 Background: Osteochondromas are the most prevalent benign bone tumor, occurring mostly in the long bones of the leg, thigh, and arm. Representing 20%–50% of benign tumors, osteochondromas are rarely symptomatic. Most symptomatic cases are linked to posttraumatic conditions or idiopathic causes. Although conservative management is recommended, surgical removal may be necessary for recalcitrant cases. This is a Type 3 clinical CASE study.
Background: Osteochondromas are the most prevalent benign bone tumor, occurring mostly in the long bones of the leg, thigh, and arm. Representing 20%–50% of benign tumors, osteochondromas are rarely symptomatic. Most symptomatic cases are linked to posttraumatic conditions or idiopathic causes. Although conservative management is recommended, surgical removal may be necessary for recalcitrant cases. This is a Type 3 clinical CASE study.
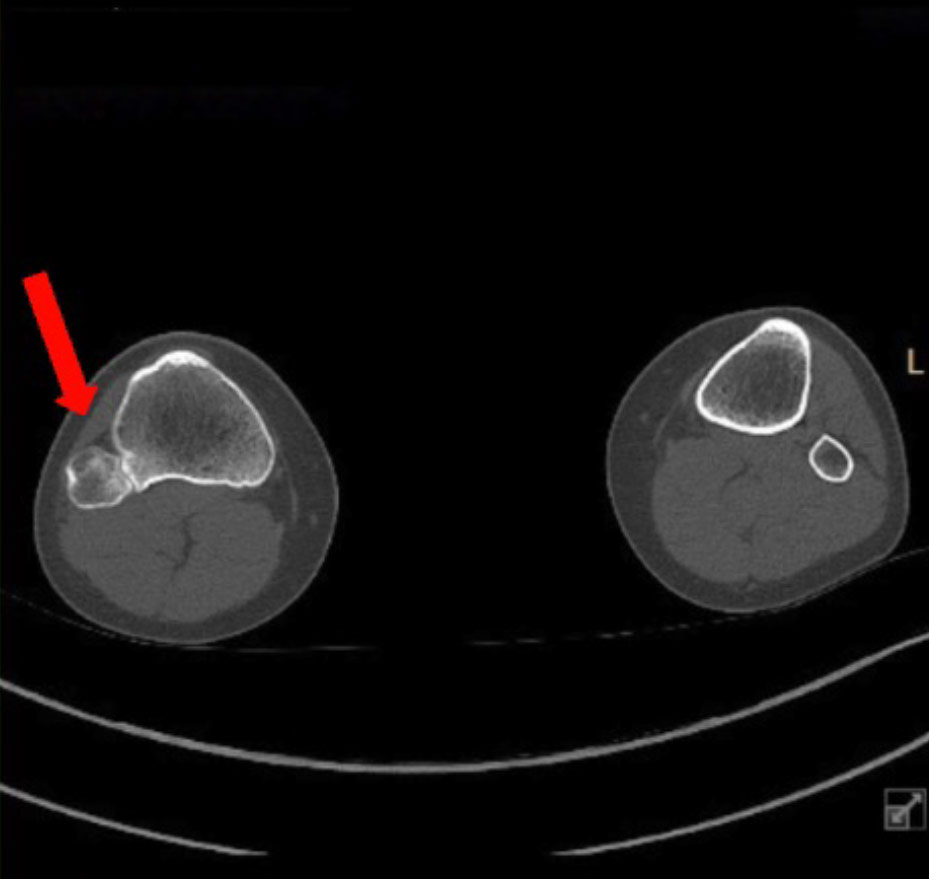
Patient: Patient is a 20-year-old female Division-3 soccer player who presented to her AT complaining of insidious onset right posterolateral knee pain. Past medical history of a right medial malleolus fracture, multiple ipsilateral inversion ankle sprains, bilateral medial tibial stress syndrome, and polycystic ovary syndrome. Patient was point tender over anterior tibialis and fibularis muscles, reported pain with active dorsiflexion and inversion, passive eversion, and pain without weakness during anterior tibialis and fibularis tertius MMT. Differential diagnoses included fibularis strain and anterior tibialis strain. After initial treatments failed, she was referred to the team physician 2-months after onset. Radiographs revealed increased bone density at the fibular head, indicative of a healing fracture. MRI confirmed diagnosis of a fibular head stress fracture. Patient was placed NWB in a walking boot for 8 weeks and began a rehabilitation program with her AT focused on pain modulation and general ankle and hip strengthening. Due to persistent pain, a CT scan and second MRI were ordered 7 months after initial onset. CT revealed a proximal tibiofibular synostosis secondary to an osteochondroma (figure).
Intervention & Treatment: Patient was given a tall walking boot to wear PRN and resumed rehabilitation as previously described. A cortisone injection within the interosseous space was administered 8 months after initial onset, however her pain persisted. Two months later she underwent a resection of the osteochondroma and neuroplasty of the common fibular nerve. Although outcomes for this type of surgery are generally positive, postoperatively the patient reported posterolateral knee pain and radiating pain into her foot despite continued therapeutic interventions including nerve desensitization therapy. Four months postoperatively she developed a foot drop and has since failed to make a full RTP.
Outcomes or Other Comparisons: In this case, the patient continued experiencing pain and developed foot drop postoperatively. Although fibular nerve lesions and symptomatic osteoarthritis are reported complications of surgery, resection of the fibular head is a commonly performed surgical technique for symptomatic proximal tibiofibular synostosis. Most of the previously documented cases are idiopathic, with no real causal events in the patient’s medical history. Repetitive microtrauma is thought to be a possible mechanism for proximal tibiofibular synostosis in patients who do not report specific trauma, such as this case.
Conclusions: This case report presents the treatment of a proximal tibiofibular synostosis caused by an osteochondroma in a female soccer player. When symptomatic, the clinical presentation of osteochondromas may differ greatly, making accurate diagnosis difficult. As was the case with this patient, common symptoms include knee pain and pain with ankle dorsiflexion. Although diagnosis can be made through radiographs, this case highlights limitations of this imaging modality. CT or MRI are recommended for making a definitive diagnosis and for determining whether surgical intervention is necessary. Conservative treatment is recommended for patients with few symptoms, but surgical intervention is recommended when conservative treatment fails. The most common procedures include excision of the synostosis, arthrodesis of the proximal tibiofibular joint, and resection of the fibular head.
Clinical Bottom Line: While proximal tibiofibular synostosis caused by an osteochondroma is uncommon, clinicians should be aware of the potential causes, common clinical presentation, and diagnostic imaging required to make a definitive diagnosis. Often mistaken for muscle strains or sequelae of lateral ankle sprains, osteochondromas of the proximal tibia and fibula should be considered as a differential diagnosis in patients presenting with posterolateral knee or ankle pain.
Source: Roth A, Bortz C, Wilkenfeld DA. Proximal Tibiofibular Synostosis in a Female Soccer Athlete. J Athl Train. 2023;58(6S):167. Used with permission; all rights reserved.





