By Christy M. King DPM, FACFAS
 Avascular necrosis (AVN) of the talus presents one of the most complex and challenging problems in foot and ankle surgery, particularly in the aftermath of talar fractures. As podiatric specialists, understanding its nuances–from its unique anatomical predisposition to the evolving landscape of its management–is crucial for optimizing patient outcomes. My goal is to provide an insightful overview for clinicians, detailing diagnostic approaches, conservative and surgical interventions, and practical tips for navigating this formidable condition.
Avascular necrosis (AVN) of the talus presents one of the most complex and challenging problems in foot and ankle surgery, particularly in the aftermath of talar fractures. As podiatric specialists, understanding its nuances–from its unique anatomical predisposition to the evolving landscape of its management–is crucial for optimizing patient outcomes. My goal is to provide an insightful overview for clinicians, detailing diagnostic approaches, conservative and surgical interventions, and practical tips for navigating this formidable condition.
The Talus: An Anatomic Vulnerability
The talus is a truly unique bone, intricately designed to channel forces from the upper body to the intricate structures of our feet. Its susceptibility to AVN stems from several distinct anatomical features:
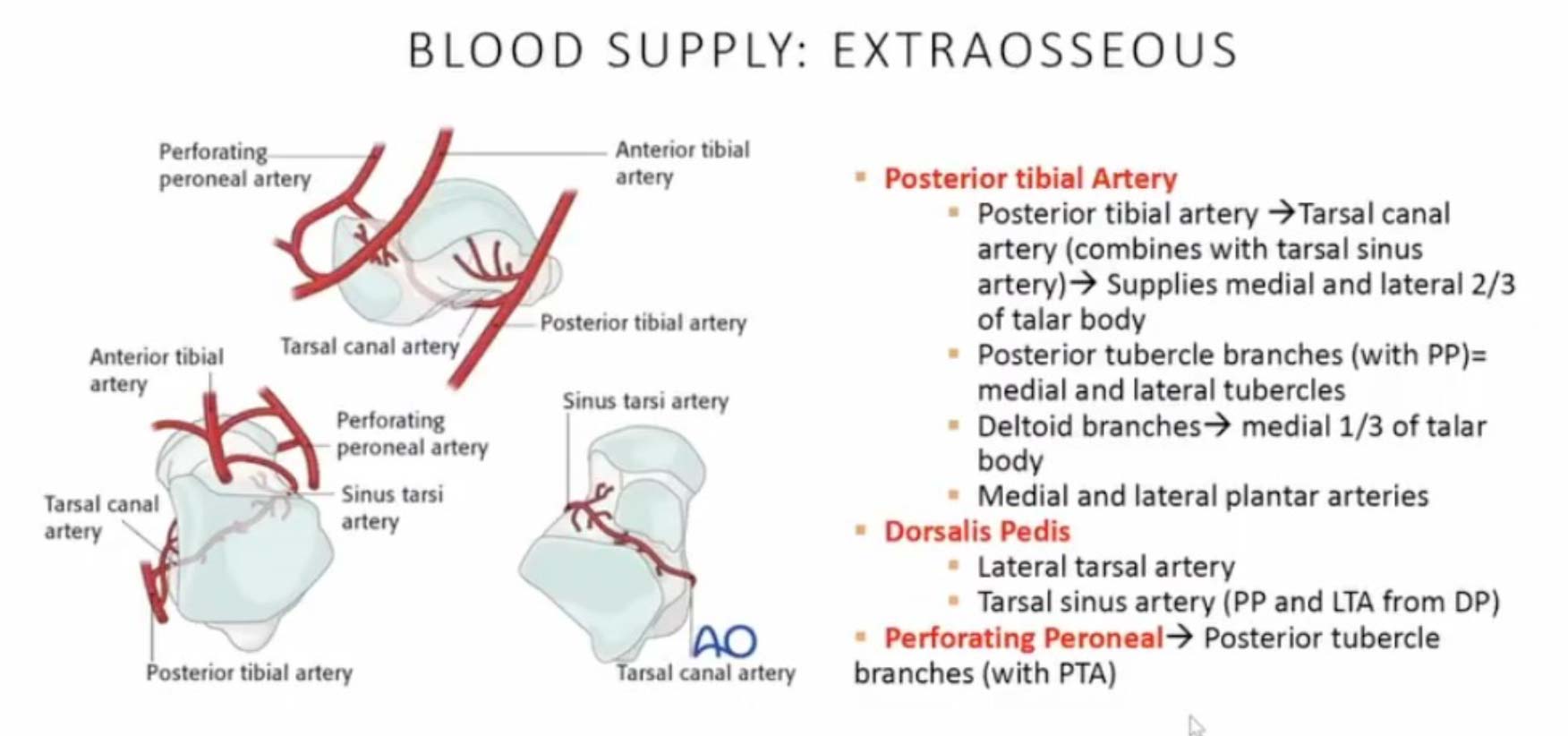
- High Cartilage Content: Approximately 60% of the talus is covered in cartilage, limiting areas for extraosseous blood supply penetration.
