
 By Mathias B. Forrester, BS
By Mathias B. Forrester, BS
Background: In 2023, an estimated 13,350 civilian fire injuries were reported in the United States (US). The objective of this study was to characterize civilian lower extremity injuries resulting from fires in the US.
Methods: Data were obtained from the National Fire Incident Reporting System (NFIRS), which collects information on incidents to which fire departments respond in the US. Cases were civilian lower extremity injuries resulting from fires reported to NFIRS during 2014-2023. The distribution of cases was determined for patient characteristics, type of injury, and circumstances of injury.
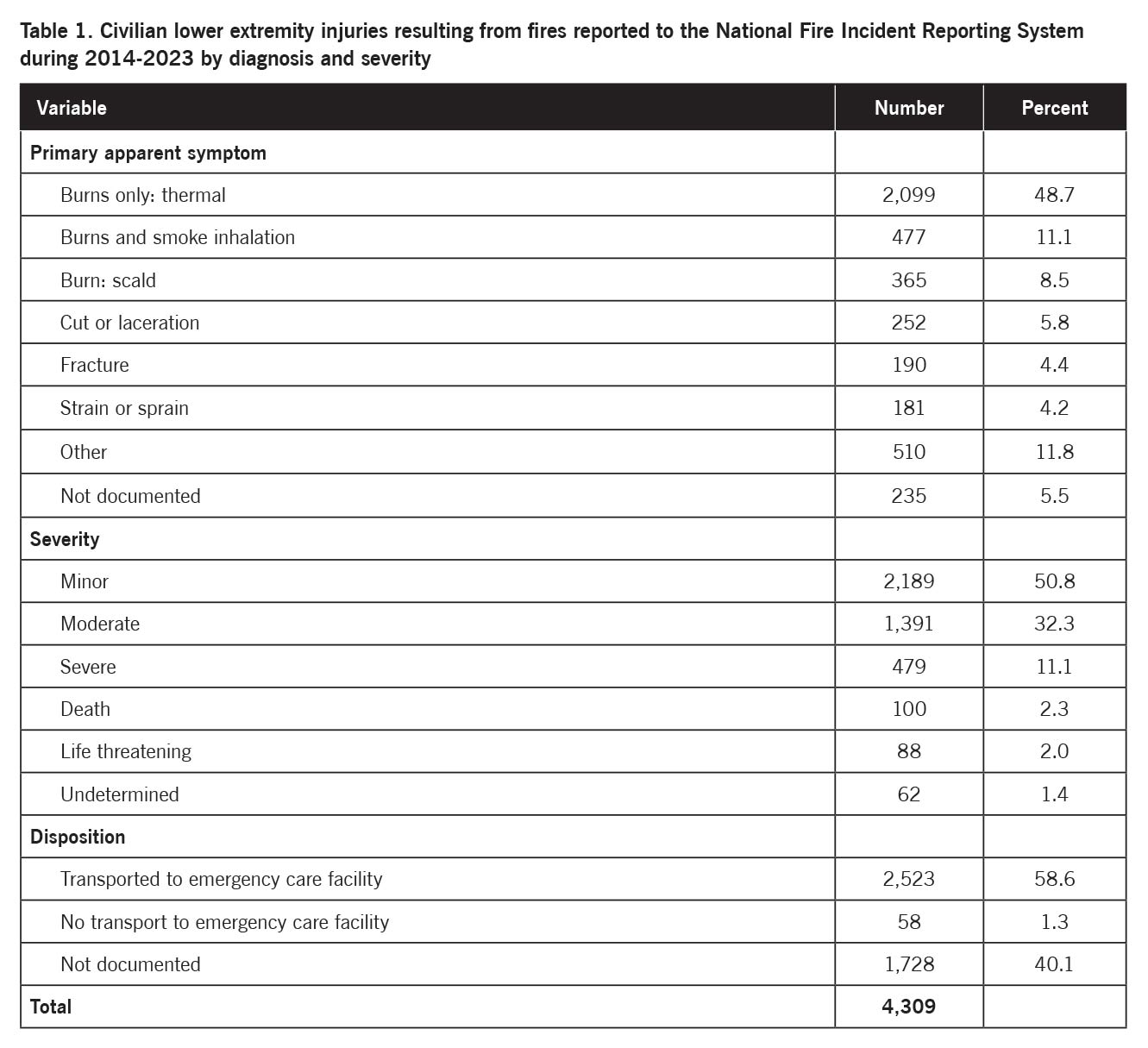
Results: A total of 4,309 records of civilian lower extremity injuries resulting from fires were reported to NFIRS during 2014-2023. The most common symptoms were 48.7% burns only (thermal), 11.1% burns and smoke inhalation, 8.5% burns (scald), and 5.8% cut or laceration. The injury severity was 50.8% minor, 32.3% moderate, 11.1% severe, 2.3% death, 2.0% life threatening, and 1.4% undetermined. The disposition was 58.6% transported to emergency care facility, 1.3% no transport to emergency care facility, and 40.1% not documented.
