 By Pamela K Hale, CPO
By Pamela K Hale, CPO
Gait, refers to the manner in which a person walks, is fundamental not only to physical health but also to overall quality of life. Achieving a near-normal gait pattern when providing rehabilitative care is crucial for several reasons: optimizing biomechanical efficiency, improved minimizing secondary health issues, enhancing psychological well-being, and improving social integration.
CASE 1: Knee Instability and Osteoarthritis
Fitzgerald, et al1 concluded that, “a substantial proportion of individuals with knee OA report episodes of knee instability during activities of daily living. Instability affects physical function beyond that which can be explained by contributions from other impairments such as knee pain, range of motion, and quadriceps strength. Knee instability is a problem that should be specifically addressed in rehabilitation programs and may require interventions beyond those that address pain, joint motion, and muscular strength, to maximize the effectiveness of rehabilitation for individuals with knee OA.”
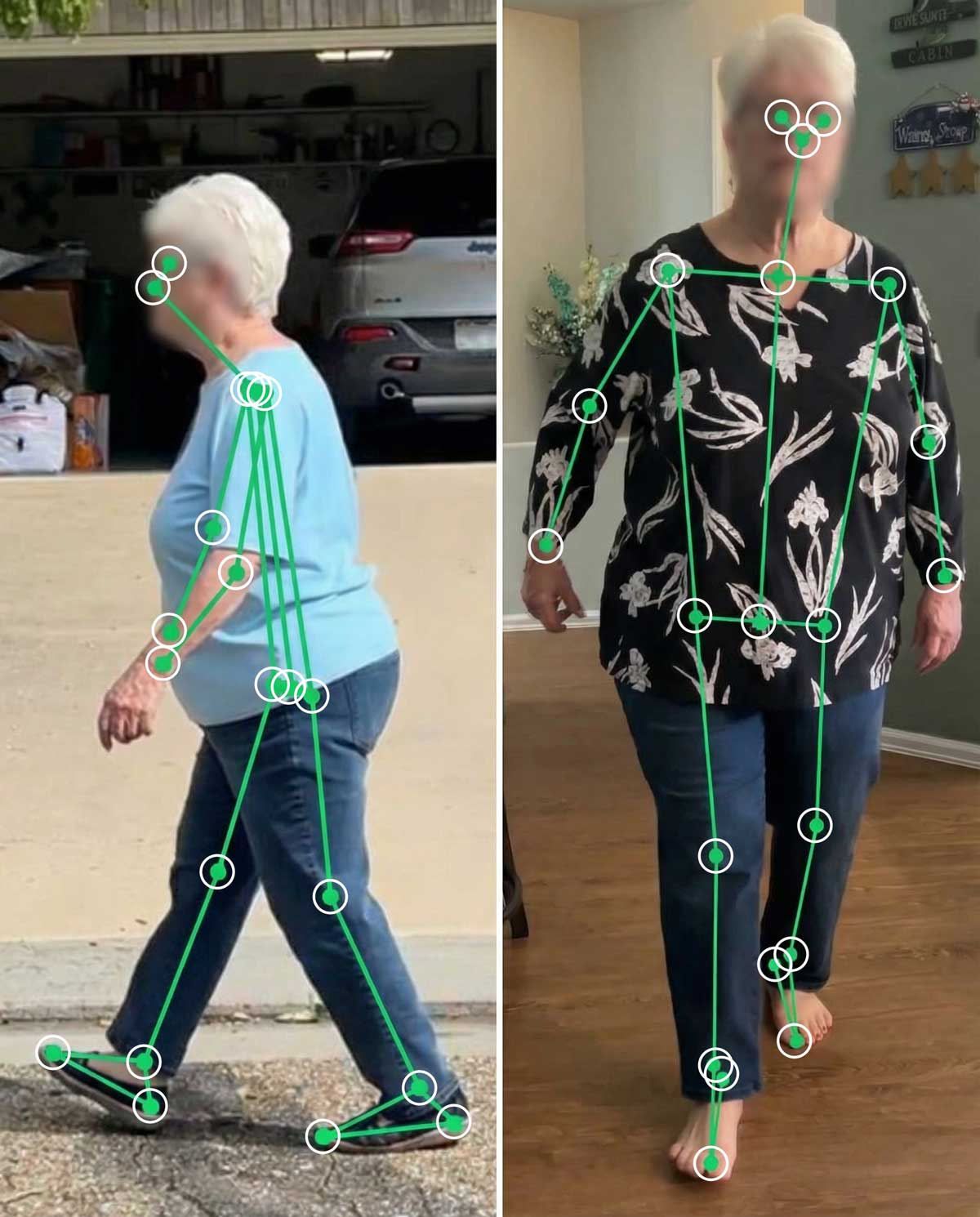
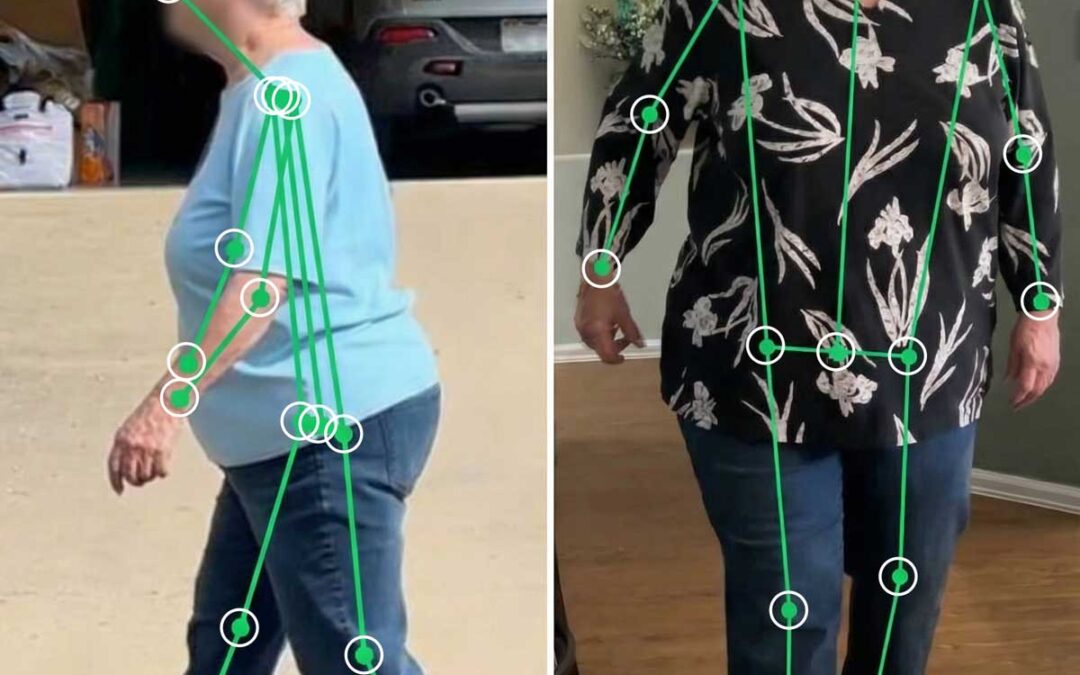
Terminal Stance Left Leg. The VISION app uses AI to identify the joint position
JS is a patient diagnosed with osteoarthritis (OA) affecting her left knee. She reported significant lifestyle changes due to her condition, including the necessity to sell her house. This decision was prompted by her inability to manage physical challenges such as the slight elevation in her backyard, stairs leading to the basement, and walking distances greater than 15 feet at a time.
JS’s primary limitation was not pain, but rather a persistent fear of her knee “giving out,” which contributed to her concern about potential falls. Despite having experienced episodes where her knee did “give out” and having fallen as a result, she did not qualify as a candidate for knee replacement. This was primarily because she did not report significant pain, although she exhibited radiographic evidence of medial compartment osteoarthritis, loss of function due to fatigue and fear, reduced mobility, limited range of motion for knee extension, and genu varum.
During ambulation, JS demonstrated a notably slow gait. She frequently reached for walls to support herself while walking, underscoring her instability and apprehension about falling.
To gain a clearer understanding of JS’s gait abnormalities and knee instability, a video recording was obtained capturing her walking from both the coronal (front/back) and sagittal (side) views. This visual assessment allows for detailed observation of her movement patterns, providing valuable insight into the specific deviations and challenges she faces during ambulation.
