

Bone bruises are commonly associated with anterior cruciate ligament (ACL) tears, but researchers are only beginning to understand the potential clinical significance of these chondral lesions with regard to knee osteoarthritis (OA) and preventing ACL injury recurrence.
By Cary Groner
Although most clinicians agree that the chondral damage suffered during ligamentous injuries such as ACL ruptures increases the risk of later knee OA, questions remain about the clinical significance of the bone bruises that sometimes underlie weakened cartilage.1,2
These lesions remain somewhat mysterious, and researchers have published contradictory findings about many issues related to bone bruises, including how long it takes them to heal and to what extent they put cartilage at risk and contribute to subsequent OA.
“Bone bruises are not terribly well understood,” said Robert Marx, MD, a professor of orthopedic surgery at the Hospital for Special Surgery in New York. “In athletes who’ve had trauma, they are indicative of trauma to the subchondral bone, but we also see them in people who have arthritis or other conditions.”
Seeing the bruises on magnetic resonance imaging (MRI) is one thing, Marx said; understanding their significance is something else.
“It’s indicative of the two bones essentially smashing into each other, frequently after an ACL tear, but sometimes without a ligament injury,” he said. “They can hurt for many months, but it’s yet to be proven whether they are related to the development of arthritis.”
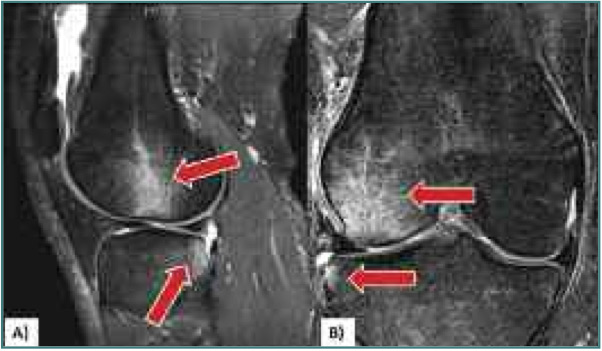
Figure 1. Magnetic resonance images of bone bruise patterns (lateral femoral condyle and posterolateral tibial plateau) associated with acute anterior cruciate ligament (ACL) injury, to which finite element model data are compared to determine relevance of injury condition. A: Sagittal plane view shows the more posterior location of the tibial bruise relative to the femoral bruise. Arrows point to the hyperintense signals associated with bone bruises. B: Frontal plane view shows lateral compression of the femur and tibia. (Reprinted with permission from reference 15.)
Jonathan Chang, MD, clinical associate professor of orthopedics at the University of Southern California in Los Angeles, noted that bone bruises weren’t even identified until the advent of MRI in the 1980s and 1990s.
“For years we weren’t sure what we were seeing, but now we know that this represents damage to the cancellous bone that has caused bleeding,” Chang explained. “Minor bone bruises tend to follow the course of most fractures, in that you get a slow healing over two to four months.”
With more serious bruises, however, trouble can arise.
“We’ve found that if the bone bruise is large enough, the body will have trouble maintaining or restoring circulation to the area, and you can get avascular necrosis of the bone,” he said. “In many cases, that circulation cutoff can lead to the chondral damage you see in a lot of our athletes.”
Quantification
Research suggests that bone bruises are more widespread than previously realized, and may in fact occur in 80% of patients who’ve had ACL ruptures. They’ve also been found after medial collateral ligament injury, posterior cruciate ligament injury, and in patients who haven’t damaged their ligaments.3 MRI findings are thought to represent areas of hemorrhage, edema, or infarction resulting from trabecular microfractures (trabecular bone is synonymous with the cancellous bone to which Chang referred) and, when associated with ACL injuries, occur most often in the lateral tibiofemoral compartment.3
As Chang suggested, how long bone bruises persist seems partly dependent on how serious they are. Some researchers have suggested that such bruises typically resolve six to 12 weeks after initial injury.4 Others have reported that the lesions last much longer. For example, researchers in the Netherlands reported in 2007 that median healing time in their study population was roughly 42 weeks.5
In an earlier study of 120 patients with acute post-traumatic knee hemoarthrosis, researchers detected bone bruises in 86 (72%) and then followed the patients for six to 12 months. Resolution was observed within that period in those with reticular bruises (hemorrhage and edema in medullary bone noncontiguous with the cortical bone of the subadjacent articular surface), and fortunately this was the most common type, accounting for 70% of patients with bone bruises. However, in those with geographic bone bruises (characterized by increased density and immediate continuity to adjacent cortical bone) researchers reported that evidence remained of osteochondral sequelae at the site of the bruise, including osteosclerosis, cartilage thinning, cartilaginous loss or defect, osteochondral defects, and cortical impaction with or without abnormal cortical bone.6
Other studies suggest similarly dire prognoses. One, for example, reported that six years after acute ACL injury, 15 of 23 patients (65%) with bone bruises had osteochondral sequelae despite ACL reconstruction. The authors concluded that the initial injuries had resulted in irreversible changes to the knee.7 And, in a 2008 study published in the Journal of Orthopedic Science, Japanese researchers found that bone bruise was related to subsequent tibiofemoral OA.8
