
 By Victoria Exley, BSc (Hons ) Pod, MSc; Katherine Jones, PhD; Grace O’Carroll, PhD; Judith Watson, PhD; and Michael Backhouse, PhD
By Victoria Exley, BSc (Hons ) Pod, MSc; Katherine Jones, PhD; Grace O’Carroll, PhD; Judith Watson, PhD; and Michael Backhouse, PhD
Ingrown toenails (onychocryptoses) are one of the most common nail pathologies, yet there is a lack of data to assess the evidence surrounding the nail surgery procedures from which clinicians must choose.
When performing nail surgery, clinicians must choose from a multitude of procedures and variations within each procedure. While much has been published to guide this decision making, there is a lack of up-to-date, robust systematic reviews to assess the totality of this evidence. This second paper by the same authors reports outcomes on healing time, post-operative complications, pain, and participant satisfaction.
Methods
Five databases (MEDLINE, Embase, CINAHL, Web of Science and CENTRAL) and 2 registers (Clinicaltrials.gov and ISRCTN) were searched to January 2022 for randomized trials evaluating the effects of a surgical intervention(s) for ingrown toenails. Data on co-primary outcomes of symptom relief and symptomatic regrowth were presented in the study authors’ first paper. This paper presents data for the secondary outcomes and further discussion.
Results
Of 3,928 records identified, 36 randomized trials were included in the systematic review. Healing time appears to be reduced with shorter application of phenol. A reduced healing time was also apparent with the addition of curettage, although this may also increase the risk of postoperative bleeding and pain. Postoperative bleeding was also reportedly lower in people who received local anesthetic with epinephrine but no tourniquet. Use of phenol with nail bed excision may decrease the risk of infection. Lower pain scores were reported when using partial matrixectomy and surgical interventions with phenol. Shorter duration of pain was reported with phenolization and wedge resection. Participant satisfaction was high overall.
Risk of bias was assessed for 6 domains in each study (Figure 1).
Discussion
This is the second paper from the same authors of this systematic review and meta-analysis of randomized controlled trials of surgical treatments for ingrown toenails. The first reported the methods used in the review and reported results from the primary outcomes of recurrence and relief of symptoms. This second paper focuses on the secondary outcomes of healing time, postoperative complications (eg, infection and hemorrhage), postoperative pain (duration and intensity), and participant satisfaction. Although a large number of trials were identified for inclusion in the review, the poor reporting, heterogeneity of the studies and differences in outcome measures/timepoints, meant a meta-analysis was not possible on these secondary outcomes.
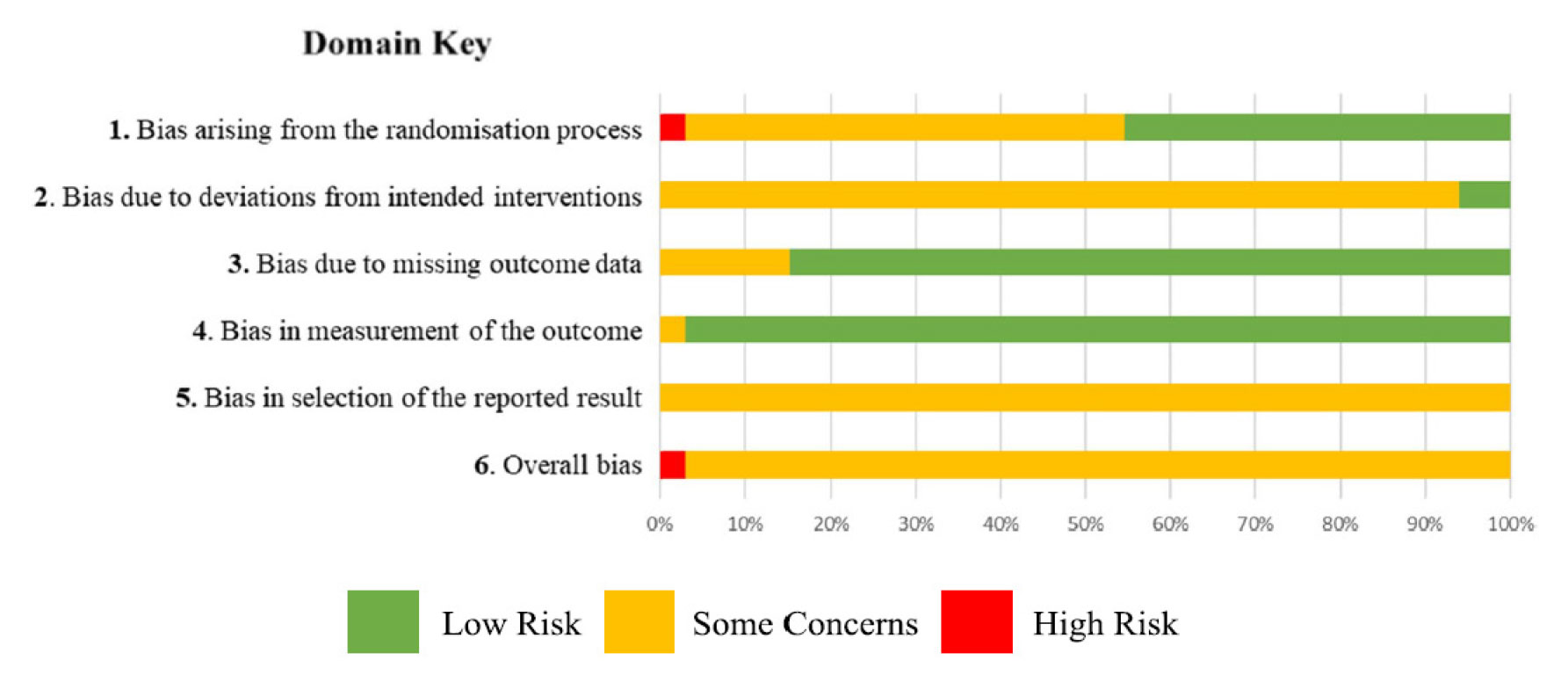
Figure 1. Risk of bias summary plot: RoB 2.0 tool.
