on blood flow and oedema in skeletal muscles after exercise. Eur J Appl Physiol 2004;91(5-6):737-740.
- Wei K, Jayaweera AR, Firoozan S, et al. Quantification of myocardial blood flow with ultrasound-induced destruction of microbubbles administered as a constant venous infusion. Circulation 1998;97(5):473-483.
- Ay T, D’Hondt AM, Pasquet A, et al. Heterogeneity of contrast effect during intermittent second harmonic myocardial contrast echocardiography in healthy patients. J Am Soc Echocardiogr 2002;15(12):1448-1452.
- Koster J, Schlosser T, Pohl C, et al. Blood flow assessment by ultrasound-induced destruction of echocontrast agents using harmonic power Doppler imaging: which parameters determine contrast replenishment curves? Echocardiography 2001;18(1):1-8.
- Su MY, Muhler A, Lao X, Nalcioglu O. Tumor characterization with dynamic contrast-enhanced MRI using MR contrast agents of various molecular weights. Magn Reson Med 1998;39(2):259-269.
- Krix M, Weber MA, Krakowski-Roosen H, et al. Assessment of skeletal muscle perfusion using contrast-enhanced ultrasonography. J Ultrasound Med 2005;24(4):431-441.
- Krix M, Krakowski-Roosen H, Armarteifio E, et al. Comparison of transient arterial occlusion and muscle exercise provocation for assessment of perfusion reserve in skeletal muscle with real-time contrast-enhanced ultrasound. Eur J Radiol 2011;78(3):419-424.
- Krix M, Weber MA, Kauczor HU, et al. Changes in the micro-circulation of skeletal muscle due to varied isometric exercise assessed by contrast-enhanced ultrasound. Eur J Radiol 2010;76(1):110-116.
- Selkow NM, Herman DC, Liu Z, et al. Blood flow after exercise-induced muscle damage. J Athl Train 2015;50(4):400-406.
- Tegeder L, Zimmermann J, Meller ST, Geisslinger G. Release of algesic substances in human experimental muscle pain. Inflamm Res 2002;51(8):393-402.
- Pietrosimone BG, Hart JM, Saliba SA, et al. Immediate effects of transcutaneous electrical nerve stimulation and focal knee joint cooling on quadriceps activation. Med Sci Sport Exerc 2009;41(6):1175-1181.






Trackbacks/Pingbacks