Part of the diagnostic and prognostic difficulty lies in the lack of a common descriptive language. One more generally accepted grading system, by Matias Costa-Paz, MD, and his colleagues in Argentina, was published in Arthroscopy in 2001; it classified the lesions into three categories based on MRI findings: type 1 (a diffuse signal with change of the medullary component, often reticular and distant from the articular surface); type 2 (a localized signal contiguous to the subadjacent articular surface); and type 3 (disruption or depression of the normal contour of the cortical surface).9
The study helped delineate the healing times associated with different lesion severities. The authors reported 100% and 91% resolution of type 1 and 2 lesions, respectively, at two years; however, all five patients with type 3 bone bruises showed persistent abnormalities on MRI, even after ACL reconstruction. As noted, other studies have found similarly persistent problems, leading the authors of a recent literature review to conclude that they may result from a change in load bearing caused by subchondral or osteochondral microfracture and could signal early degenerative disease.3
Injury and homeostasis
Advanced MRI analysis has shed further light on the injury and its manifestations.

“This is really a transchondral fracture, not just a ho-hum bone bruise,” said Hollis Potter, MD, chief of the Division of Magnetic Resonance Imaging, director of research in the Department of Radiology and Imaging, and holder of the Coleman Chair in MRI research at the Hospital for Special Surgery. “Load is imparted through the cartilage into the bone; it occurs during the pivot shift. Cartilage resists compression but not shear, and often we see compression over the condyle but shear over the plateau.”
Despite its name, the tibial plateau is more subject to shear because its shape is actually convex. Chang emphasized the importance of this.
“The convexity of the plateau concentrates a lot more pressure in a small area, and that appears to be the reason we get more bone bruises on the lateral femoral condyle,” he said.
Potter explained that in a recent paper,10 she and her colleagues had found surprisingly high rates of chondral damage after ACL injury.
“In our study, we determined that a hundred percent of patients sustained some condyle damage, and that their risk of developing osteoarthritis was substantially elevated over time,” she said.
The study showed, specifically, that in the lateral tibial plateau, the size of the bone marrow edema pattern at baseline was significantly associated with increased cartilage loss at one, two, and three years; in the lateral femoral condyle, there was a similar association at one and two years but not at year three. Regardless of surgical interventions, however, by seven to 11 years after injury, the risk of cartilage loss in the lateral femoral condyle was 50 times that of baseline—as well as 30 times baseline in the patella and 19 times baseline in the medial femoral condyle.
“We recognized that the bone bruise or transchondral fracture was not just an isolated event,” Potter said. “The injury itself affects cartilage homeostasis, and you will have condyle depletion from areas that were not involved in the initial bruise.”
For example, Potter and her colleagues found that, in addition to the two most common acute injury sites—the lateral tibial plateau, followed by the lateral femoral condyle—where the risk of cartilage loss doubled from year one, the same rate of loss also occurred in the medial femoral condyle. Moreover, at the patella, the risk tripled.
“The rate of progression was high for the medial compartment as well as the patellofemoral joint, suggesting an accelerated progression in the ‘natural’ rate of chondral loss after ACL injury,” the authors wrote.
In the evolving view, then, the environment of the knee is subject to both mechanical and biochemical forces, both of which may be affected by the kind of injury that leads to bone bruises. Hyaline cartilage—the kind that covers the articular surfaces—has a complex structure that is avascular, aneural, and alymphatic, all of which makes healing difficult.11
Sequelae
Other scientists have evaluated the effects of bone bruises on surrounding tissue and reached conclusions similar to those of Potter and her colleagues. In one study, researchers assessed biopsy samples of geographic lesions in the subchondral bone and found death or degeneration of chondrocytes, proteoglycan loss, and necrosis of osteocytes.12 In another, researchers used histolic and immunostaining techniques to evaluate the status of articular cartilage and subchondral bone overlying bone bruises in patients with ACL tears; they reported a loss of the proteoglycan component in the matrix, as well as an increased presence of the degradation fragments of cartilage oligomeric matrix protein (COMP) in injured knees.11 Because COMP levels in synovial fluid are a marker for cartilage turnover in disease, this suggests significant injury and may indicate preclinical osteoarthritic lesions.
