Dirty Truth #5: Normal Gait Cycle has Both Pronation and Supination
By Jay Segel, DPM; Sally Crawford, MS
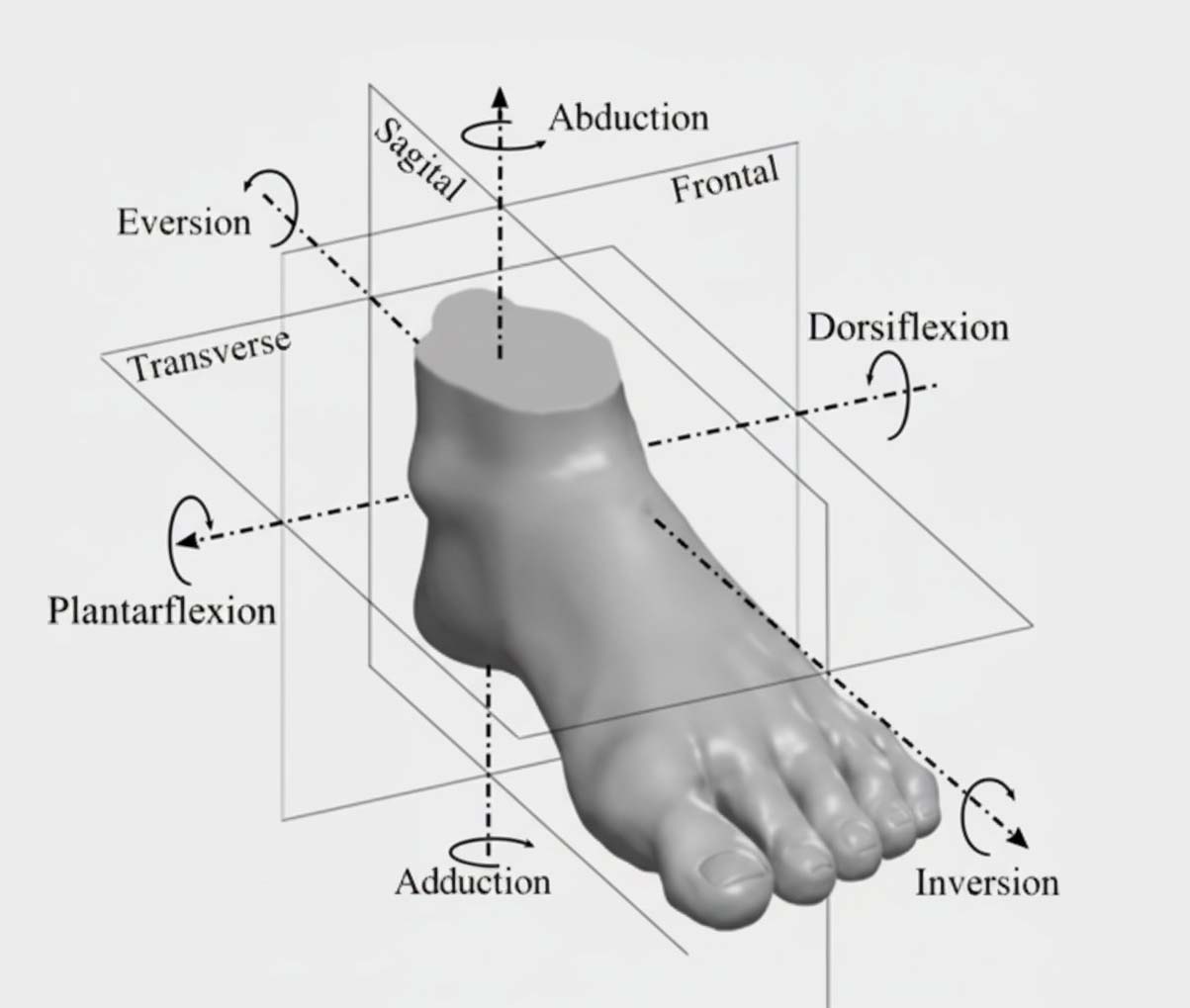
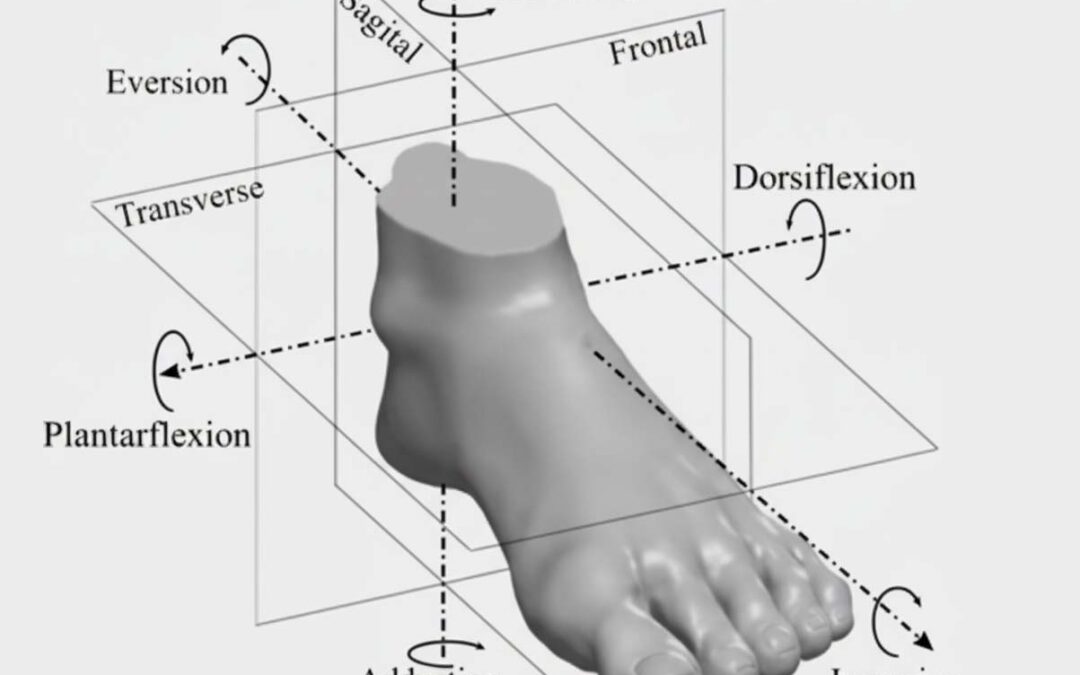
Figure 1: 3 axes of motion and 3 planes of motion
Each one of these so-called “Dirty Truths” has its specific reason, or reasons, for making the list. This one gets most of its “dirtiness” educationally and clinically. Many patients are familiar with the term “pronation,” though their understanding may vary. A clear explanation of body planes and planes of motion is important for an accurate understanding of this concept.
Whether we are lecturing to our colleagues or talking to our patients, we find it useful to begin with a simple grounding statement. “You can cut the body in half, 3 different ways, left/right, top/bottom, and front/back; those are body planes.” These 3 planes are identified as the sagittal plane (left/right), the transverse plane (top/bottom), and the frontal plane (front/back), which in the foot might commonly be known as proximal and distal. Each one of those planes has an axis of motion (Figure 1).