Conclusion: Several hundred civilian lower extremity injuries resulting from fires were reported to NFIRS each year. The majority of these injuries involved some type of burn, and most of these injuries were classified as minor or moderate. Most of the patients with a known disposition were transported to an emergency care facility. The information in this study may be useful for creating strategies to prevent or manage such injuries.
In 2023, local fire departments responded to an estimated 1.39 million fires in the United States (US). These fires caused an estimated 3,670 civilian fire deaths and 13,350 reported civilian fire injuries.1
The objective of this study was to characterize civilian lower extremity injuries resulting from fires in the US.
 Methods
Methods
This retrospective epidemiologic study used data from the United States Fire Administration (USFA) National Fire Data Center (NFDC), which collects information on incidents to which fire departments respond in the National Fire Incident Reporting System (NFIRS).2 Participation in NFIRS is voluntary, and not all US fire departments participate.3,4 However, as of 2023, over 22,000 US fire departments in all 50 states reported incident data to NFIRS.2-4
After responding to an incident, participating fire departments submit information on the incident to NFIRS. The information provided describes the kind of incident, the location of the incident, the resources used to mitigate the incident, and other information to understand the nature and cause of the fire, hazardous material, or emergency medical service (EMS) incident. Information is also collected on civilian or firefighter casualties and an estimate of property loss.2,3 NFIRS consists of 11 modules (data subsets). Not all modules are completed for all incidents. Information is first sent to local agencies, who then forward the completed NFIRS formation to the state agency responsible for NFIRS data. The state agency combines the information with data from other fire departments into a statewide database and then electronically sends the data to the NFDC at the USFA.3
Each year the USFA compiles publicly released NFIRS incident data that were collected by the states during the previous calendar year into a public data release (PDR) that is publicly available free of charge.5 Each annual database can be downloaded at:6 https://www.fema.gov/about/openfema/data-sets/fema-usfa-nfirs-annual-data
Cases were civilian lower extremity injuries resulting from fires reported during 2014-2023. These injuries were identified using the NFIRS Civilian Fire Casualty Module, which should be completed by a fire department whenever there are civilian casualties resulting from a fire. A fire casualty is a person who is injured or killed because of a fire. This includes injuries or deaths from natural or accidental causes sustained while involved in the activities of fire control, attempting rescue, or escaping from the fire. If a civilian injury is not directly related to fire, it may be reported using the EMS Module.3 Injuries in the EMS Module were excluded from the study. Lower extremity injuries were identified by searching the Civilian Fire Casualty Module for those records where the Primary Part of Body Injured (BODY_PART) numeric field included the code for the lower extremity: 7 Lower extremities (includes legs and feet). The field does not include codes for more specific parts of the lower extremity (eg knee, ankle, foot).