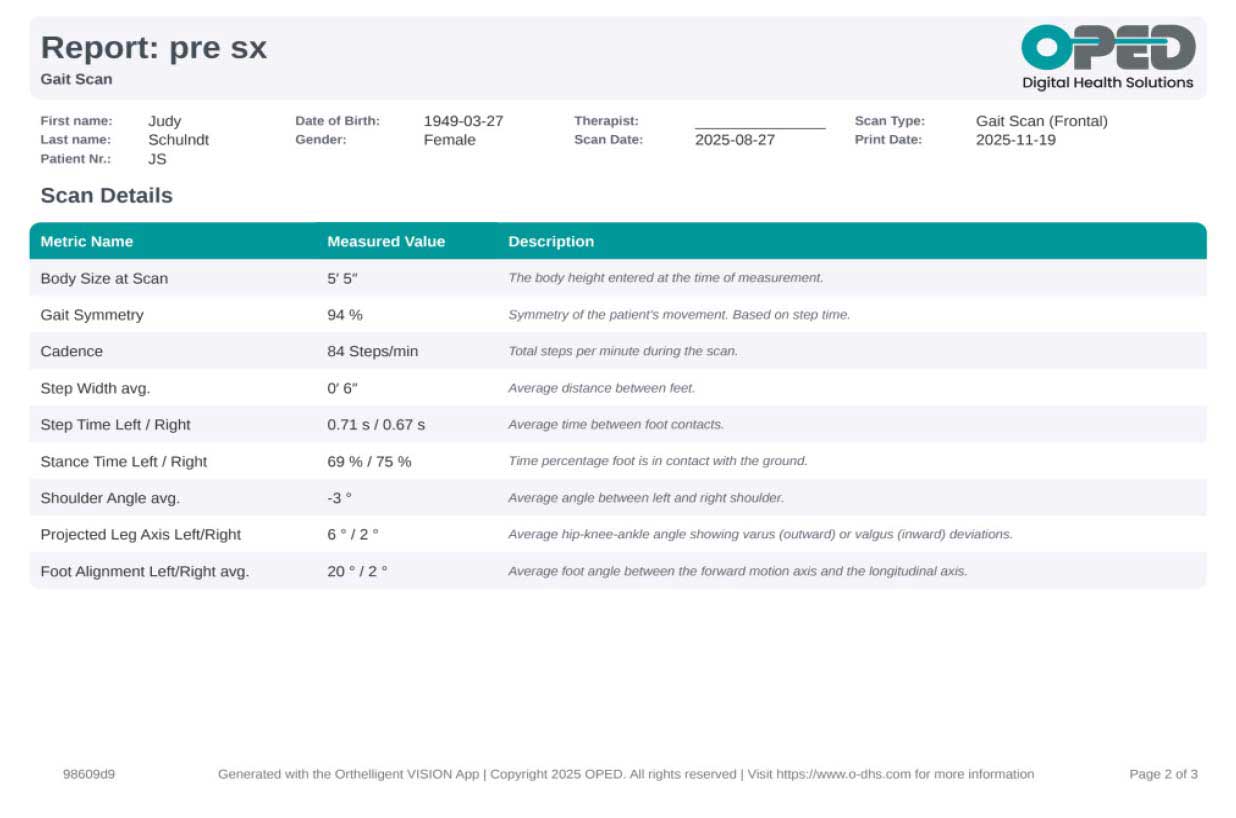
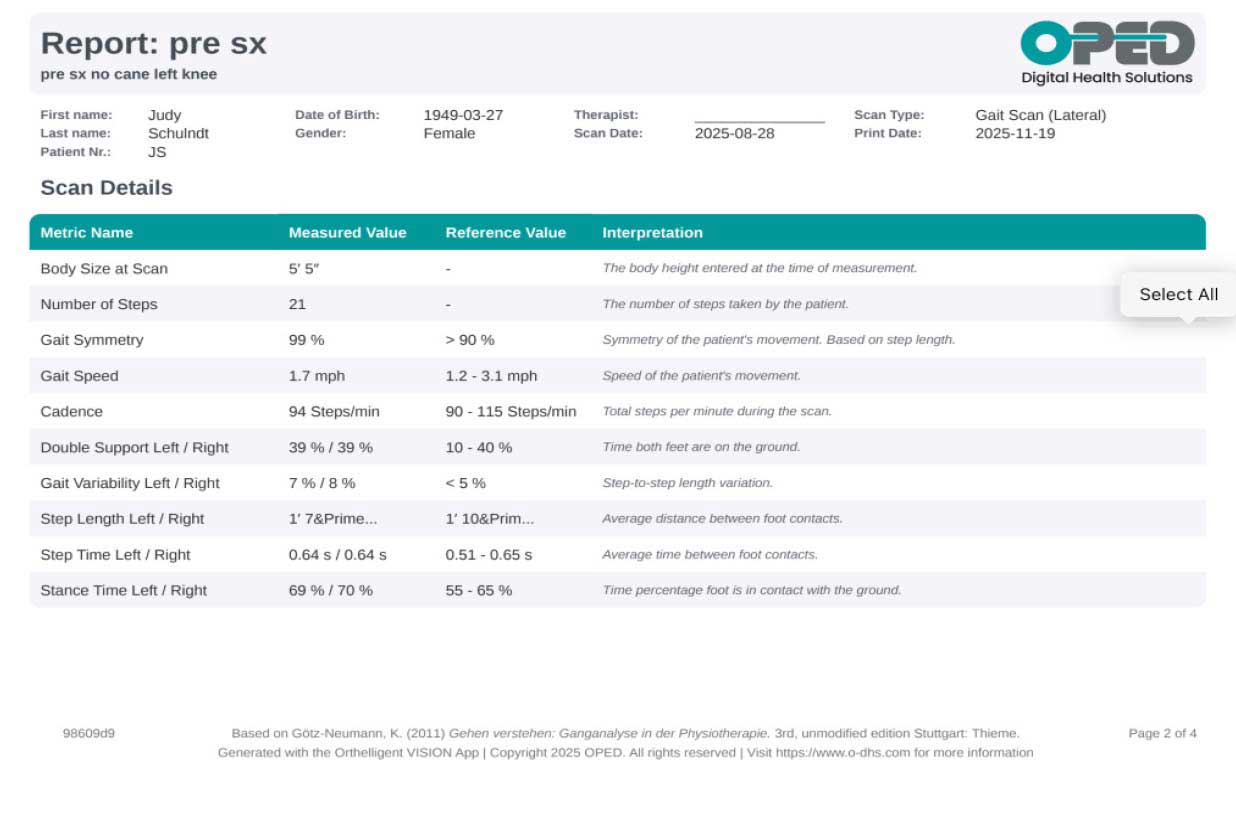
To further evaluate JS’s gait abnormalities and knee instability, the Orthelligent® VISION Gait Analysis application2 by OPED was utilized. This advanced assessment tool was used to analyze her walking patterns in detail. The objective reports generated by the application provided comprehensive temporal-spatial data, such as walking speed and time spent in various phases of the gait cycle, as well as joint angle data for a precise understanding of her movement deviations. These quantitative insights complemented the visual and subjective assessments, offering a thorough overview of JS’s gait characteristics and informing subsequent intervention strategies.
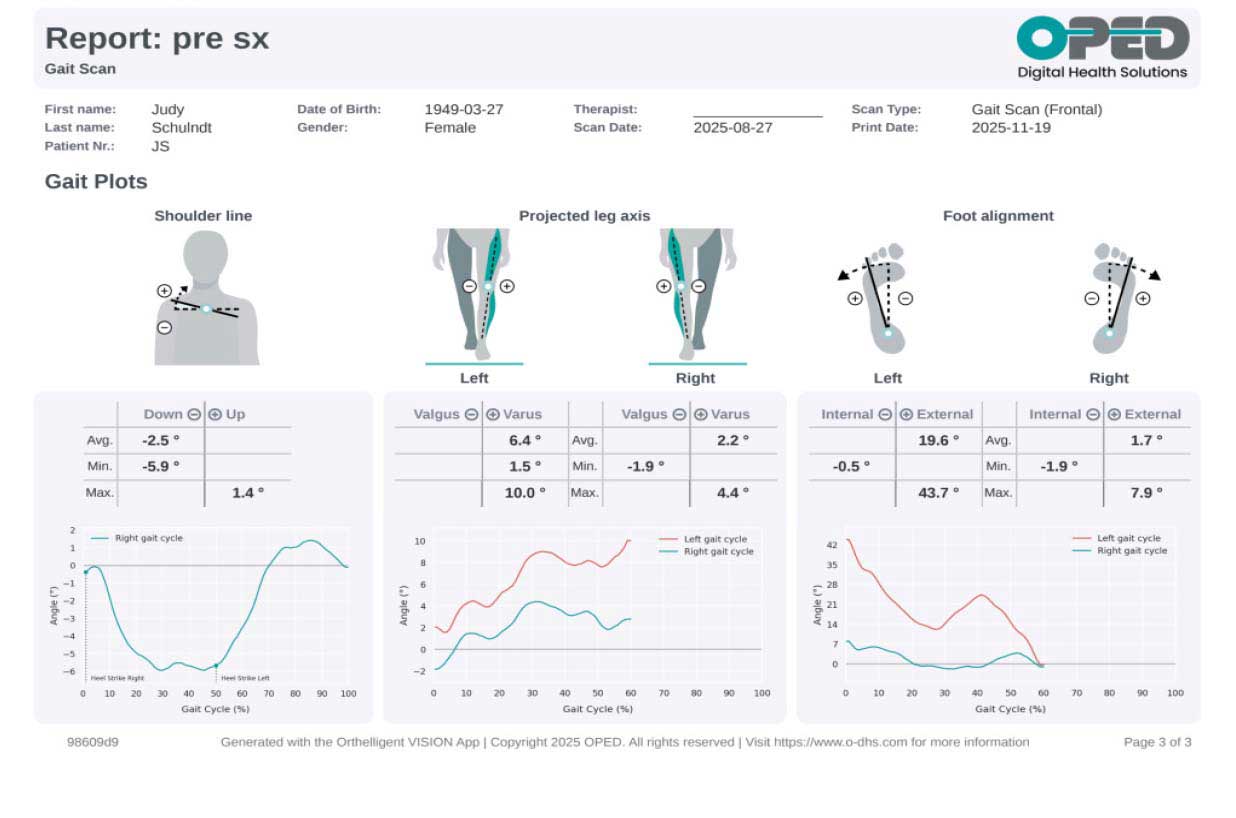
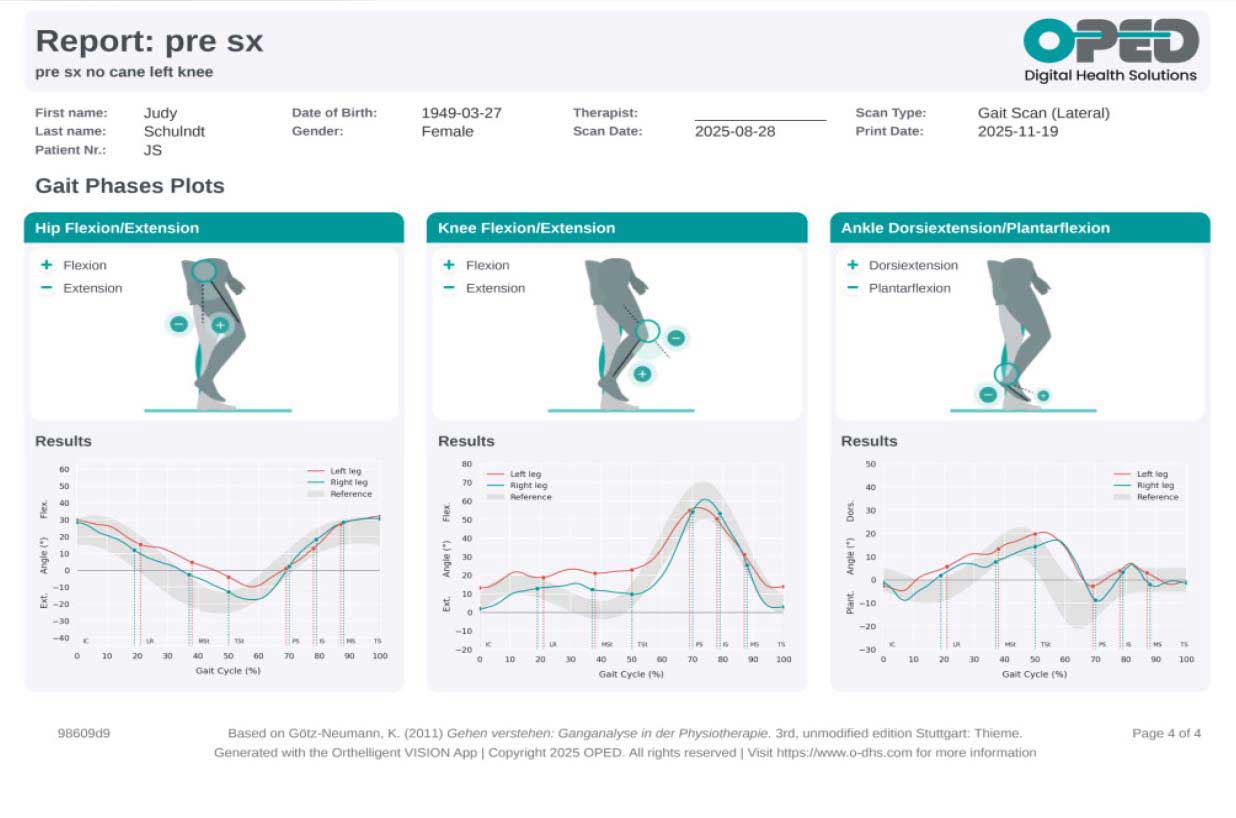
While the joint angle graphs provided by the application showed pronounced deviations during terminal stance. These included increased hip flexion, increased knee flexion, and increased ankle dorsiflexion angle and prolonged dorsiflexion. Such findings suggest that JS’s gait is characterized by compensatory movements, likely resulting from her underlying knee instability and related osteoarthritis. These objective measurements offer valuable insights into the specific biomechanical challenges she faces and help guide targeted interventions for her rehabilitation.