In a study published in Arthritis and Rheumatism in 2005, moreover, Swedish scientists used delayed gadolinium-enhanced MRI to study the associations between glycosaminoglycan (GAG) content in cartilage and synovial fluid in 24 patients with acute ACL injury. Nearly all (23) of the patients had bone bruises, and 15 had an isolated bone bruise in the lateral femoral condyle. The researchers concluded that ACL injury not only caused post-traumatic edema of the lateral femoral cartilage but also initialized a generalized biochemical change within the knee that led to GAG loss from both lateral and medial femoral cartilage.13
“That medial aspect was an area in which they didn’t [often] see the bone bruise,” said Potter, referring to that study.
But because the medial tibiofemoral compartment is where later OA often occurs, the findings bolster the view that ACL injury, and the associated bone bruises, affect the knee’s homeostasis and ability to repair itself.
MRI analysis doesn’t tell you everything you need to know about the patient’s status, however, even if you’re an expert like Potter.
“What’s amazing is that after twenty-two years of this, I can look at the exact same MRI findings in five different patients, and those patients will have a tremendous stratification of symptoms,” she said. “One will be completely asymptomatic; someone else will have the same findings but be in a wheelchair. Subjective pain and function scores are only part of the picture. That’s where imaging comes in, and biomarkers from serum, and potentially synovial fluid biomarkers, to look at early cartilage breakdown products.”
Applications
Some researchers and clinicians are already seeking ways to translate such knowledge into practical applications.
“If a large enough bone bruise exists, and it’s associated with a tenuous circulatory situation, you do need to have the patient dial back on activity, and to some extent on rehabilitation,” said Jonathan Chang. “You don’t want to stress the joint and the articular cartilage when the body is trying to recover.”
The authors of a 2006 review noted earlier3 reached a similar conclusion, writing, “It may be reasonable to delay return to full weight bearing when we find a large and severe bone bruise, to prevent further collapse of subchondral bone and further aggravation of articular cartilage injury.” The researchers also noted, however, that there is no hard evidence yet to support this contention, rational as it may seem.
In a presentation at the 2012 annual meeting of the National Association of Athletic Trainers (NATA) in St. Louis, Johanna Hoch, PhD, ATC, and her colleagues used the Costa-Paz grading system to describe the location and frequency of severe bone bruises found on MRI in 28 patients with acute knee ligament injuries.14 Each bruise was documented as in the lateral or medial femoral condyles (LFC or MFC, respectively), or on the lateral or medial tibial plateaus (LTP or MTP). Of the 60 bone bruises identified, 37% occurred on the LTP and 30% were on the LFC; the remaining 33% distributed between the MFC and MTP. Seven (12%) of the bruises were grade 1; 40 (68%) were grade 2; and 12 (20%) were grade 3. Most grade 1 and 2 lesions were located on the LTP (43% and 38%, respectively); however, of the grade 3 lesions, more than two-thirds (67%) were found on the LFC, with the other 33% on the LTP.
“We were seeing studies that documented bone bruises and how long it took them to resolve, but nobody was classifying them by size or severity,” said Hoch, who is an assistant adjunct and clinical education coordinator at the School of Physical Therapy and Athletic Training at Old Dominion University in Norfolk, VA, (the paper was written while she was a doctoral candidate at the University of Kentucky in Lexington).
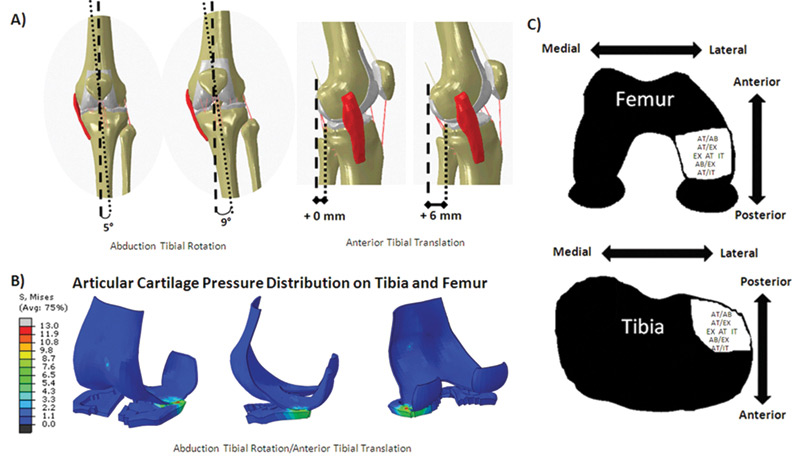
Figure 2. Injury conditions that resulted in peak articular cartilage contact pressure locations in the posterolateral tibia and lateral femur. A: Combined abduction, tibial rotation, and anterior tibial translation injury conditions. B: Articular cartilage pressure distribution during abduction, tibial rotation, and anterior tibial translation in the group of individuals who suffered ACL injuries. C: Loading conditions that resulted in articular cartilage stress patterns similar to the bone bruise patterns associated with ACL injury on the femur and tibia. (Reprinted with permission from reference 15.)
