
By Maryam M. Sadaak, Salwa Fadl AbdElMageed, and Mona Mohamed Ibrahim
This study came as highly needed because it highlighted the benefit of aquatic training in the rehabilitation of Grade 3 acute ankle sprain by showing very promising results.
 Ankle sprains are the second most common sports injury after knee injuries, with about 85% of them affecting the lateral ankle ligaments, and ankle injuries account for 14% of orthopedic emergency visits related to sports. These injuries are particularly prevalent in sports like basketball and volleyball due to jumping and landing mechanisms as well as rapid direction changes.
Ankle sprains are the second most common sports injury after knee injuries, with about 85% of them affecting the lateral ankle ligaments, and ankle injuries account for 14% of orthopedic emergency visits related to sports. These injuries are particularly prevalent in sports like basketball and volleyball due to jumping and landing mechanisms as well as rapid direction changes.
Physiotherapy, incorporating functional therapy along with a pain-free active range of motion, manual therapy, anteroposterior manipulation, therapeutic exercise, taping, muscle strength training, stability training, and sport-specific exercises, has shown promising results compared to immobilization and the PRICE (Protection, Rest, Ice, Compression and Elevation) protocol only during the inflammatory phase. The use of a semi-rigid cast in the early phase of ankle sprain was associated with faster recovery and higher satisfaction compared to elastic bandages. In cases where conservative treatment fails to improve stability, pain, or function after 3–6 months, surgical intervention with the modified Broström technique as the primary approach was recommended, followed by the anatomical reconstruction approach when there is a lack of adequate tissues for repair.
With this in mind, the study authors sought to investigate the effect of aquatic therapy as an early rehabilitation protocol for elite athletes with acute Grade 3 lateral ankle sprain Grade 3 on back-to-sport time, dynamic balance, pain, athletic performance, and muscle power compared to land-based exercise training.
Methods
The cohort included 38 athletes, age 18–30 years, with Grade 3 ankle sprain with sprain onset from 1 to 7 days. All participants are professional athletes, mainly participating in above-head sports such as volleyball and basketball. The patients were randomly allocated into 2 treatment groups: Group I (control group): 15 patients received a conventional physical therapy (PT) program of structured therapeutic exercise program, manual therapy, and land-based exercises, in addition to external support; and Group II (aquatic therapy group): 15 patients received aquatic training (refer to blue box on page 48). Visual Analog Scale (VAS) was used to measure the pain intensity, while the dynamic balance was measured by the Star Excursion Balance Test (SEBT). Athletic performance was measured by HOP Tests (single, triple, 6-m, and crossover hops) aided by the Agility T-Test (ATT) and Illinois Agility Test (IAT). Muscle power was tested by a single leg press. Finally, back to sports time was recorded for each participant in both groups.
Results
There was a significant interaction effect of aquatic therapy and time for VAS (P < 0.001), single hop (P < 0.001), triple hop (P < 0.001), crossover hop (P < 0.001), IAT (P = 0.019), and ATT (P < 0.001) of both affected and nonaffected. There was no significant interaction effect of aquatic therapy and time for 6-MHT of affected (P = 0.923) and nonaffected (P = 0.140). There was a significant main effect of time for all dependent variables (P < 0.001) except for 6-MHT of affected (P = 0.939), nonaffected (P = 0.109) subjects, and IAT (P = 0.099). The SEBT and single leg press revealed a significant difference between groups on affected and non-affected sides (P < 0.001*). Lastly and most importantly, the back-to-sport time revealed a significant difference in the return-to-sport time in favor of the aquatic therapy group, who returned faster than the control group (P < 0.001*) (Figure).
