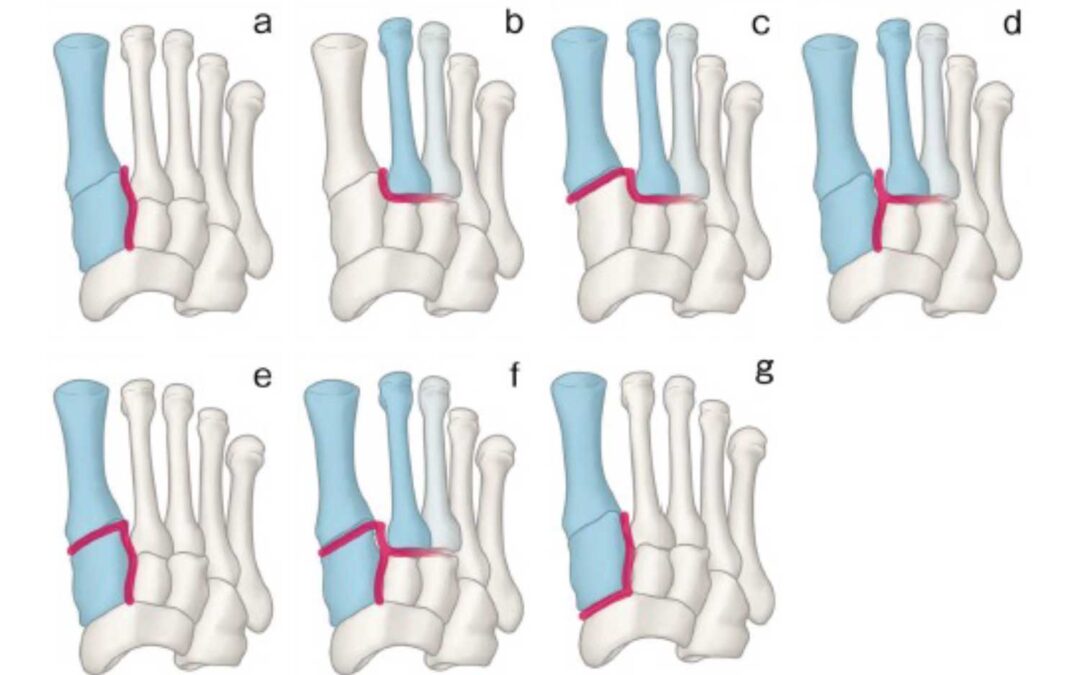
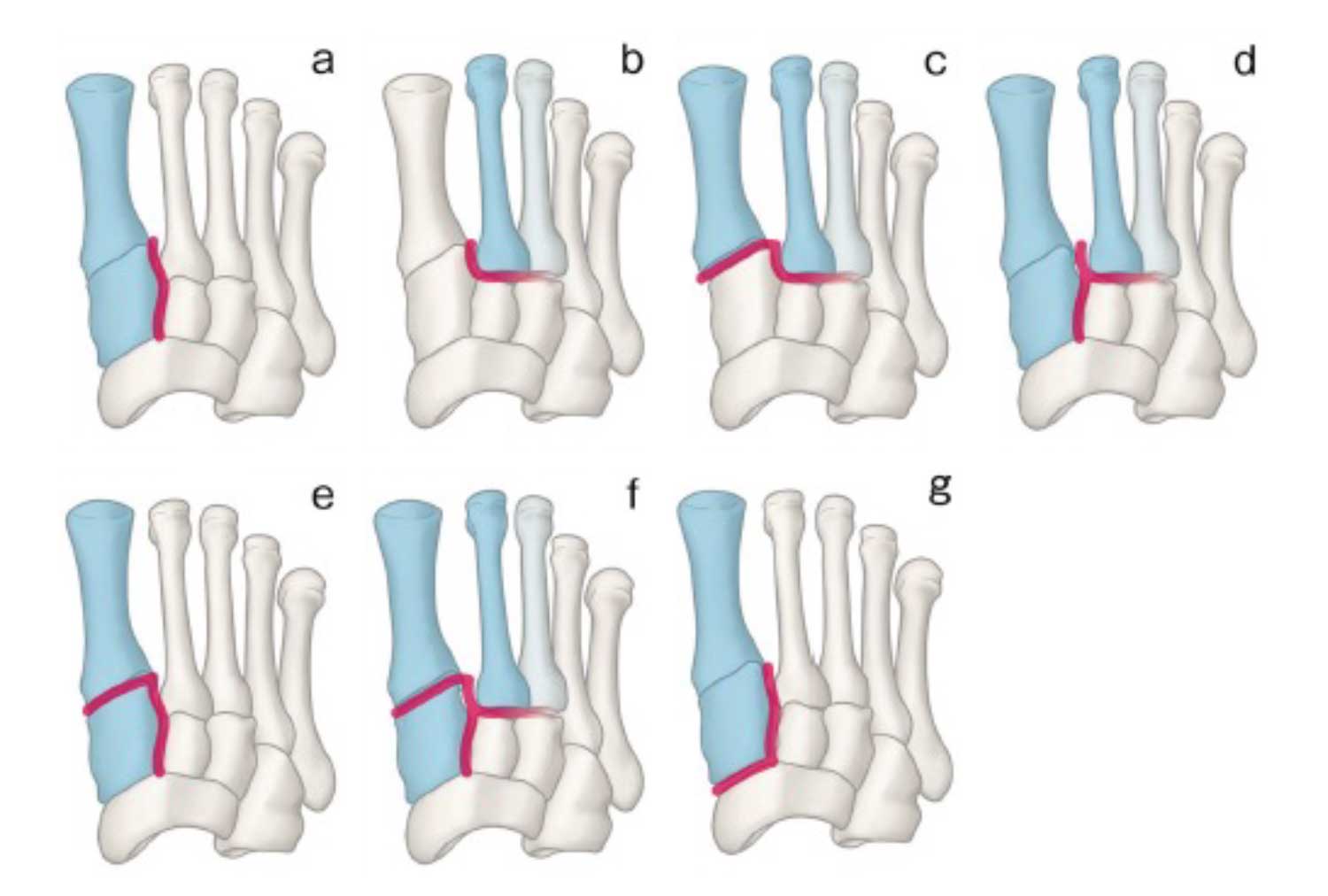
Patterns of Subtle Lisfranc Injury. The injured joints are indicated in red. (a) Longitudinal type injury. (b) Transverse type injury. In some patients with this type of injury, the joint between the third cuneiform and third metatarsal may be involved. (c) Transverse type injury combined with first tarsometatarsal joint injury. (d) Longitudinal type injury plus transverse type injury. (e) Longitudinal type injury plus first tarsometatarsal joint injury. (f) Longitudinal type injury, transverse type injury, and first tarsometatarsal joint injury. (g) Longitudinal injury extending into the naviculo-first cuneiform joint. Source: Haraguchi N, Ota K, Ozeki T, Nishizaka S. Anatomical pathology of subtle Lisfranc injury. Sci Rep. 2019;9(1):14831. doi: 10.1038/s41598-019-51358-8.
Lisfranc injuries, once described fracture-dislocations of the tarsometatarsal joints and considered rare, are now recognized to occur more frequently and in subtler forms due to advancements in imaging. These injuries vary significantly in severity and anatomical presentation. Early diagnosis is critical for favorable outcomes. Traditional anatomy-based classification systems have limited treatment utility. This review supports a stability-based classification, emphasizing the role of weight-bearing radiographs and CT in diagnosis.
Stable Lisfranc injuries typically respond well to nonoperative treatment-immobilization and non-weightbearing for 6 weeks. Unstable, displaced, or comminuted injuries require surgical intervention, most commonly open reduction and internal fixation (ORIF), with a growing preference for bridge plating. ORIF generally achieves good outcomes but is less predictable in high-energy trauma. Primary arthrodesis is less commonly used in acute settings but may reduce post-traumatic arthritis and hardware removal.
Emerging techniques like suture button fixation offer flexible stabilization with the potential to improve midfoot biomechanics and reduce complications, though more data is needed. Future research should aim to refine classification systems, validate weight-bearing CT, enhance rehabilitation strategies, and tailor surgical methods to specific injury types to optimize outcomes.
Source: Poutoglidou F, van Groningen B, McMenemy L, Elliot R, Marsland D. Acute Lisfranc injury management. Bone Joint J. 2024;106-B(12):1431-1442. doi:10.1302/0301-620X.106B12.BJJ-2024-0581.