Perhaps the most obvious clinical finding from this is the lack of robust clinical conclusions that can be drawn from all these studies. Possibly the clearest pattern to emerge was around the use of phenol. Shorter application of phenol during the chemical matrixectomy was linked to shorter time to healing in 2 studies, but application duration appeared to have little effect on postoperative complications. Although this may suggest that clinicians should use a shorter duration of phenol, this must be balanced against the meta-analysis in the first paper which indicate higher rates of regrowth are associated with shorter application times. The optimal balance of effectiveness and sequalae is yet to be determined and clinicians may opt to vary application times to meet the needs of individual patients.
Curettage has been explored in several studies. Alvarez-Jimenez et al. reported that using a Martini bone curette following partial nail avulsion and destruction of the nail matrix with phenol reduced healing time by a third (7.5 ± 1.8 days compared to 12.4 ± 3 days, p = 0.001). They also found that it reduced rates of postoperative infection, but increased postoperative bleeding and as reported previously had no effect on recurrence. However, with only 51 patients, and that this has not been tested in multiple trials, care must be taken not to over-interpret these findings. It is notable that while interventions such as curettage may benefit some outcomes such as healing, it may increase others such as postoperative bleeding. A similar pattern was found with phenol where longer durations of application were linked to reduced likelihood of regrowth but increased healing times. Clinicians and future studies should prioritize these competing risks and benefits in a way that prioritizes what is important to patients.
Many studies report infection rates following nail surgery but combining these isn’t yet possible as case definitions are unclear and inconsistent. Standardized definitions of surgical site infections and severity classifications exist and have been used in other fields of surgical research, but they have not yet been validated and applied to nail surgery. Despite the clear interest in postoperative infection as an outcome, only 1 trial explored the use of oral antibiotics and found no evidence that they reduced the rate of postoperative infection. However, with only 50 to 53 participants per group, it would only have been powered to identify a large effect.
Other postoperative sequalae, such as hemorrhage, also had unclear case definitions and were poorly reported. With some studies only capturing data for some outcomes up to 48 hours post procedure, there is not enough time to meaningfully assess the effect of an intervention on complication rates. Perhaps more worryingly, there was a lack of information on the reporting of adverse events in general despite clear legal and governance frameworks being in place for many years.
Another frequently captured outcome was patient satisfaction. This is a widely used, but poorly defined concept in healthcare and although definitions vary, they generally center on satisfaction being the extent to which an individual’s experience meets their expectations. However, patient expectations are not a stable trait and change over time as has been recognized elsewhere. Evidence from randomized trials have shown that patient expectations can be deliberately modified, and that patient expectations can be guided toward what clinicians consider achievable. Modification of patient’s expectations would in turn influence their final level of satisfaction, which brings into question its value as a measure of treatment effectiveness.
Given the limitations of the studies identified in this review, it’s clear that many fundamental questions remain unanswered around the surgical treatment of ingrown toenails: Is destruction of the nail matrix always necessary? What is the optimal technique to prevent symptomatic regrowth? How should patients be reviewed and monitored postoperatively? Are different procedures more appropriate for subgroups of patients? Further high-quality collaborative trials are needed to answer these questions.
Conclusion
This second paper reports secondary outcomes from a robust systematic review of randomized trials on surgical treatment of ingrown toenails. Despite the large volume of clinical trials conducted on the topic, few clinical conclusions can be drawn due to the poor quality of these studies. Further high-quality clinical trials are needed to answer fundamental questions in the surgical treatment of ingrown toenails.
Victoria Exley, BSc (Hons ) Podiatry, MSc Applied Health Research, is a research fellow and trial coordinator at the York Trials Unit, Department of Health Sciences, University of York in the United Kingdom.
Katherine Jones is a research fellow in the Warwick Clinical Trials Unit, Warwick Medical School, at the University of Warwick in Coventry, United Kingdom.
Grace O’Carroll, PhD, is a research fellow and trial coordinator at the York Trials Unit, Department of Health Sciences, University of York in the United Kingdom.
Judith Watson, PhD, is a reader and deputy director of the York Trials Unit, Department of Health Sciences, University of York in the United Kingdom.
Michael Backhouse, PhD, is associate professor in the Warwick Clinical Trials Unit, Warwick Medical School, at the University of Warwick in Coventry, United Kingdom.

This article has been excerpted from “A systematic review and meta-analysis of randomised controlled trials of surgical treatments for ingrown toenails part II: healing time, post-operative complications, pain, and participant satisfaction.” J Foot Ankle Res. 2023 Sep 6;16(1):55. doi: 10.1186/s13047-023-00655-7. PMID: 37674170; PMCID: PMC10481456. Editing has occurred, including the renumbering or removal of tables, and references have been removed for brevity. Use is per CC Attribution 4.0 International License.