Discussion
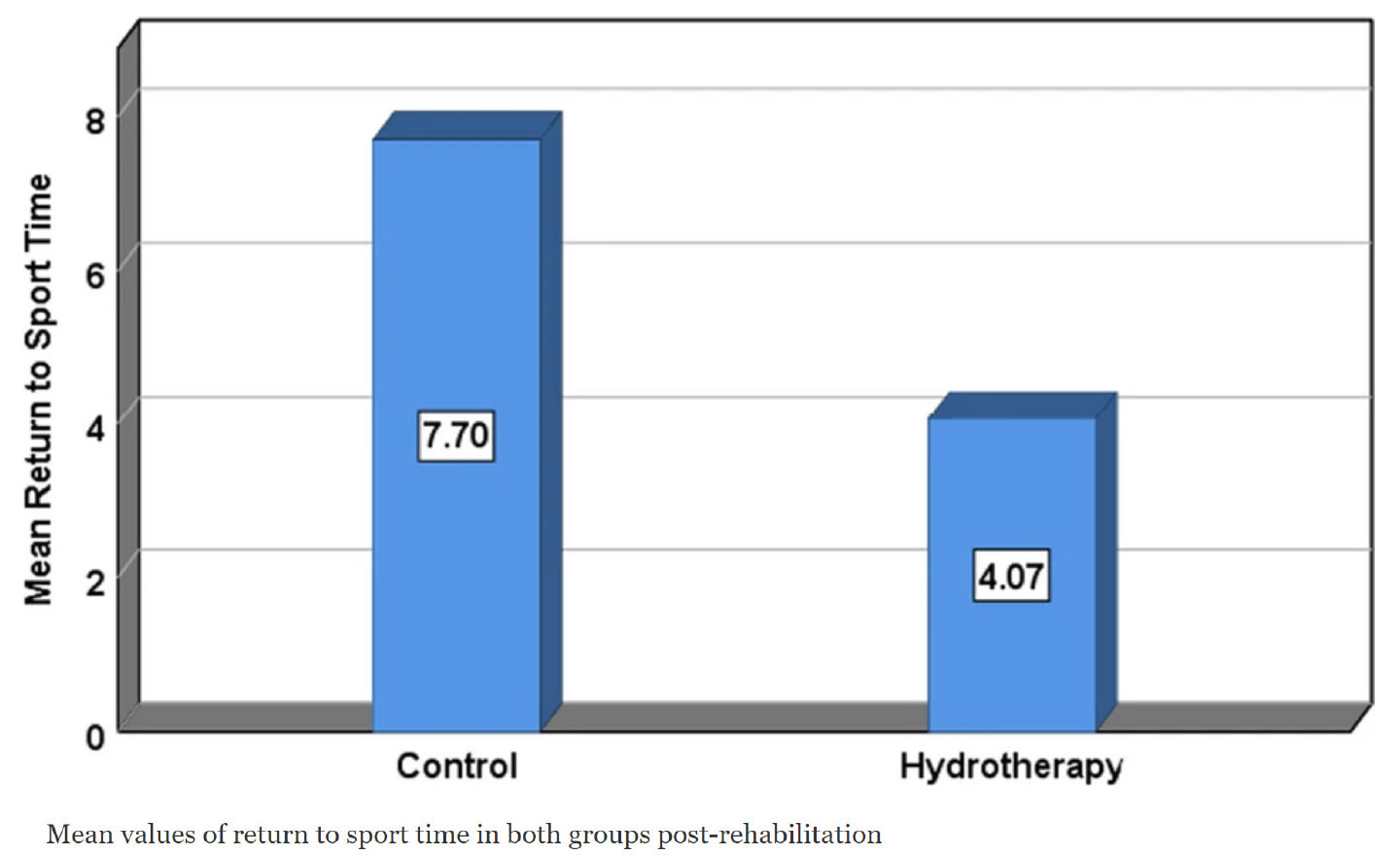 The findings of the present study demonstrate the superiority of an accelerated early intervention protocol utilizing a 4-week aquatic therapy training program for Grade 3 acute ankle sprain in elite professional athletes. A comparison with the traditional physiotherapy rehabilitation program revealed significant differences favoring the aquatic therapy group in terms of ankle pain, overall functionality, dynamic balance, and various athletic performance and power measures. Notably, athletes following the suggested aquatic therapy protocol achieved a faster return to sport, approximately 4.7 weeks after injury, compared to 7.7 weeks for land-based exercises used in the control group. These results challenge the common practice of immobilization and casting and recently rigid tapping as the initial treatment, favoring functional treatment and therapeutic exercises in enhancing athletic performance and reducing the risk of reinjury.
The findings of the present study demonstrate the superiority of an accelerated early intervention protocol utilizing a 4-week aquatic therapy training program for Grade 3 acute ankle sprain in elite professional athletes. A comparison with the traditional physiotherapy rehabilitation program revealed significant differences favoring the aquatic therapy group in terms of ankle pain, overall functionality, dynamic balance, and various athletic performance and power measures. Notably, athletes following the suggested aquatic therapy protocol achieved a faster return to sport, approximately 4.7 weeks after injury, compared to 7.7 weeks for land-based exercises used in the control group. These results challenge the common practice of immobilization and casting and recently rigid tapping as the initial treatment, favoring functional treatment and therapeutic exercises in enhancing athletic performance and reducing the risk of reinjury.
Related research regarding this study showed no significant difference between aquatic therapy and land-based therapy regarding chronic ankle instability treatment. Therefore, this study came as highly needed because it highlighted the benefit of aquatic training in the rehabilitation of Grade 3 acute ankle sprain by showing very promising results.
