
 By John Chuback, MD
By John Chuback, MD
Healthcare professionals are continually striving to improve patient outcomes through enhanced understanding and precise diagnosis. Yet, a significant pathological continuum, chronic venous insufficiency (CVI) and chronic venous disease (CVD), remains grossly underrecognized and misunderstood by many across the healthcare spectrum. This gap in knowledge often leads to delayed or incorrect diagnoses, suboptimal patient care, and unnecessary suffering for millions worldwide.
Congestive lower extremity failure (CLEF) is a novel concept, recently published in the Journal of Vascular Surgery: Venous and Lymphatic Disorders, that aims to demystify the complex pathophysiology of CVI by drawing a direct and insightful analogy to a condition profoundly understood by clinicians: Congestive heart failure (CHF). The motivation behind CLEF is simple yet profound: to translate the intricate cellular, molecular, and genetic complexities of CVI into a basic, understandable framework for all healthcare colleagues, from physicians and nurses to physician assistants and wound care specialists.
 The Urgent Need for a New Educational Model
The Urgent Need for a New Educational Model
For too long, CVD, particularly its earlier manifestations like varicose veins, has been mistakenly perceived as merely a cosmetic concern rather than a serious medical condition. This misperception, unfortunately, is still held by so many healthcare professionals, hindering the provision of optimal patient care and clinical outcomes. As a cardiac surgeon transitioning into the field of varicose vein treatment, I realized that venous issues were much more than varicose veins–they were part of a larger, complex clinical spectrum.
It was this background in open heart surgery that provided the crucial inspiration for the CLEF model and an obvious correlation between CHF as an educational model and CVI. By aligning the progression of CVI with the well-understood stages of CHF, CLEF offers a familiar and intuitive framework for clinicians to grasp the gravity and progressive nature of venous disease.
CLEF Explained: A Parallel Path to Organ Failure