For example, if we were to cleave a cadaver in half, top and bottom, it would involve a horizontal cut, an axis of motion from left to right, or vice versa. In medical terminology, this is broken down as directional motions referred to as abduction and adduction. Similarly, a left/right division would involve a top-to-bottom cut referred to in foot terminology as dorsiflexion and plantarflexion axis of motion, while, lastly, the frontal plane, also known as the coronal
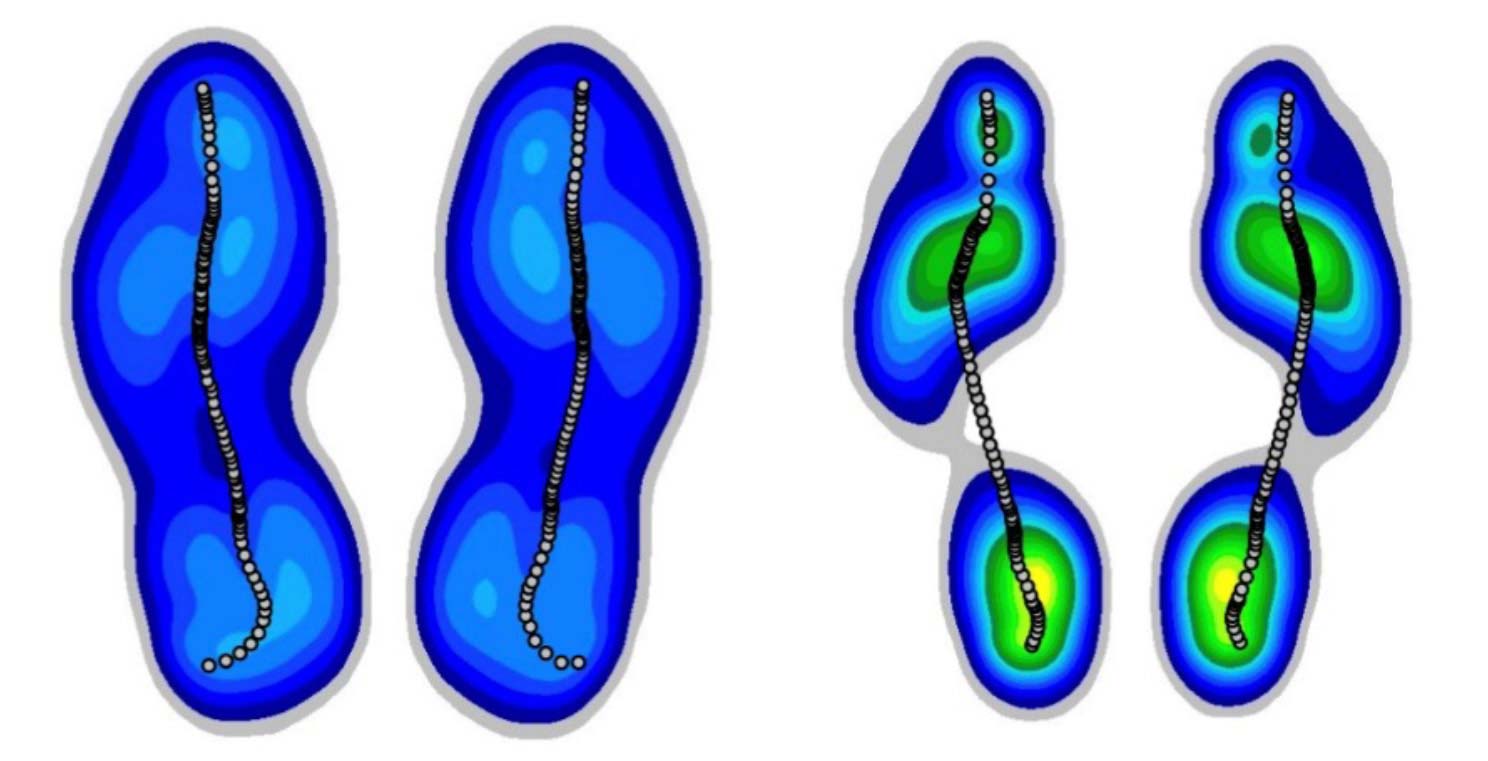
Figure 2: The black line shown through shod or barefoot contacts is a progressive aggregate of dots plotted on the pressure graph at the sample rate, a “where and when” type of representation.
plane, would have its axis of motion defined as inversion and eversion. Note that none of these are pronation or supination. The reason is that the motions described above occur in 1 plane, whereas pronation and supination are known as triplane motions. So, we often refer to pronation at the subtalar joint in terms of the talus bone, featured prominently in the first dirty truth1, as moving inward, downward, and forward in closed chain kinetics, otherwise described as when the foot is engaging with the support surface as opposed to non-weightbearing swing phase of gait.
Bringing this concept back to CAGA (computer-aided gait analysis) for observation and clarity, we introduce the center of pressure (COP) graph (Figure 2).
Please note that this COP can be broken down into moments and events to better understand gait characteristics to include pronation. These events, discussed in previous 101 articles, characterize events and motion (Figure 3).