“I thought that if we could follow this data longitudinally, maybe we could find a relationship between severity, size, and outcomes,” Hoch said. “If we follow up at an average of three years and find articular cartilage changes, can we confirm that these changes are associated with larger, more severe lesions? We may not see that cartilage damage on initial MRI or arthroscopy, but the changes may develop over time because the cartilage isn’t able to regain its homeostasis and continues to degrade.”
Hoch’s larger point isn’t just about predictive maps; she hopes her team’s findings may lead to changes in therapeutic regimens.
“As other researchers have suggested, we may need to delay ACL reconstruction to allow the lesion and the cartilage to heal, or delay full weight-bearing status to prevent further collapse of the subchondral bone and further aggravation of the overlying articular cartilage,” she said. “But we don’t really have a basis for making those decisions, and that’s where our paper was coming from—what about severity? Is there an association? We need to investigate the outcomes and see.”
Prevention
Other scientists are investigating ways to use individual bone bruise data to prevent recurrent injuries. In a 2011 paper published in the American Journal of Sports Medicine (AJSM), researchers at The Ohio State University in Columbus noted that the location of a bone bruise after ACL injury provides evidence of the injury mechanism itself.15
The investigators created a computer model to analyze tibial and femoral articular cartilage pressure distributions during normal landing and injury simulations, and used the model to identify the biomechanical variables that led to peak articular cartilage pressures in the posterior-lateral tibia and mediolateral femur—distributions similar to bone bruise patterns associated with ACL injury (Figure 1). Then they took prospective biomechanical data on 399 female athletes, nine of whom ultimately suffered ACL injuries, and used the computer model to simulate ACL injury mechanisms for each group and determine the corresponding articular cartilage pressure distributions (Figure 2).
An intriguing aspect of the research was that the scientists combined in vivo data, in vitro cadaveric data, and in silica computer modeling in a technique they call “in sim” (short for in simulacra amalgama)—a comprehensive approach that provides more complete information than any of the methodologies alone.16
“It’s challenging to study the mechanism of ACL injury, because you can’t really identify what’s going on with the internal structures during the event,” said Carmen Quatman, MD, PhD, a clinical instructor of orthopedic surgery at the university and the paper’s lead author. “A bone bruise is essentially micro-damage, and we think it is likely a footprint of what is happening during the injury. The purpose of the study, and of our ongoing work, is to look at what the bruises can tell us about the directional forces that occur during the injury. If we could identify them—and it may be that certain patients have somewhat different patterns—then we could try to prevent future injury by targeting the opposite of those forces, trying to figure out how we could prevent someone from going into that dangerous position.”
The goal, she told LER, is to make the modeling as clinically relevant as possible, which requires a paradigm shift.
“To study multiple perspectives at once, we target the same questions with multiple methods, with the ultimate goal of refining everything,” Quatman said. “We develop our computer model based on the anatomy of young athletes, and our cadaver data are driven by our live data as well. By using this technology we can start to think about what’s going on internally and look at predictive patterns.”
Quatman noted that athletes younger than 25 years who injure an ACL have a significant chance of re-tearing it when they return to high-risk sports after surgical reconstruction. If clinicians could look at the MRI from the patient’s acute injury, plug that information into a computer model, then get an accurate description of the forces that led to the bone bruise, they would theoretically be able to design a custom neuromuscular workout program to prevent reinjury.
“The bone bruise tells us something,” Quatman continued. “Ideally, you could go backward and say, ‘This is what we think happened; this is a dangerous motion or posture for you, so we want to keep you out of it.’”
The team reported in the AJSM article that the lateral tibial and femoral bone bruises associated with acute ACL injury may occur due to lateral joint compression, and that the more posterior location of the lesions on the tibial plateau, relative to the femur, may indicate that the tibia shifts anteriorly or rotates internally relative to the femur during the injury event. The findings support the notion that a valgus collapse injury mechanism results from tibial abduction combined with anterior tibial translation or either external or internal tibial rotation.