Aquatic therapy presented strong historical beneficial usage and overall reduction of pain together with both cardiovascular and musculoskeletal health beneficial effects through water buoyancy. However, it showed no significant difference from other types of therapy for some orthopedic conditions such as osteoarthritis. Therefore, these studies formed a strong base for the current study to support the superior results that were shown by this study.
Considering individual preferences and factors like cost, accessibility, and resource availability is crucial when selecting the most appropriate treatment for acute ankle sprains. Aquatic therapy may be particularly suitable for individuals who prefer water-based exercises or have limitations in weight-bearing activities, while traditional PT may offer greater accessibility and cost-effectiveness for certain individuals.
The current study focused on the ultimate way to decrease the return-to-sport time while maintaining the optimal performance level, the least amount of pain, and ideal balance and muscle power, which in return increased the general satisfaction and psychological welfare of both the athletes and their contractors. However, it was limited to the professional athletic population of mainly overhead athletes and high-contact sports age 18–30 years and had injuries within 7 days.
The findings of the current study agreed with that of a previous study regarding edema and pain in specific musculoskeletal conditions of assuming the upright position during running in water. This upright posture resembles walking and non-weight-bearing exercise in warm water in the aquatic therapy group. Moreover, certain studies have indicated that aquatic therapy could potentially alleviate pain in individuals with musculoskeletal injuries when compared to receiving no therapy. However, these studies did not find significant pain reduction benefits of aquatic therapy when compared to ground exercises.
Previous research has consistently indicated that aquatic therapy holds promise in enhancing performance outcomes among athletes with musculoskeletal injuries and has found supporting evidence for its efficacy in regard to muscle power and performance parameters. Aquatic therapy can help athletes with deficits secondary to ankle sprain by facilitating early rehabilitation through water buoyancy, reducing pressure over the joints, decreasing pain and swelling, and increasing strength, flexibility, and range of motion. It also provides a low-impact environment for athletes, reducing stress on the joints and allowing them to safely perform exercises that may not be possible on land. Underwater exercises can improve balance and stability in athletes with ankle sprains by enhancing proprioception, leading to improved joint stability and better performance on land-based activities. Further, investigations assessing the impact of aquatic therapy on various athletic performance measures, such as speed, jumping ability, and power, have reported significant improvements following the intervention.
In line with these findings, this study demonstrated that elite professional athletes participating in a 4-week aquatic therapy training program exhibited significant improvements in muscle power level, agility, and balance compared to those undergoing traditional PT rehabilitation. These results reinforce the notion that aquatic therapy offers a valuable approach to optimizing athletic performance during the recovery process.
While this study demonstrated significant positive outcomes of aquatic therapy for Grade 3 ankle sprains, several questions remain unanswered, presenting avenues for future research. Firstly, the long-term effects of aquatic therapy on functional outcomes, such as return to sports and prevention of recurrent sprains, need to be explored. Lastly, exploring the potential benefits of combining aquatic therapy with other complementary interventions, such as manual therapy or neuromuscular training, may further enhance the rehabilitation outcomes for individuals with Grade 3 ankle sprains. Future research endeavors addressing these unanswered questions will contribute to a deeper understanding of the therapeutic potential of aquatic therapy and further optimize its application in clinical practice.
Conclusion
Aquatic therapy is more effective than traditional protocols regarding early rehabilitation of Grade 3 acute ankle sprain in elite professional athletes for reducing pain intensity, improving dynamic balance and athletic performance and power, and accelerating their return to sports time. Because aquatic therapy produces better outcomes, it is advised to be included in the rehabilitation programs of athletic patients with Grade 3 acute ankle sprains.
Authors
Maryam Sadaak is a sports injuries physiotherapist with Smouha Sporting Club, Alexandria, Egypt.

Salwa Fadl AbdElMageed is a professor with the Department of Physical Therapy for Musculoskeletal Disorders and its Surgeries, Faculty of Physical Therapy, Cairo University, Cairo, Egypt.
Mona Mohamed Ibrahim, PhD, is an assistant professor with the Department of Physical Therapy for Musculoskeletal Disorders and its Surgeries, Faculty of Physical Therapy, Cairo University, Cairo, Egypt
This article has been excerpted from “Effect of aquatic versus conventional physical therapy program on ankle sprain Grade 3 in elite athletes: randomized controlled trial.” J Orthop Surg Res 19, 400 (2024). https://doi.org/10.1186/s13018-024-04855-0. Editing has occurred, including the renumbering or removal of tables and figures, and references have been removed for brevity. Use is per CC Attribution 4.0 International License.