- Limited Attachments: Unlike most bones, the talus lacks muscle or tendon attachments, further restricting potential vascular access points.
- Delicate Blood Supply: While 3 main vessels supply the talus, they are much smaller, with a significant portion of the blood supply originating from the medial side. This makes the lateral side of the talus more prone to AVN. The intraosseous blood supply is even more intricate and variable, leading to diverse patterns of AVN within the bone.
- Traumatic Onset: Almost 75% of talar AVN cases are traumatic, directly linking the initial injury, such as a talar fracture with open reduction and internal fixation (ORIF), to the onset of bone death due to ischemia. The bone attempts to revascularize and reabsorb necrotic bone, but often fails due to inadequate blood supply, leading to sclerosis and eventual collapse.
 Diagnosis and Staging: Pillars of Effective Management
Diagnosis and Staging: Pillars of Effective Management
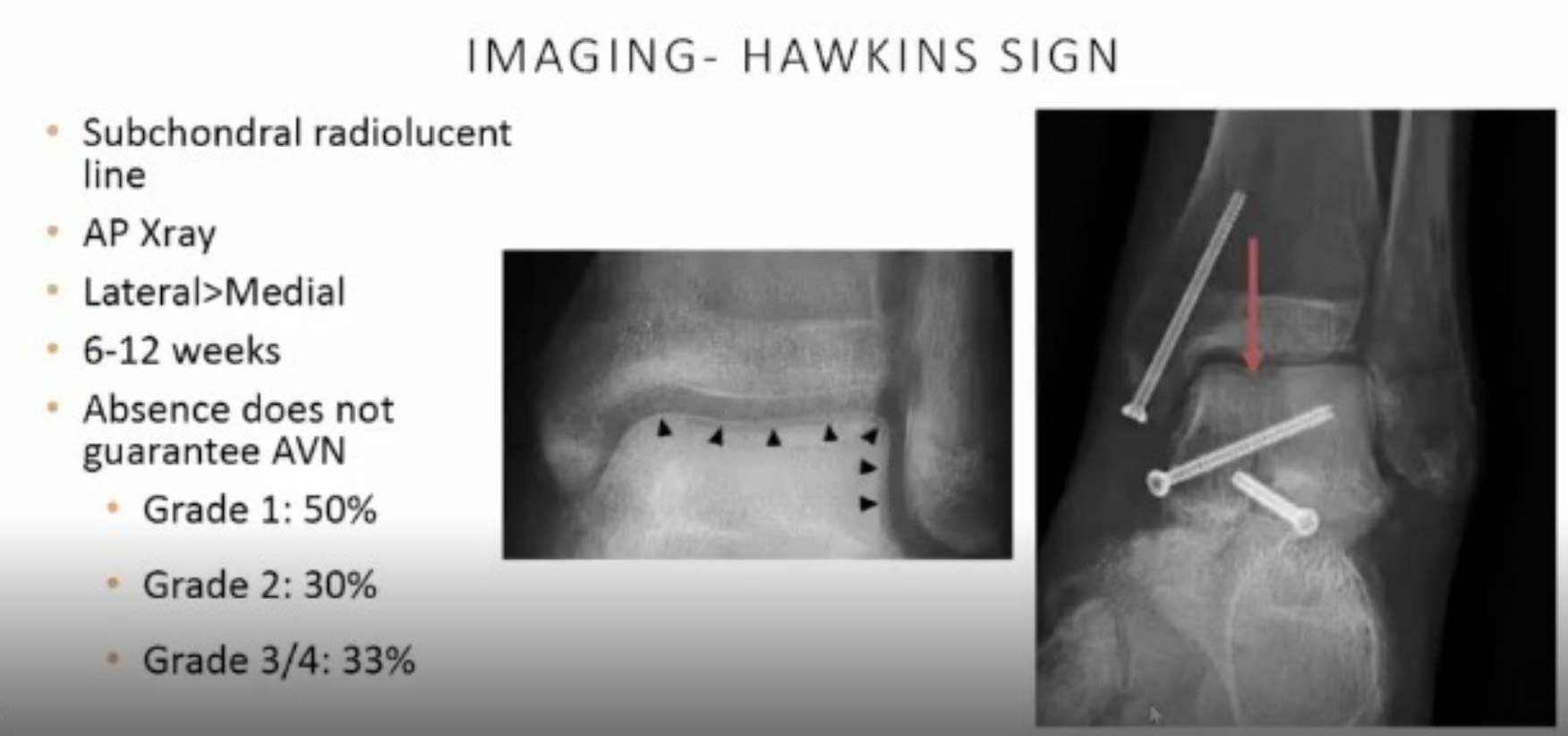
Early and accurate diagnosis is paramount. X-rays remain the easiest initial tool to observe signs of revascularization, such as the Hawkins sign. The Hawkins sign, a subchondral radiolucent line, is most often seen on an AP X-ray, typically appearing 6 to 12 weeks post-injury. Its presence is a positive indicator of revascularization, though its absence does not guarantee AVN development.