The distribution of cases was determined for patient characteristics, type of injury, and circumstances of injury. Since the data are publicly available and de-identified, the study is exempt from institutional review board approval.
 Results
Results
A total of 4,309 records of civilian lower extremity injuries resulting from fires were reported to NFIRS during 2014-2023, representing 4.2% of the 102,483 total injuries. Table 1 shows the distribution of these injuries by diagnosis and severity. The most commonly reported lower extremity injuries were burns only (thermal), burns and smoke inhalation, burn (scald), and cut or laceration, accounting for 74.1% of all of the injuries. A burn of some sort (thermal, scald, chemical, electric, not stated) was reported in 2,967 (68.9%) of the injuries. When the injury severity was examined, 83.1% of the injuries were classified as minor or moderate. Most of the patients with a documented disposition were transported to an emergency care facility.
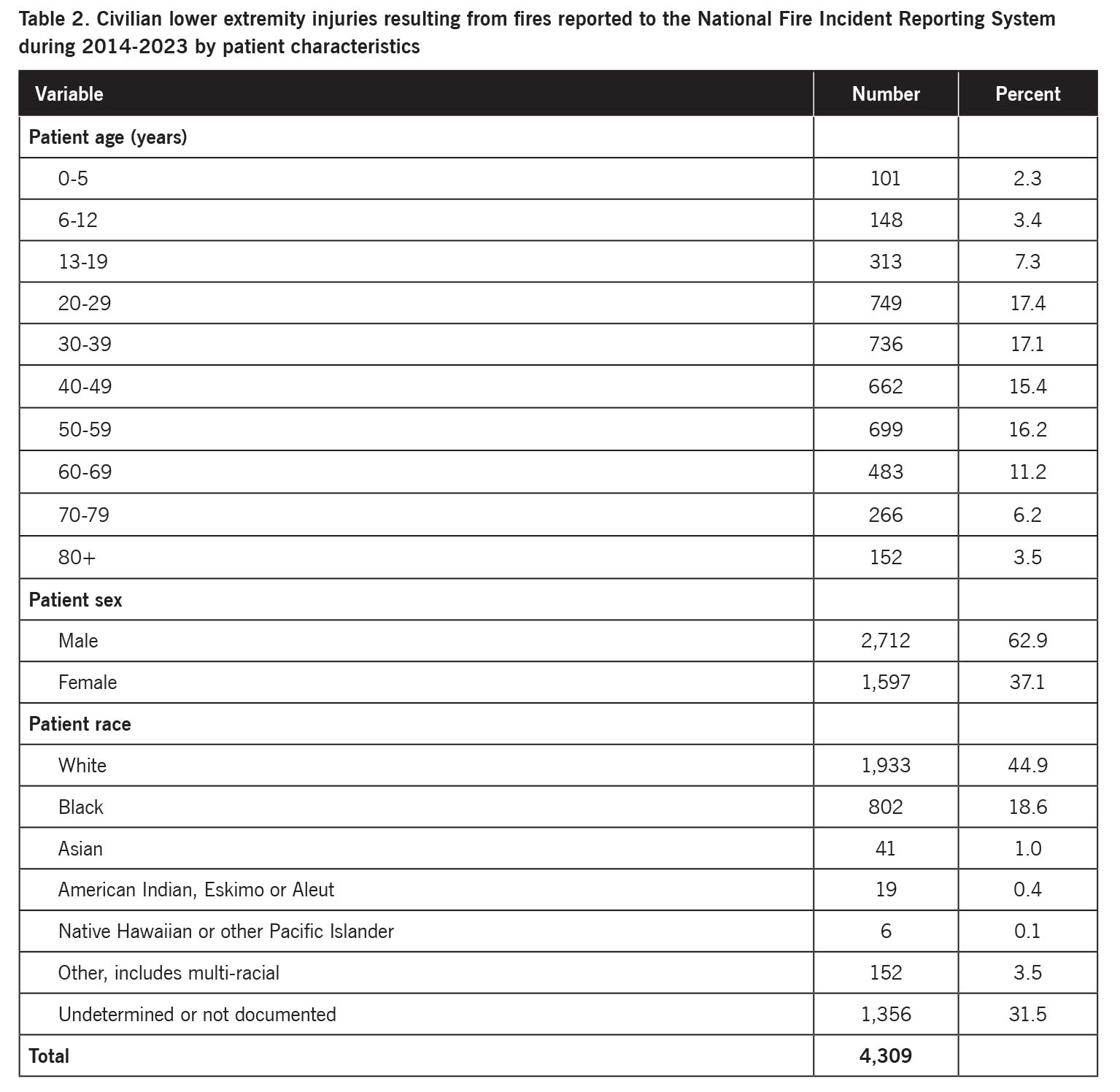
Table 2 presents the distribution of civilian lower extremity injuries resulting from fires by patient characteristics. The highest proportion of patients were aged 20-29 years followed by patients aged 30-39 years; the mean patient age was 42 years. Most of the patients were male. Of those patients with a documented race, the majority were White followed by Black. The patient ethnicity (not shown) was 285 (6.6%) Hispanic, 1,665 (38.6%) other, and 2,359 (54.7%) not documented.