 The genius of the CLEF concept lies in its parallel progression with CHF, highlighting shared underlying principles of congestion and progressive organ dysfunction. Let’s break down this powerful analogy:
The genius of the CLEF concept lies in its parallel progression with CHF, highlighting shared underlying principles of congestion and progressive organ dysfunction. Let’s break down this powerful analogy:
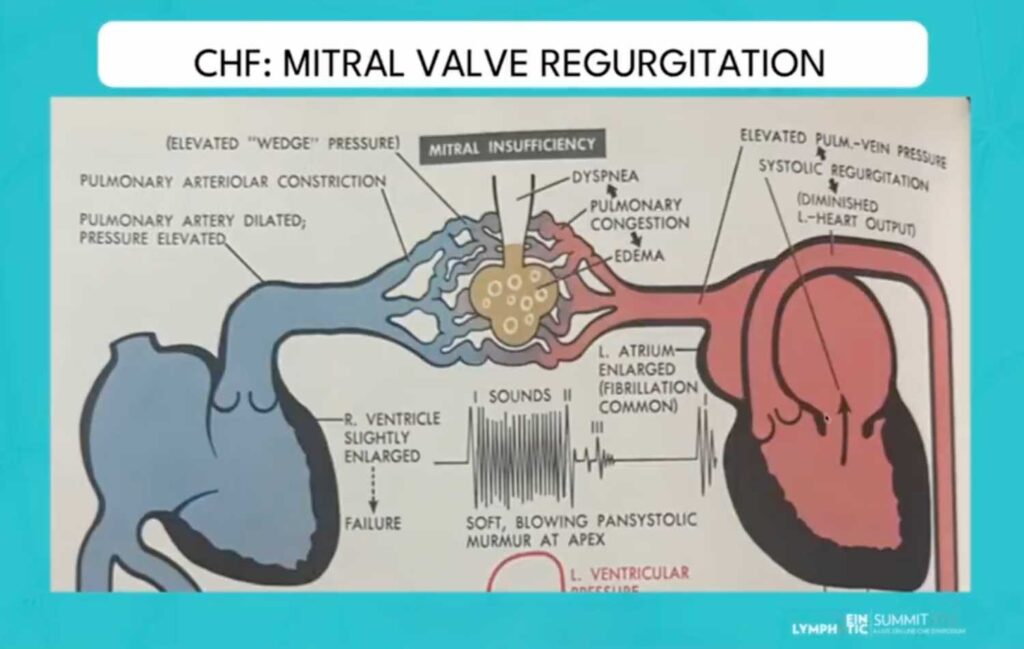
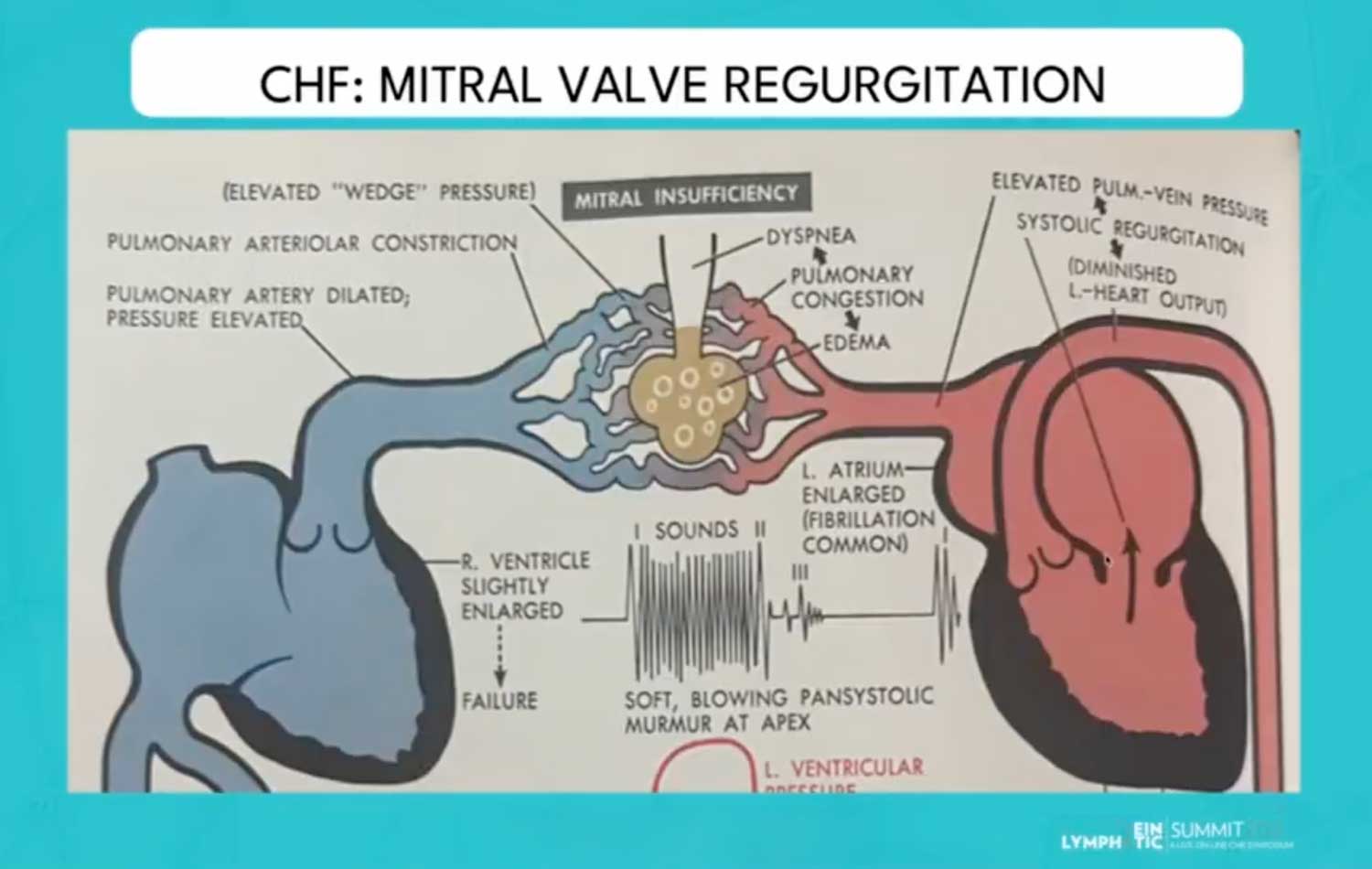
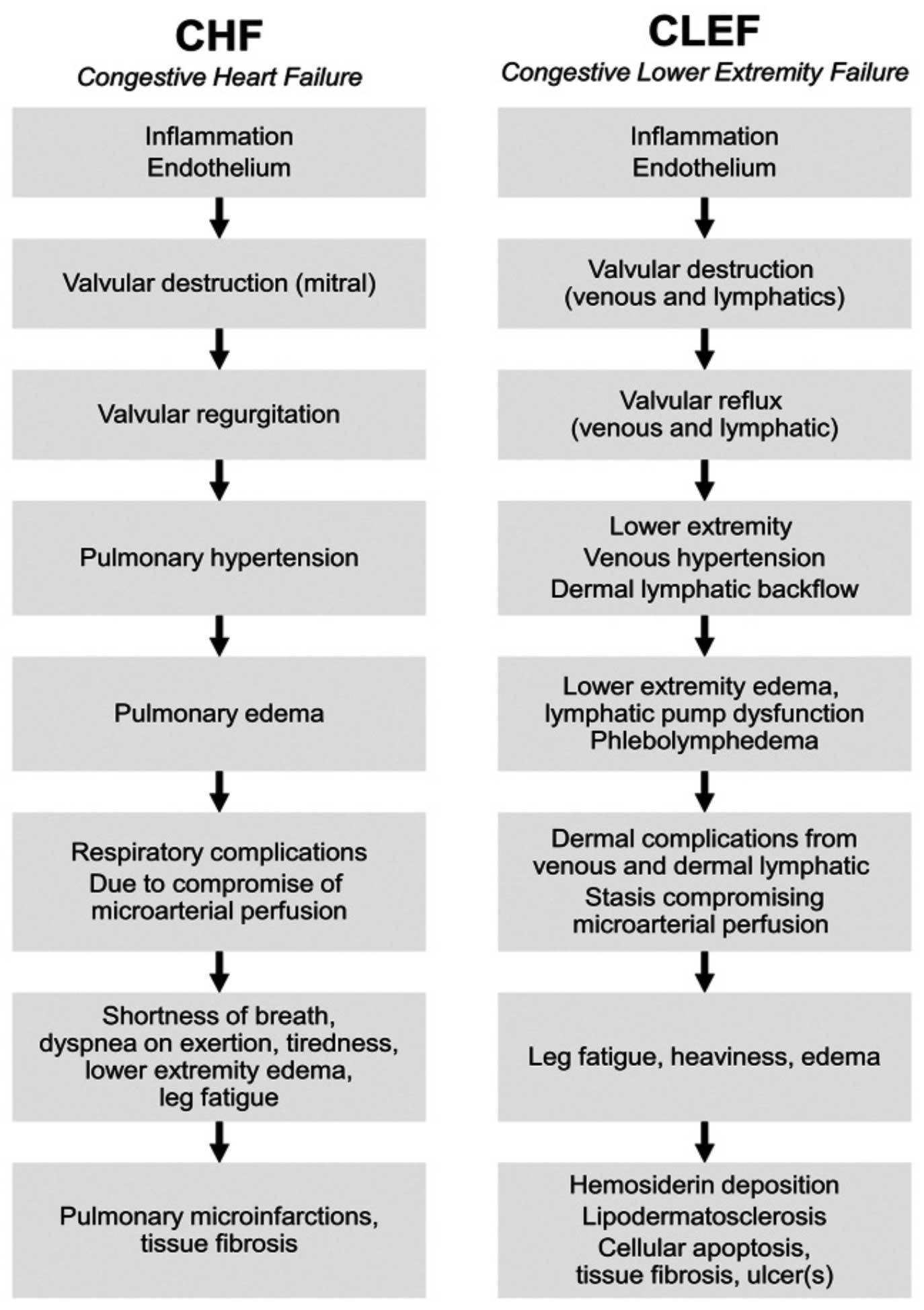
- Initial Pathological Event: Both CHF and CLEF begin with inflammation at the endothelial level. Under the common model for CHF, this leads to valvular destruction, particularly of the mitral valve. Similarly, in CLEF, this inflammation leads to valvular destruction of the venous valves.
- Early Effect and Backflow: This valvular damage leads to valvular regurgitation in CHF (ie, mitral valve regurgitation). In CLEF, this manifests as valvular reflux, such as saphenofemoral reflux, allowing blood to flow backward.