For greater sensitivity, especially in early stages, MRI is invaluable. It can detect AVN with high accuracy and help evaluate the degree and location of involvement. CT scans are useful for visualizing cystic or sclerotic changes, and bone scintigraphy can assess osteoblastic activity.
Staging systems are critical for guiding treatment pathways:
- Hawkins Classification: This system categorizes talar fractures based on the number of dislocated joints. Unfortunately, Hawkins Type III (subtalar and ankle dislocation) and Type IV (subtalar, ankle, and talonavicular dislocation) fractures are associated with a nearly 100% chance of developing AVN. This underscores the importance of early and honest discussions with patients about the potential long-term course of their injury.
- Fiscat Scaling: Initially developed for femoral AVN, Fiscat scaling is also applicable to the talus, correlating imaging findings with clinical signs to inform treatment decisions.
Treatment Options: A Phased Approach
Management of talar AVN ranges from conservative strategies to complex surgical interventions, chosen based on the stage of AVN and patient presentation.
 Conservative Therapies:
Conservative Therapies:
- Non-weightbearing (NWB): This is a highly effective initial therapy for early signs of sclerosis or poor vascularization. A landmark study by Canali and Kelly (1978) showed that nearly 9 months of NWB resulted in 90% good to excellent outcomes. Clinical Tip: I advise keeping patients non-weightbearing for approximately 3 months post-ORIF, allowing for range of motion around 6–8 weeks. If AVN is suspected, a trial of 3 months of NWB is recommended before considering more extensive interventions.
- Partial Weightbearing (PWB): This can be introduced in later stages, often with the aid of patellar weight-bearing braces or other offloading devices, as vascularization begins.
- Extracorporeal Shockwave Therapy (ESWT): This promising non-invasive option has shown benefit in early-stage (Fiscat 1–2) traumatic talar AVN. A 2010 study by Zhai demonstrated that ESWT improved AOFAS and VAS scores and decreased necrotic areas on imaging. Clinical Tip: If accessible, ESWT is a great adjunct for treatment, though more research in this area is needed.
 Surgical Interventions:
Surgical Interventions:
- Core Decompression: While primarily supported by data from atraumatic AVN, it can be considered for stages 1 and 2, and possibly stage 3 without cortical collapse, to reduce intraosseous pressure and enhance revascularization. However, data supporting its efficacy in traumatic AVN is limited.
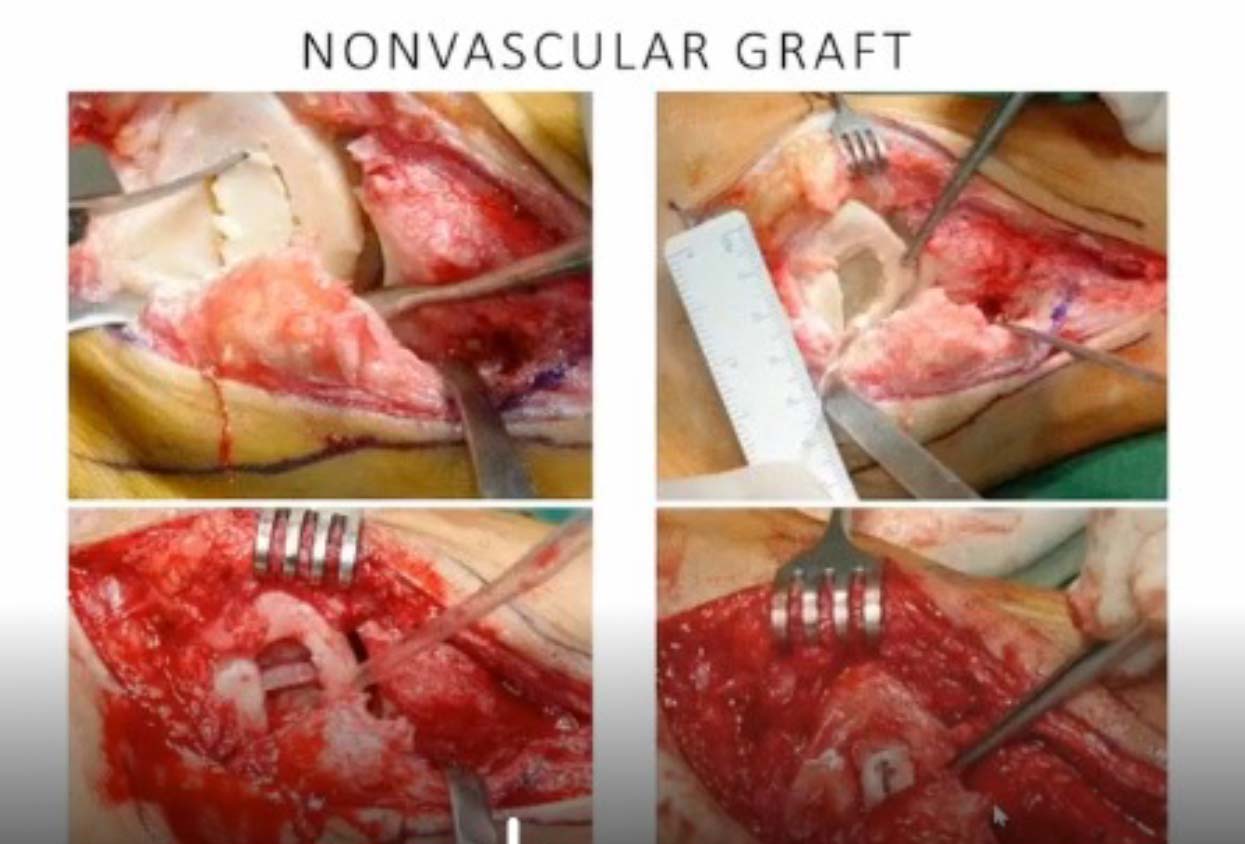
- Bone Grafting: Both vascularized and non-vascularized grafts can provide structural support and promote revascularization through creeping substitution. Non-vascularized grafts (eg, iliac crest) may offer structural support but not necessarily vascularization. Vascularized grafts (eg, pedicle from cuboid or calcaneal graft) are generally preferred for smaller, more superficial lesions (Hawkins/Fiscat 1–3) before true cortical collapse.
- Hindfoot Fusions (Arthrodesis): For cases involving true cortical collapse, hindfoot fusions have historically been considered the gold standard.