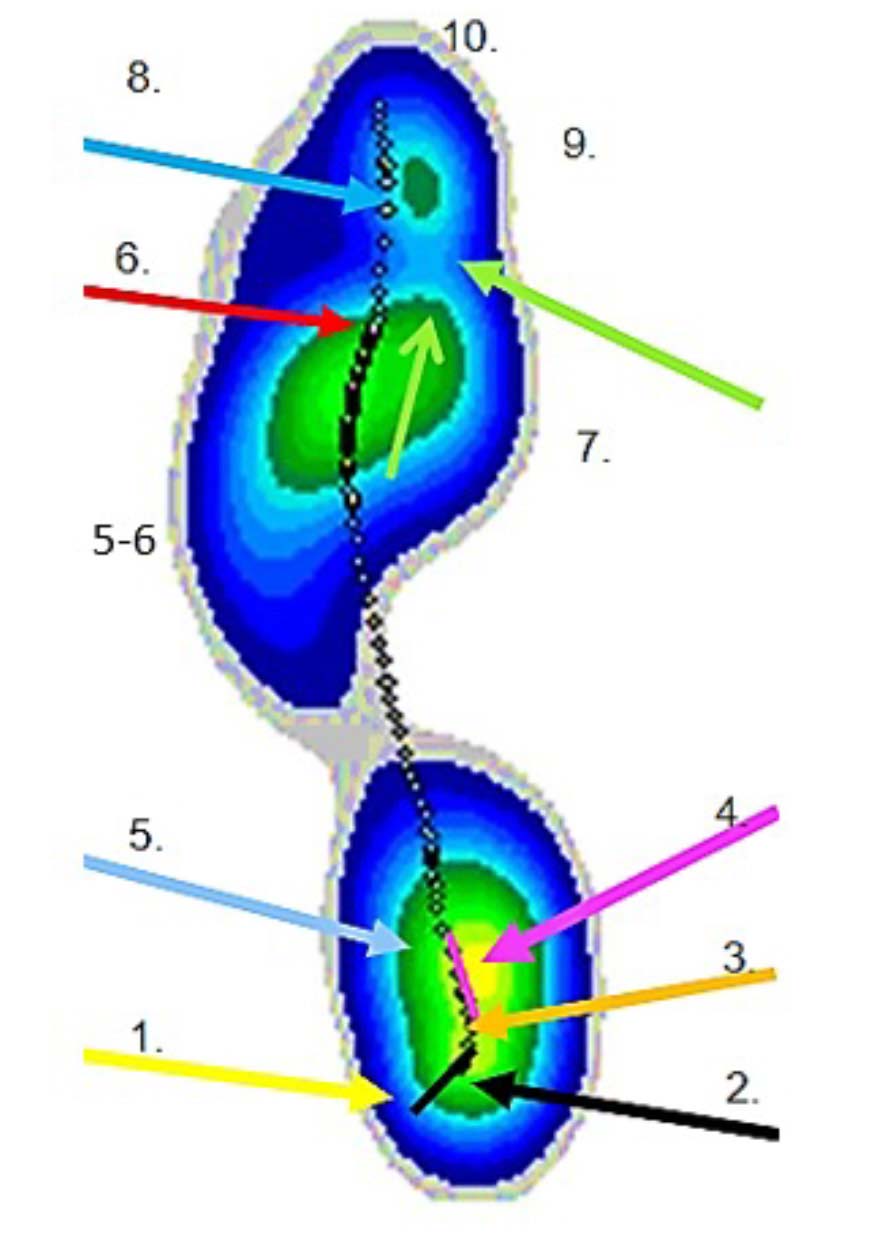
Figure 3: The COP begins with (1) Initial Contact Point, where the foot first touches the ground, often aligning with a neutral position. This is followed by (2) Initial Contact Response, as the foot adjusts to the surface, leading to (3) End Initial Contact Response Point. Next, (4) Initial Single Support Curve occurs during the contact or loading response phase, where 1 foot bears the body’s weight. The cycle progresses to (5) Re-supination Point, typically the second neutral intersection, marking a shift in foot alignment. This is followed by (5-6) Midstance Event, where the body is centered over the foot. Then, (6) Terminal Transition Point, often the third neutral intersection, signals the transition to the push-off phase. The (7) Forefoot Pronation Curve follows, leading to (8) Terminal Double Support phase, where both feet are briefly in contact with the ground. Finally, the (9) Toe-Off Curve leads to (10) Toe-Off Point, where the foot leaves the ground, completing the cycle.