- Pressure Build-up: The consequence of this backflow is a rise in pressure. In CHF, we see pulmonary hypertension in the pulmonary veins. Analogously, CLEF involves lower extremity venous hypertension and dermal lymphatic backflow, as fluid struggles to return to the heart.
- Fluid Accumulation and Organ Overload: This elevated pressure leads to fluid accumulation. In CHF, this is pulmonary edema, a volume overload in the lung parenchyma. For CLEF, it results in lower extremity edema and phlebolymphedema, indicating a dysfunction and overwhelming of the lymphatic pump mechanism.
- Clinical Manifestations: The clinical symptoms of CHF include respiratory complications, dyspnea on exertion, fatigue, and lower extremity edema. In CLEF, patients experience leg fatigue, heaviness, persistent edema, and dermal complications like stasis, often accompanied by compromise of microarterial perfusion.
- End-Stage Complications: The progression culminates in severe organ damage. In CHF, this can lead to pulmonary microinfarctions, tissue fibrosis, and ultimately pulmonary failure. In the context of CLEF, the end stage is characterized by hemosiderin deposition, lipodermatosclerosis, cellular apoptosis, significant tissue fibrosis, and critically, venous leg ulceration.
Illustrating this analogy is a classic medical drawing of CHF by Dr. Netter and a compelling image depicting a normal leg versus one suffering from CLEF.
Another image shows a patient with end-stage CLEF (C6 disease), marked by severe venous hypertension, hemosiderosis, lipodermatosclerosis, venous dermatitis, active ulceration, and superficial thrombosis.
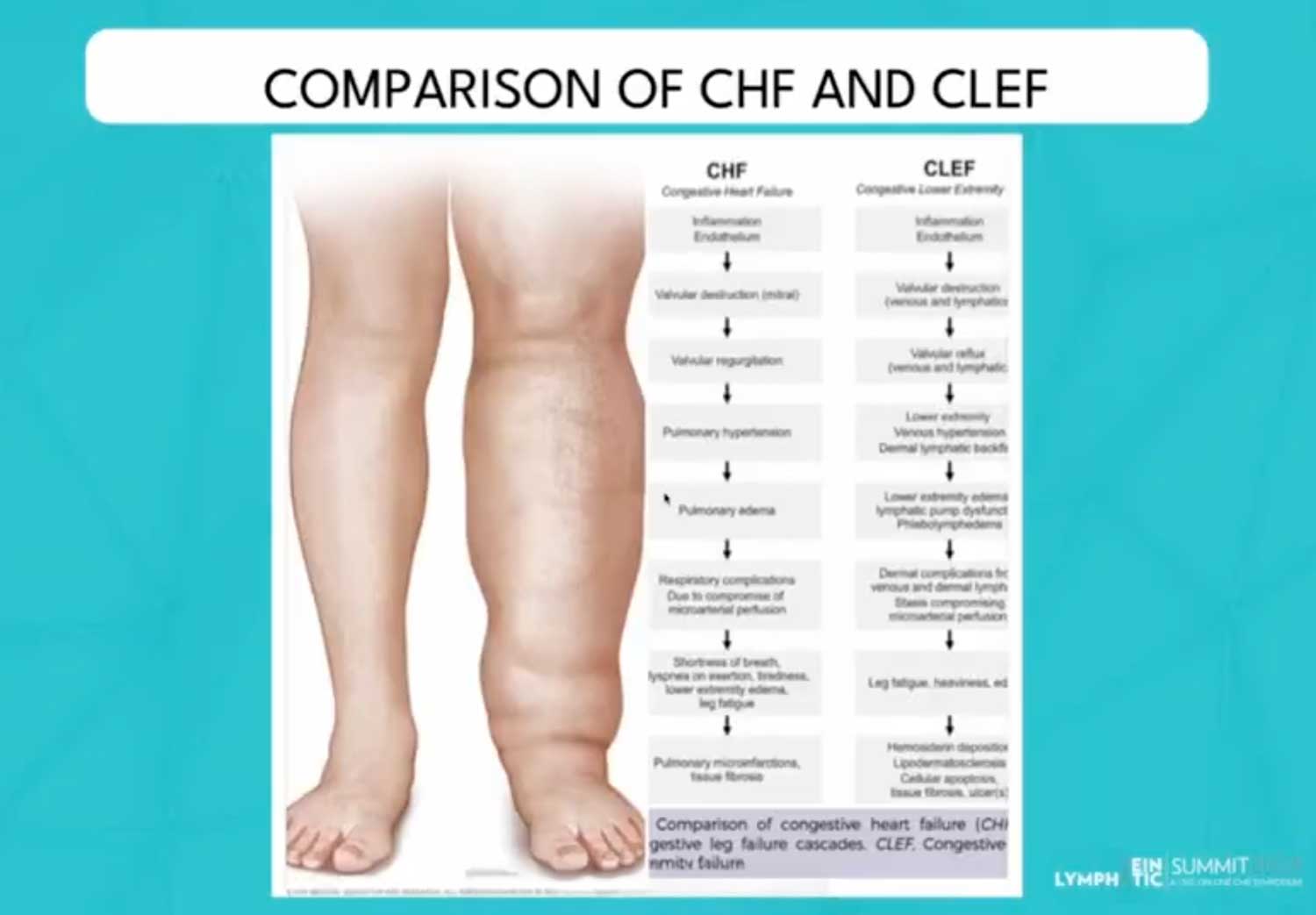 These visual aids powerfully convey the severity and progression of CLEF as a very real disease and pathology.
These visual aids powerfully convey the severity and progression of CLEF as a very real disease and pathology.
The Transformative Benefits of Increased Awareness
The adoption of the CLEF model promises significant benefits for patient care by fostering improved rates of recognition and accurate diagnosis among non-vein specialists and clinicians. This includes a wide array of healthcare professionals such as arterial surgeons, cardiologists, general surgeons, podiatrists, dermatologists, internists, and family practitioners.
Greater awareness directly translates to increased implementation of appropriate therapy and the full implementation of societal guidelines. This comprehensive approach includes:
- Compression therapy: A cornerstone of CVI management.