A subjective assessment of JS’s left leg was conducted before any interventions were implemented. During terminal stance, observed from the sagittal view, there was noticeable hip flexion, knee flexion, and ankle dorsiflexion. When examining the coronal view, genu varum was present, accompanied by ankle dorsiflexion and an outward rotation “toe out” of the foot. Although a complete video was available for review, a representative screenshot was utilized to capture the left leg at terminal stance, corresponding to approximately 50% of the gait cycle.
The objective data obtained from the VISION Gait Analysis application, specifically from the lateral (sagittal) view, revealed several key abnormalities in JS’s walking pattern. The analysis demonstrated a noticeably slow walking speed, which was accompanied by an increased duration of double limb support—meaning JS spent more time with both feet on the ground during walking. Additionally, there was a bilateral increase in stance time, indicating prolonged periods where each foot remained in contact with the ground.
Joint angle graphs generated by the application revealed a noticeable shoulder line asymmetry between the left and right sides, suggesting compensatory postural adjustments during walking. The data also confirmed the presence of left genu varum and external alignment of the left foot, both of which contribute to JS’s overall instability and altered gait mechanics.
JS demonstrates abnormalities across the sagittal, coronal, and transverse planes, all of which contribute to her impaired knee stability, diminished function, and reduced endurance during ambulation. Specifically, persistent knee flexion and ankle dorsiflexion are observed throughout the stance phase of gait. This combination creates a knee flexion moment that requires JS to generate stability either through concentric contraction of the quadriceps to extend her knee, or via eccentric contraction of the soleus muscle to slow the forward movement of the tibia.
However, both the knee and ankle are positioned in a biomechanical disadvantage, meaning they are unable to generate sufficient force to effectively control further knee flexion or ankle dorsiflexion during the stance phase. As a result, JS adopts compensatory strategies to manage these challenges. The primary compensatory mechanism involves reducing the duration of single limb support on the affected limb. This is typically achieved by either shortening her step length or increasing the amount of time spent in double limb support, where both feet are in contact with the ground.
The VISION Gait Analysis application’s objective data from the coronal view highlighted several asymmetries and deviations in JS’s gait pattern. Specifically, the analysis reported differences in stance time between the left and right sides, indicating that JS spends less time on her left leg during ambulation. Additionally, discrepancies in leg axis and foot alignment were observed, reflecting further biomechanical challenges.
The implications of these abnormalities are reduced mobility, continued joint deterioration at the left knee or in other joints as well as, reduced range of motion.
What are possible interventions?
- Through PT Improving range of motion, strength and posture.
- Utilize a cane or walker.
- Support the knee with an Unloader Brace.
- Surgical intervention.
- Is there more?
In the next installment we will explore the initial effect of using a cane. And check in with JS regarding her journey.
As a Certified Prosthetist and Orthotist, Pamela K Hale is a nationally recognized speaker and works with clinicians to assess movement patterns and recommend solutions. Her expertise helps improve patient mobility and supports the rehabilitation of those with movement challenges.