Now that we have a firm footing, pun intended, let’s highlight some of the other issues revolving around this dirty truth. Patients often view pronation negatively, but it is actually the body’s natural shock absorber and a normal, beneficial function. The real concern is excessive pronation, not pronation itself (Figure 4).
As we have discussed, pronation is a motion, whereas pronated is a position. Consider this: if a foot is maximally pronated at contact/impact, it cannot go through a normal pronation event and therefore cannot adapt well to uneven surfaces nor provide needed shock absorption. Citing pronation alone is not enough; if we check out the top figure, one can note that pronation can happen in the rearfoot, midfoot, and forefoot, or at all three places and phases. Each should be considered and addressed separately and globally.
Lastly, it has been common practice to make custom orthoses with “X” degrees of varus posting to address pronation. When posting or canting an orthotic, what is happening is a change in weight-bearing foot position. By adding a varus wedge to a shoe or orthotic, it is essentially placing the foot in a biased supinatory attitude. This puts the foot at risk for poor adjustment to uneven surfaces and lateral ankle sprains. Briefly, when we rise and walk, often our first steps are to the side or a pivot, which are lateral movements. Placing the foot in a relatively supine position and then shifting our center of mass laterally increases the risk at initial contact. Taking this one step further, yes, pun intended again, the title of this dirty truth reminds us that normal gait contains both pronation and supination events, so curtailing pronation exacerbates supination, jeopardizing that foot to lateral column issues such as sinus tarsitis, tailor’s bunions, corns on the lateral toes, Morton’s neuroma, reduced shock amelioration, and lateral ankle sprains.
Note: There is a full vetting of this article called, “The Shortcomings of Gait Cycle Parameters in Patient Treatment.” *
*The Shortcomings of Gait Cycle Parameters in Patient Treatment. Jay Segel, DPM; Sally Crawford, MS, Biomed Eng. Podiatry Management. (Jan 2014)
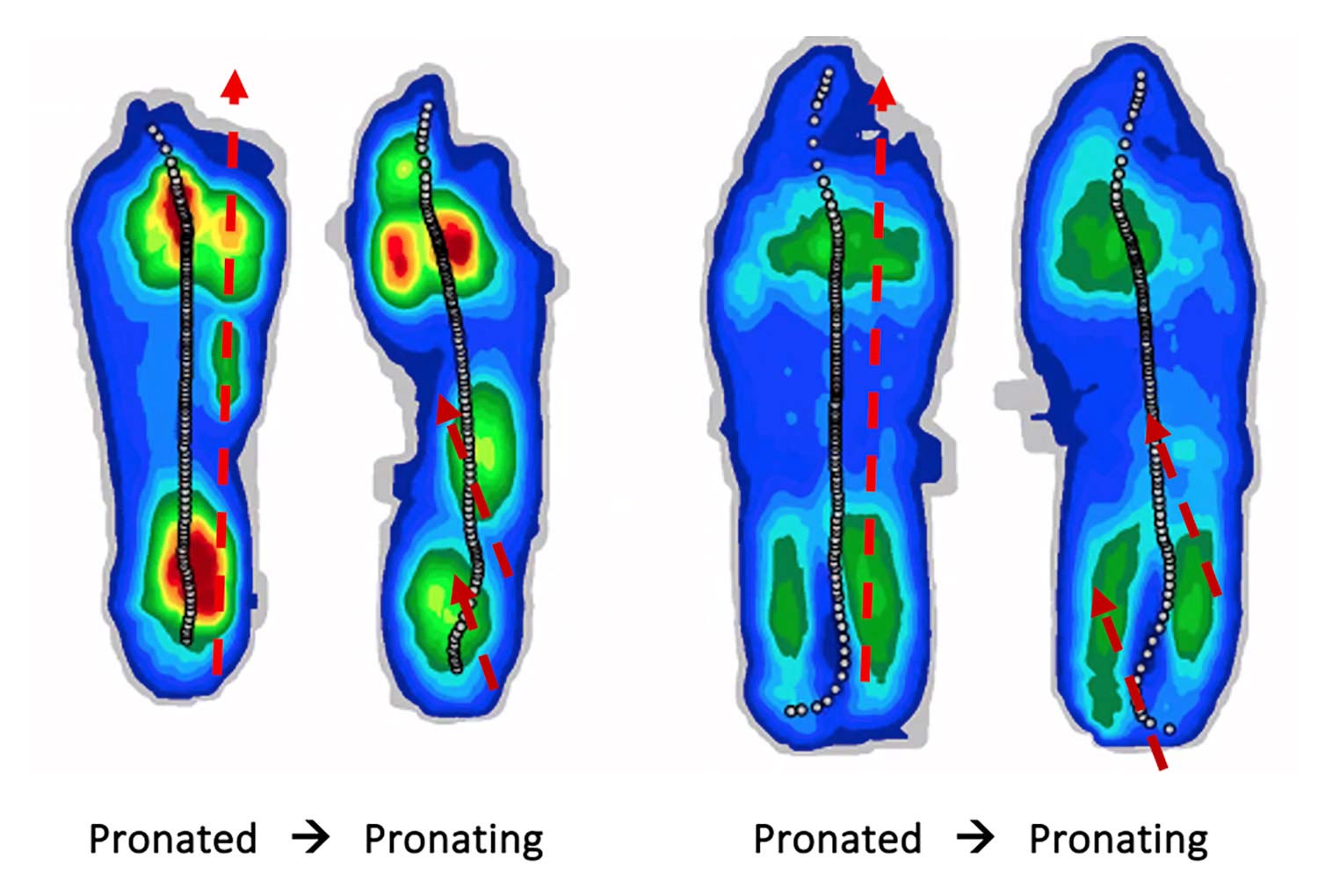
Figure 4: “Pronation is not pronated,” and they represent 2 very different biomechanical challenges.
- Segel J, Crawford S. Dirty Truth #1: The Foot Is Not Symmetrical. Lower Extremity Review. 2025;17(3):22-24.






