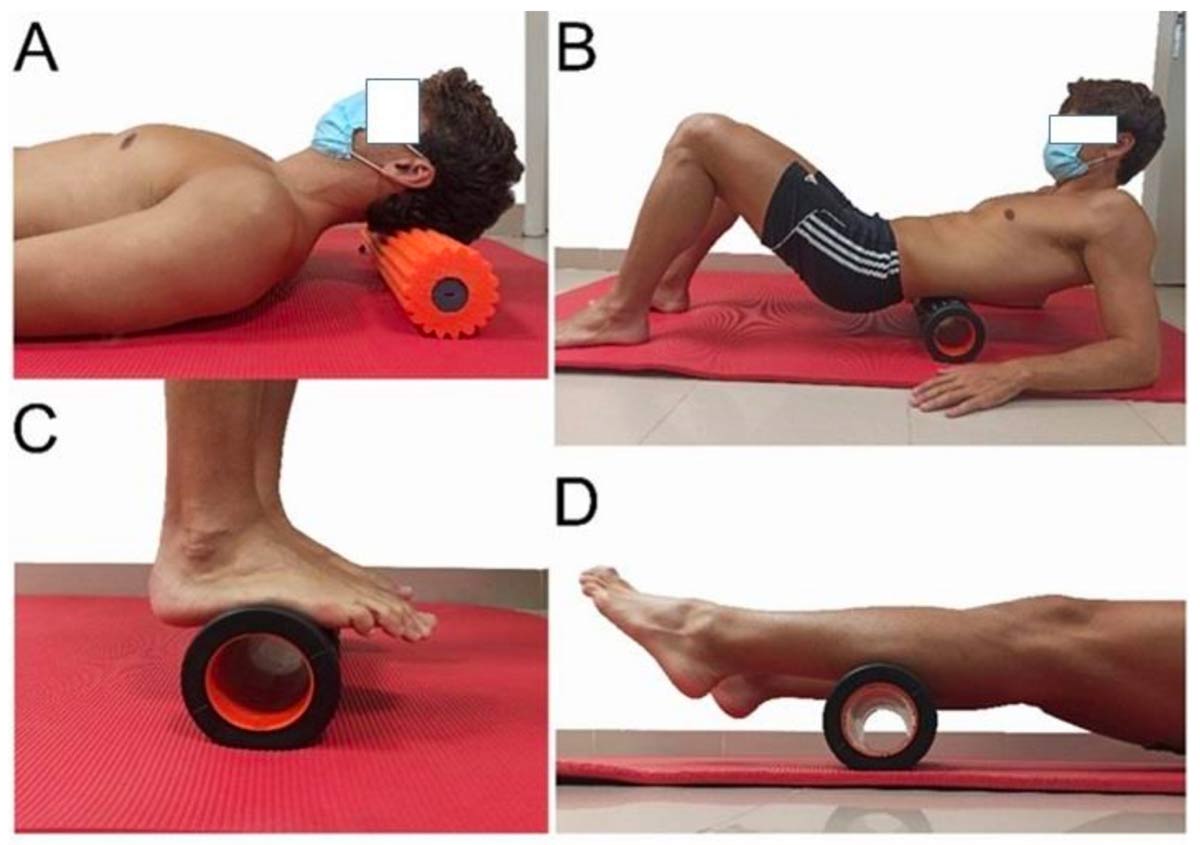
Figure. Interventions. (A) intervention to the epicranial aponeurosis, (B) thoracolumbar facia and erector muscles intervention, (C) plantar fascia and (D) posterior part of the sural fascia.
Classic anatomy textbooks describe the hamstring muscles from a traditional mechanistic view as being isolated from the adjacent structures. However, recent research has changed this perspective, proposing a connective tissue link between the active components of the movement system to form an extensive network of myofascial chains, or meridians. Of these meridians, there is most anatomical evidence for the superficial back line (SBL). This myofascial chain connects the hamstring muscles with the gastrocnemius muscles and the plantar fascia caudally, and with the thoracolumbar fasciae, the erector spinae muscle, and the epicranial aponeurosis cranially.
Functionally, anatomical studies have demonstrated the role of these fascia in the transmission of biomechanical force between the different regions of the body connected by the chains. The hamstring muscles are described as forming part of myofascial chains or meridians, and the superficial back line (SBL) is one such chain. Good hamstring flexibility is fundamental to sporting performance and is associated with prevention of injuries of these muscles.