- Interventional procedures: Addressing both superficial and deep venous systems.
- Manual lymphatic drainage and lymphedema pumps: Crucial for managing the lymphatic component of phlebolymphedema.
- Oral venoactive agents: Such as micronized purified flavonoid fraction.
 Ultimately, the widespread education afforded by the CLEF model is projected to prevent progression to more advanced stages of CVD and prevent end-stage CLEF for millions globally. This will significantly assist in improving the quality of life and reducing suffering for those already symptomatic and diagnosed with advanced stages of CVI.
Ultimately, the widespread education afforded by the CLEF model is projected to prevent progression to more advanced stages of CVD and prevent end-stage CLEF for millions globally. This will significantly assist in improving the quality of life and reducing suffering for those already symptomatic and diagnosed with advanced stages of CVI.
CLEF is more than just a new term; it is a vital educational tool designed to underscore that CVI is a serious pathological continuum, not just a cosmetic problem. By embracing this paradigm, clinicians can enhance their diagnostic acumen, implement timely and effective treatments, and fundamentally transform the lives of countless patients suffering from this often-overlooked condition.
Dr. John Chuback is the founder of Chuback Vein Center, and is board-certified in Cardiovascular and Thoracic Surgery, and is a Diplomate of the American Board of Venous and Lymphatic Medicine. Dr. Chuback is also the founder of VItasupportMD, a brand of doctor-formulated dietary supplements that support healthy veins, lymphatics, and circulation.
This article is a summary of Dr. Chuback’s presentation, ”Congestive Lower Extremity Failure (CLEF): A Novel Educational Model for Improved Understanding of Chronic Venous Insufficiency and Associated Advanced Stage Consequences,” from the 2024 Vein Lymphatic Summit held July 19–20, 2024. To view the full presentation with questions and answers and see the agenda for the 2-day program, visit https://vls24.lerexpo.com/ . Continuing education credits are available for this and many of the lerEXPO programs.





Thank you for a extremely interesting and important comparison of two pathologies, certainly similar to our frequently Diabetic patients with prep with both peripheral arterial disease and carotid and cardiovascular arterial disease
Very interesting and important analogy
Once again thank you I very much enjoyed reading your article