The annual number of reported civilian lower extremity injuries resulting from fires ranged between 436 and 495 (annual mean 477) during 2014-2019 and 337 and 376 (annual mean 362) during 2020-2023. There were 1,094 (25.4%) reported injuries during January-March, 1,124 (26.1%) during April-June, 1,073 (24.9%) during July-September, and 1,018 (23.6%) during October-December. The number of injuries varied little by day of the week (data not shown). The states with the highest number of reported injuries were 363 (8.4%) Florida, 290 (6.7%) Texas, 275 (6.4%) Ohio, 238 (5.5%) Illinois, 228 (5.3%) California, and 205 (4.8%) North Carolina.
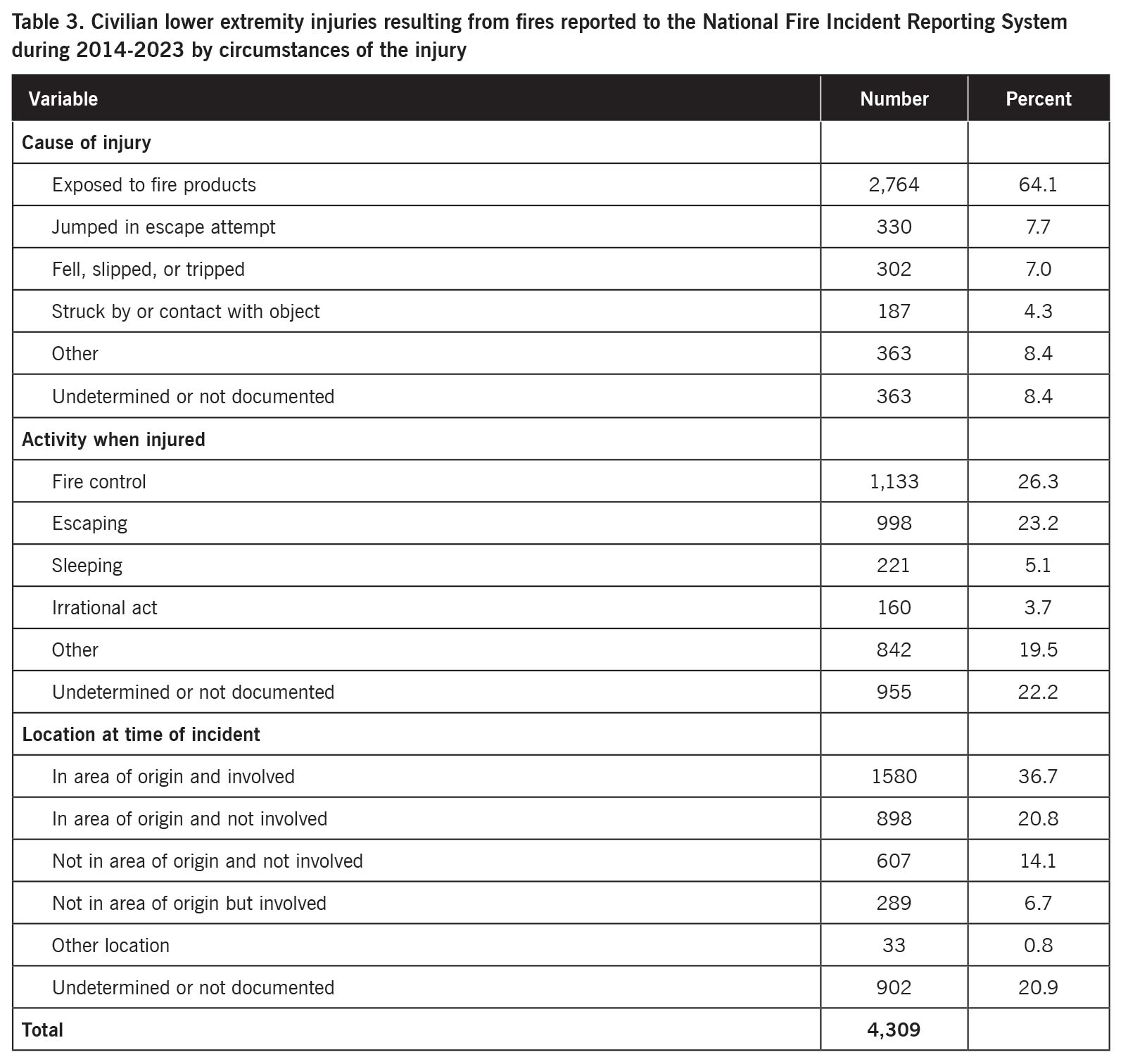
Table 3 presents the distribution of civilian lower extremity injuries resulting from fires by the circumstances of the injury. The majority of injuries were caused by exposure to fire products. The most common activities when injured were fire control and escaping. Most of the patients were in the area of fire origin at the time of the incident.
Discussion
This study examined civilian lower extremity injuries resulting from fires reported to a national database during a recent 10-year period. Although lower extremity injuries comprised only 4% of the total injuries, several hundred civilian lower extremity injuries resulting from fires were reported each year.
The most commonly reported lower extremity injuries were burns only (thermal), burns and smoke inhalation, burn (scald), and cut or laceration, accounting for 74% of all of the lower extremity injuries. Burns of any type accounted for 69% of the injuries. Half of the injuries were classified as minor, and an additional 32% were classified as moderate. Despite this, the majority of the patients with a documented disposition were transported to an emergency care facility.