The aim of this study was to measure the effect of self-myofascial release (SMR) on hamstring flexibility and determine which segment of the SBL resulted in the greatest increase in flexibility.
Methods: 94 volunteers were randomly assigned to a control group or to 1 of the 5 intervention groups. In the intervention groups, SMR was applied to 1 of the 5 segments of the SBL (plantar fascia, posterior part of the sural fascia, posterior part of the crural fascia, lumbar fascia, or epicranial aponeurosis) for 10 min. The analyzed variables were hamstring flexibility at 30 s, 2, 5, and 10 min, and dorsiflexion range of motion before and after the intervention.
Results: Hamstring flexibility and ankle dorsiflexion improved when SMR was performed on any of the SBL segments. The segments with the greatest effect were the posterior part of the sural fascia when the intervention was brief (30 s to 2 min) or the posterior part of the crural fascia when the intervention was longer (5 or 10 min). In general, 50% of the flexibility gain was obtained during the first 2 min of SMR.
Discussion: This study found that performing SMR on any segment of the SBL resulted in a statistically significant increase in hamstring flexibility and ankle dorsiflexion. These results reinforce the concept of the chain as an entity, not just from an anatomic perspective, as has been described previously, but also as a functional structure as reported in recent studies. The segment found to affect hamstring flexibility most was the plantar fascia. The effects were greater especially when the foam roller was applied for relatively short times.
This implication is not new, and the results are similar to those observed when self-massage of the plantar fascia with a ball was performed for 5 min, or to the results with self-massage for 5 min. Comparable results to ours were obtained when treatment was applied by a therapist over various sessions; they also found better results when the SMR was self-applied. Our results show that when the foam roller was applied for longer periods of time (from 5 to 10 min), the segments of the thoracolumbar fasciae and erector muscles, and the posterior part of the sural fascia had more impact on hamstring flexibility. Previous studies observed an improvement in dorsiflexion but did not assess hamstring flexibility. Other investigations also found increased ankle dorsiflexion following self-massage of the posterior part of the lower limb, but did not establish which fascial segment had the greatest effect.
The effects of SMR to each of these segments on hamstring flexibility may be due to the continuity, overlapping and compartmentalization of the muscular tissue by the fascia. A possible explanation for the better results when SMR was performed on the plantar fascia is the significant fascial continuity, via the Achilles tendon, between the plantar fascia and the posterior part of the sural fascia. In the same way, SMR application to the thoracolumbar fascia and erector muscles can be explained by the anatomical connection between the thoracolumbar fascia and the hamstring muscles via the sacrotuberous ligament. Other studies have found significant improvements by combining the foam roll with passive movements. However, it appears that the use of other therapies such as focal vibration may generate superior improvements. Despite these results, the selling price of focal vibration is much higher than that of foam roll. For this reason, it could be interesting to use therapies such as focal vibration within a therapeutic treatment with the physical therapist and the use of the foam roll as a self-treatment for the patient.
Regarding the results obtained, there is a fascial structural relationship in the entire posterior chain. However, there is also a neurophysiological explanation: different manual techniques can generate viscoelastic and hypoalgesic effects through a model based on the fact that a mechanical stimulus initiates a chain of spinal, peripheral, and/or supraspinal neurophysiological events that would produce these changes at a distance even in distant areas such as the suboccipital region.
In summary, the present study demonstrates that the SBL can be considered a functional structure, since SMR application to any of its component segments improved hamstring flexibility and ankle dorsiflexion, the segments with the greatest effects being the plantar fascia (for short treatment duration) and the thoracolumbar fascia and erector muscles (for longer treatment duration). The results suggest that this technique could be effective both in rehabilitation and sports to enhance hamstring flexibility remotely.
In conclusion, the present study demonstrates that the SBL can be considered a functional structure, as the application of SMR on any of its component segments improved hamstring flexibility and ankle dorsiflexion. The use of this treatment could be effective in both rehabilitation and sport to improve hamstring flexibility at a distance.
Source: Fauris P, López-de-Celis C, Canet-Vintró M, et al. Does self-myofascial release cause a remote hamstring stretching effect based on myofascial chains? A randomized controlled trial. Int J Environ Res Public Health. 2021 Nov 24;18(23):12356. Use is per Creative Commons CC BY.