“Our group feels strongly that these injuries are multiplanar, and that the mechanism differs between people,” Quatman explained. “We found that people who landed at initial [baseline] posture with their knees about five degrees more valgus, given the same anterior tibial perturbation, had a lot higher ACL strain; that was the group that went on to ACL injury.”
As a clinician, Quatman views such complex computer modeling as an important tool.
“Any kind of gross estimation identified in these multiplanar layers is better than standing there, trying to eyeball how the knee is moving in space,” she said. “From a clinical perspective, I might not know the exact pressure going through the tibia, but I don’t necessarily need to know that. I just need to know that it is fivefold greater in this patient when they land in a valgus posture than it is in the person who lands in a more neutral posture.”
The future
As such research continues, and investigators develop a more sophisticated understanding of the association between bone bruises, ligamentous reinjury, and the risk of subsequent osteoarthritis, clinicians and their patients will ideally end up with an array of new weapons to combat both repeated injuries and their long-term sequelae.
Cary Groner is a freelance writer based in the San Francisco Bay Area.
1. Groner C. ACL injury and OA risk: surgery’s complicated rule. LER 2012;4(6):18-23.
2. Groner C. ACL injury and OA risk: surgery’s complicated rule. LER 2012;4(7):65-69.
3. Nakame A, Engebretsen L, Bahr R, et al. Natural history of bone bruises after acute knee injury: clinical outcome and histopathological findings. Knee Surg Sports Traumatol Arthrosc 2006;14(12):1252-1258.
4. Miller MD, Osborne JR, Gordon WT, et al. The natural history of bone bruises: a prospective study of magnetic resonance imaging detected trabecular micro fractures in patients with isolated medial collateral ligament injuries. Am J Sports Med 1998;26(1):15-19.
5. Boks SS, Vroegindeweij D, Koes BW, et al. MRI follow-up of posttraumatic bone bruises of the knee in general practice. Am J Roetgenol 2007;189(3):556-562.
6. Vellet AD, Marks PH, Fowler PJ, Munro TG. Occult posttraumatic osteochondral lesions of the knee. Prevalence, classification, and sort terms equally evaluated with MR imaging. Radiology 1991; 178(1):271-276.
7. Faber KJ, Dill JR, Amendola A, et al. Occult osteochondral lesions after anterior cruciate ligament rupture. Six-year magnetic resonance imaging follow-up study. Am J Sports Med 1999;27(4):489-494.
8. Oda H, Igarashi M, Sase H, et al. Bone bruise in magnetic resonance imaging strongly correlates with the production of joint effusion and with knee osteoarthritis. J Orthop Sci 2008;13(1):7-15.
9. Costa-Paz M, Muscolo DL, Averza M, et al. Magnetic resonance imaging follow-up study of bone bruises associated with anterior cruciate ligament ruptures. Arthroscopy 2001; 17(5):445-449.
10. Potter HG, Jain SK, Ma Y, et al. Cartilage injury after acute, isolated anterior cruciate ligament tear: immediate and longitudinal effect with clinical/MRI follow-up. Am J Sports Med 2012;40(2):276-285.
11. Fang C, Johnson D, Leslie MP, et al. Tissue distribution and measurement of cartilage oligomeric matrix protein in patients with magnetic resonance imaging-detect bone bruises after an acute anterior cruciate ligament tears. J Orthop Res 2001;19(4):634-641.
12. Johnson DL, Urban WP Jr, Caborn DN, et al. Articular cartilage changes seen with magnetic resonance imaging–detected bone bruises associated with acute anterior cruciate ligament rupture. Am J Sports Med 1998;26(3):409-414.
13. Tiderius CJ, Olsson LE, Nyquist F, Dahlberg L. Cartilage glycosaminoglycan loss in the acute phase after an anterior cruciate ligament injury: delayed gadolinium-enhanced magnetic resonance imaging of cartilage and synovial fluid analysis. Arthritis Rheum 2005;52(1):120-127.
14. Hoch J et al. A descriptive analysis of bone bruise presence and severity based on location for patients with acute knee injury. Presented at National Athletic Trainers Association Annual Meeting, St. Louis, June 2012.
15. Quatman CE, Kiapour A, Myer GD, et al. Cartilage pressure distributions provide a footprint to define female anterior cruciate ligament injury mechanisms. Am J Sports Med 2011;39(8):1706-1713.
16. Quatman CE, Quatman CC, Hewett TE. Prediction and prevention of musculoskeletal injury: a paradigm shift in methodology. Br J Sports Med 2009;43(14):1100-1107.