- Tibiotalocalcaneal (TTC) fusions are common for extensive talar death, though they are surgically challenging with varied functional results and higher non-union risks.
- Blair’s fusion, involving sliding and fusing the distal anterior tibia to the talus neck and head, is another option, though historical pseudoarthrosis rates led to modifications with IM nails or vascular grafts.
- Pantalar fusions can also be utilized, sometimes augmented with external fixators or IM nailing to improve structural support and vascular inflow. Clinical Tip: Remember that successful outcomes, even with fusions, may be defined as a braceable, stable, reasonably painless foot, rather than perfect anatomical union.
- Talar Prosthesis: This is an evolving and promising option. Partial talus prostheses have shown limited success, with total talus components generally recommended. Total talus prostheses can restore joint mobility, offer rapid pain relief, and may allow for shorter mobilization periods while preserving limb length.
- Clinical Tip: These customized implants often come with additional costs. There is growing interest in combining total talus prostheses with total ankle replacements, sometimes performed in a 2-stage technique with initial subtalar fusion to enhance blood supply.
Conclusion
The management of avascular necrosis of the talus remains a significant challenge for podiatrists. A comprehensive understanding of talar anatomy, meticulous diagnostic staging using imaging and classification systems, and a phased approach to treatment are critical. Initiating with conservative measures like prolonged non-weightbearing, complemented by newer modalities like extracorporeal shockwave therapy, offers hope for early-stage AVN. For advanced cases, while hindfoot fusions have traditionally been the mainstay, the advent of total talus prostheses presents an exciting and increasingly viable option, aiming to restore function and limb length. Early, honest discussions with patients about the high risk of AVN in severe talar injuries are paramount, preparing them for the potentially prolonged and complex course of recovery. Continued research, particularly into total talus prostheses and their long-term effects on adjacent joints, will undoubtedly further refine our approach to this challenging condition.
Christy M. King DPM, FACFAS is an experienced Foot and Ankle Surgeon and Residency Director with a demonstrated history of working in the hospital & health care setting. Skilled in Foot and Ankle surgery and clinical management, Resident and Student teaching, Healthcare Management, Healthcare, Sports Medicine, Clinical Research, and Pediatrics. Strong professional, graduated from Kaiser San Francisco Bay Area Foot and Ankle Residency Program.
This article is a summary of Dr. Kings’s presentation, “AVN After Talar Fracture ORIF, Now What?” from the 2025 APMA Surgical Complications Virtual Seminar on January 18, 2025. To view the full presentation with questions and answers—and see the agenda for the program, visit https://apmasurgical.lerexpo.com . Continuing education credits are available for this and many of the lerEXPO programs.