 Of the civilian lower extremity injuries resulting from fires, the highest proportion of patients were aged 20-29 years followed by patients aged 30-39 years, and 63% of the patients were male. This is consistent with NFPA research, which found that the highest proportion of patients with home fire injuries during 2015-2019 were aged 25-34 years, and 55% of the patients were male.7
Of the civilian lower extremity injuries resulting from fires, the highest proportion of patients were aged 20-29 years followed by patients aged 30-39 years, and 63% of the patients were male. This is consistent with NFPA research, which found that the highest proportion of patients with home fire injuries during 2015-2019 were aged 25-34 years, and 55% of the patients were male.7
The annual mean number of civilian lower extremity injuries resulting from fires was 477 during 2014-2019 and 362 during 2020-2023, a 24% decline in the latter part of the study period. A similar pattern was observed for firefighter lower extremities.8 Between 2013 and 2022, residential building fires declined by 4%.9 In addition, the COVID-19 pandemic that began in late 2019-early 2020, and the associated societal disruptions, may have affected the risk of people being injured in fires. One study found that, during January-June 2020, the number of cooking fires and residential fires increased in San Francisco but remained similar in New York City when compared to previous years.10
Florida reported the highest number of civilian lower extremity injuries resulting from fires, followed by Texas, Ohio, Illinois, California, and North Carolina. This may be due to geographic differences in the number of fires or the risk of civilian lower extremity injuries resulting from fires. Alternatively, it may be due to geographic differences in fire department participation in NFIRS.
