
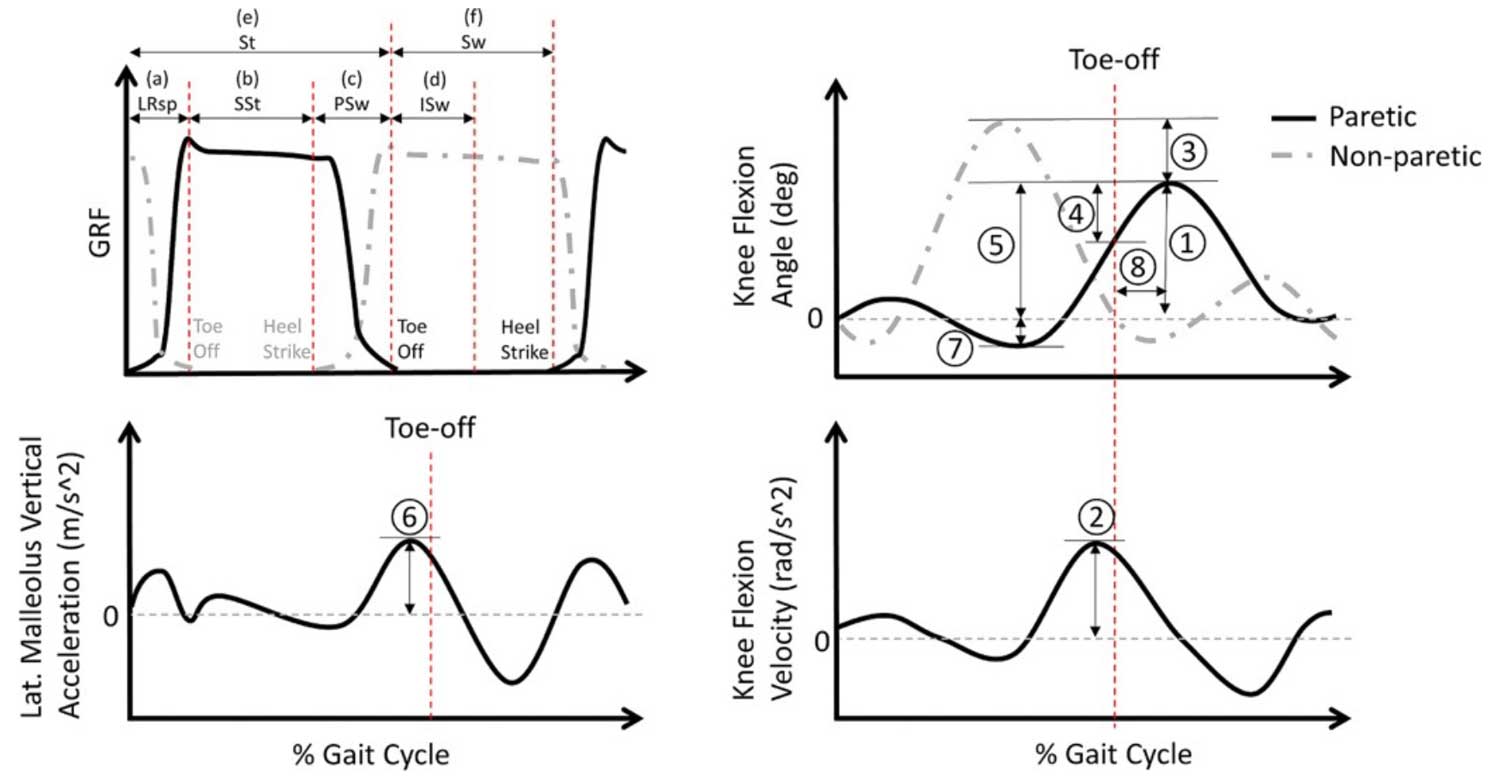
Figure. Gait phases and features associated with post-stroke SKGs. Gait phases (top left) are divided into a) Loading response (LRsp), b) Single-limb support stance (SSt), c) Pre-swing (PSw), d) Initial Swing–50 % of swing, (ISw), e) Stance (St), and f) Swing (Sw). Gait features from paretic side relevant to post-stroke SKG are 1) peak knee flexion in swing, 2) peak knee flexion velocity in pre-swing, 3) between-limb difference of peak knee flexion in swing), 4) knee range of motion in initial swing, 5) knee range of motion in full cycle, 6) peak push off acceleration in pre-swing, 7) timing of peak knee flexion in swing, and 8) peak knee extension in stance.
Stiff-knee gait (SKG) affects 25–75% of individuals with post-stroke gait impairment and is typically defined as reduced swing phase knee flexion. Different studies use various measures to identify stiff-knee gait, such as peak swing knee flexion angle, timing of peak knee flexion, knee range of motion, and ankle push-off acceleration, leading to inconsistent results. The goal of this study was to determine the best single parameter biomechanical definition of post-stroke SKG. We conducted a univariate analysis approach to examine the independence, consistency, validity, and accuracy of the most common biomechanical metrics of SKG based on clinical judgement at 2 different gait speeds. Researchers then created threshold values of the best performing parameters for suggested clinical diagnosis.
This study used univariate cluster analysis to examine the independence, consistency, validity, and accuracy of different definitions in 50 post-stroke individuals (24 with and 26 without stiff-knee gait), as determined by a physiatrist. Spearman’s rank correlation was used for correlation analysis, and 5 clustering techniques along with clinician evaluations were used for validity analysis.
Correlation analysis showed that peak knee flexion timing and knee hyperextension are poorly correlated with reduced swing-phase knee flexion angle (P = –0.09 and P = –0.26 respectively). Validity analysis indicated that the between-limb difference in peak swing knee flexion angle and peak swing knee flexion angle at self-selected gait speeds were the most valid differentiators. At the fastest comfortable gait speed, the between-limb difference of peak knee flexion angle had the highest sensitivity, lowest specificity, and highest F1 scores.
We determined thresholds of less than 44.3° for peak swing knee flexion angle and greater than 17.0° for the between-limb difference of peak knee flexion angle identify stiff-knee gait during self-selected walking. We recommend using the difference in peak swing knee flexion angle between limbs to diagnose post-stroke stiff-knee gait due to its robustness to changes in gait speed.
Source: Lee J, Lee RK, Seamon BA, Kautz SA, Neptune RR, Sulzer J. Between-limb difference in peak knee flexion angle can identify persons post-stroke with Stiff-Knee gait. Clin Biomech (Bristol). 2024;120:106351. doi: 10.1016/j. Use is per CC BY