“:placing the foot in a biased supinatory attitude. This puts the foot at risk for poor adjustment to uneven surfaces and lateral ankle sprain.” I disagree with this commonly used concept. Careful medial posting of the whole foot will reduce a few degrees of pronation 1. stabilizes the foot in stance phase and also thus putting it in a better position to regain supination as the foot rockers anteriorly as the heel rises. Using a mix shock absorbent and strong posting material still allows for some shock absorption at heel strike to foot flat. My determination as to how many medial degrees to post a foot is based on a couple of factors. The most important being the non weight bearing assessment and casting in a true subtalar neutral measurement and casting. Then assess the full weight bearing foot and post approximately 25~33% of the degrees of these 2 measurement between open and closed chain foot. I would not call reducing full pronation with a medial (full length post) = a supinatory attitude. It works from athletes to arthritis and all people in-between.
Thank you, thank you, thank you Jay and Sally.
I’ve been studying biomechanics since 1979 and have been incorporating into bespoke orthopaedic footwear for a similar length of time.
I have been shocked by the gradual decline in understanding amongst the allied health professionals to the extent that I was beginning to wonder if I was the one in the wrong.
Yet time and time again the wear patterns on footwear tell the same universal story. The foot strikes supinated and pronates as a loading response and from there the forefoot wear patterns tell a story about the wearer weight distribution during midstance and propulsion.
I’ve used The Medicapteur Winpod since 2004 and it’s clear that the gait line is more or less as described above.
The wear patterns on shoes, don’t just capture the gait cycle of a person walking shod across a force plate at one moment time, but they capture the accrued pattern of everyday walking, standing twisting and turning over several years by the wearer in their natural environment.
Pronation and supination aren’t just events in the foot and ankle, they begin with the anatomy trains of arm swing right down though the pelvis, hips and legs and equally go from the feet back up through the pelvis to the arm swing.
It’s a whole body dynamic.