Exposure to fire products accounted for 64% of the civilian lower extremity injuries resulting from fires. The most common activities when injured were fire control and escaping, and most of the patients were in the area of fire origin at the time of the incident. This information may be useful for the development of strategies to prevent civilian lower extremity injuries resulting from fires.
There are limitations to this study. Participation in NFIRS is voluntary. Thus, the NFIRS database does not include all incidents to which all US fire departments respond.4 This particularly needs to be considered in the analysis of certain variables such as geographic region. Moreover, each record only documents a single primary apparent symptom and the associated primary part of body injured. An injury may involve multiple symptoms and/or multiple body parts. Thus, the number of lower extremity injuries included in the study should be considered a minimum number of such injuries. Furthermore, the Primary Part of Body Injured numeric field only includes a single code for the lower extremity; the field does not include separate codes for more specific parts of the lower extremity (eg, knee, ankle, foot).
In conclusion, this study found that several hundred civilian lower extremity injuries resulting from fires were reported to a national database each year. Although the majority of these injuries were considered to be mild or moderate, most of the patients with a documented disposition were transported to an emergency care facility. The information in this study may be useful for creating strategies to prevent and manage civilian lower extremity injuries resulting from fires.
Mathias B. Forrester, BS, is an independent researcher in Austin, Texas. Now retired, he has performed public health research for various university and government programs for 40 years.
- Hall S. U.S. Fire Problem. Fire loss in the United States. National Fire Protection Association. October 31, 2024. Available at https://www.nfpa.org/education-and-research/research/nfpa-research/fire-statistical-reports/fire-loss-in-the-united-states. Accessed May 1, 2025.
- U.S. Fire Administration. National Fire Incident Reporting System. October 9, 2024. Available at https://www.usfa.fema.gov/nfirs/. Accessed May 1, 2025.
- U.S. Fire Administration. National Fire Incident Reporting System Complete Reference Guide. January 2015. Available at https://www.usfa.fema.gov/nfirs/documentation/. Accessed May 1, 2025.
- The National Fire Incident Reporting System and the Public Data Release File. NFIRS and PDR Overview 2023. In the 2023 All Incidents data download.
- U.S. Fire Administration. Access NFIRS Data. October 17, 2024. Available at https://www.usfa.fema.gov/nfirs/access-data/. Accessed May 1, 2025.
- Federal Emergency Management Agency. Annual NFIRS Public Data. Available at https://www.fema.gov/about/openfema/data-sets/fema-usfa-nfirs-annual-data. Accessed May 1, 2025.
- Ahrens M. U.S. Fire Problem. Home fire victims by age and gender. National Fire Protection Association. November 30, 2021. Available at https://www.nfpa.org/education-and-research/research/nfpa-research/fire-statistical-reports/home-fire-victims-by-age-and-gender. Accessed May 1, 2025.
- Forrester MB. Firefighter lower extremity injuries in the United States. Lower Extremity Review. 2025;17(3)28-34.
- U.S. Fire Administration. Residential fire estimate summaries (2013-2022) U.S. Fire Administration, May 15, 2024. Available at https://www.usfa.fema.gov/statistics/residential-fires/#:~:text=Overall%20trends%20for%20residential%20building,An%208%25%20decrease%20in%20injuries. Accessed May 1, 2025.
- Suzuki S, Manzello SL. The influence of COVID-19 stay at home measures on fire statistics sampled from New York City, London, San Francisco, and Tokyo. Fire Technol. 2022;58(2):679-688.





