
 Studies of the kinematic variables associated with medial tibial stress syndrome suggest possible targets for prevention and intervention, including the use of foot orthoses.
Studies of the kinematic variables associated with medial tibial stress syndrome suggest possible targets for prevention and intervention, including the use of foot orthoses.
By Janice K. Loudon, PT, PhD, SCS, ATC, and Michael P. Reiman, PT, DPT, OCS, SCS, ATC, FAAOMPT, CSCS
Various overuse musculoskeletal injuries, including shin pain, can hamper participation in a running exercise program.1-3 A number of terms have been introduced in the literature to describe medial shin pain, and medial tibial stress syndrome (MTSS) is one of the most descriptive terms.4 MTSS describes a specific overuse injury that produces pain along the posteromedial aspect of the distal two-thirds of the tibia.5 It excludes other types of exercise-related leg pain, such as tendinopathy, stress fracture, and exertional compartment syndrome.6-9
Researchers have reported a range of the incidence of MTSS in high school cross-country runners from 10.7% to 16.8%.1,10,11 Clement et al11 found incidence was higher in female runners (16.8%) than in male runners (10.7%). The sports in which athletes are most commonly afflicted are cross country, track, basketball, and volleyball.3 In the military, the incidence has been reported to be as high as 35%, and, again, higher in women than in men.5,12
 The pathogenesis of MTSS is controversial, with some authors describing the condition as a periostitis (inflammation of the periosteum) due to strain of the medial tibial fascia, while others describe it as a tearing of the muscle-bone interface.2,4,13 Bouche and Johnson found that in fresh cadaver limbs contraction of the superficial and deep posterior compartment muscles creates a traction force in the distal tibia fascia.13 Muscles identified as possible culprits include the posterior tibialis,14,15 soleus,16,17 and flexor digitorum longus.16
The pathogenesis of MTSS is controversial, with some authors describing the condition as a periostitis (inflammation of the periosteum) due to strain of the medial tibial fascia, while others describe it as a tearing of the muscle-bone interface.2,4,13 Bouche and Johnson found that in fresh cadaver limbs contraction of the superficial and deep posterior compartment muscles creates a traction force in the distal tibia fascia.13 Muscles identified as possible culprits include the posterior tibialis,14,15 soleus,16,17 and flexor digitorum longus.16
Tweed et al18 proposed that MTSS “is not an inflammatory process of the periosteum but instead a stress reaction of the bone that has become painful.” Further evidence that MTSS involves changes in the bone was revealed by Magnusson et al,19 who found that male soccer players with MTSS had lower bone density than those without the condition. It is possible that MTSS and tibial stress fractures are on a single continuum, but this has yet to be established.16,20
Clinical history and symptoms form the primary diagnostic basis for MTSS. Normal radiographs and compartment pressures decrease the likelihood of MTSS.2,4 Pain and tenderness are usually diffuse and located along the medial distal two-thirds of the tibia. Commonly, athletes will complain of pain at the beginning of a run that may subside midway but recur at the end of the run. Provocative tests to rule in MTSS include pain with passive ankle dorsiflexion, resisted plantar flexion, toe raises, or single-leg hops.18 Recently, Newman et al found that positive pain with shin palpation and the shin edema test were predictive of MTSS development.21
 The etiology of MTSS has been discussed in the literature.1,7,22 Potential contributing factors are diverse, and some are contradictory. They can be divided into three subsets of etiology, including structure/pathomechanics, training error, and body mass. The most widely studied subset is structure/pathomechanics. Examples of all factors include pes cavus,23 pes planus,22,24,25 pronation velocity,26 time to maximum pronation,26 prolonged rearfoot pronation,26 limited ankle motion,7,27 sex,1 bone mineral density,28 menstrual dysfunction,28 previous injury,29,30 and increased impact forces while running.31 Of all these factors, the only ones consistently linked to MTSS are a history of previous injury and high body mass index (BMI).
The etiology of MTSS has been discussed in the literature.1,7,22 Potential contributing factors are diverse, and some are contradictory. They can be divided into three subsets of etiology, including structure/pathomechanics, training error, and body mass. The most widely studied subset is structure/pathomechanics. Examples of all factors include pes cavus,23 pes planus,22,24,25 pronation velocity,26 time to maximum pronation,26 prolonged rearfoot pronation,26 limited ankle motion,7,27 sex,1 bone mineral density,28 menstrual dysfunction,28 previous injury,29,30 and increased impact forces while running.31 Of all these factors, the only ones consistently linked to MTSS are a history of previous injury and high body mass index (BMI).
The literature is scarce regarding preferred evidence-based interventions for MTSS. Basic treatment consists of rest from the offending activity, cross training, and cryotherapy.17 Other recommendations include ankle muscle strengthening and stretching.4,32 Eickhoff et al surveyed cross-country runners who were prescribed foot orthoses and found the devices improved symptoms of MTSS.33 Plisky et al10 reported that runners with MTSS injury were three times as likely to report orthosis use, but the researchers did not mention the effectiveness of the devices.
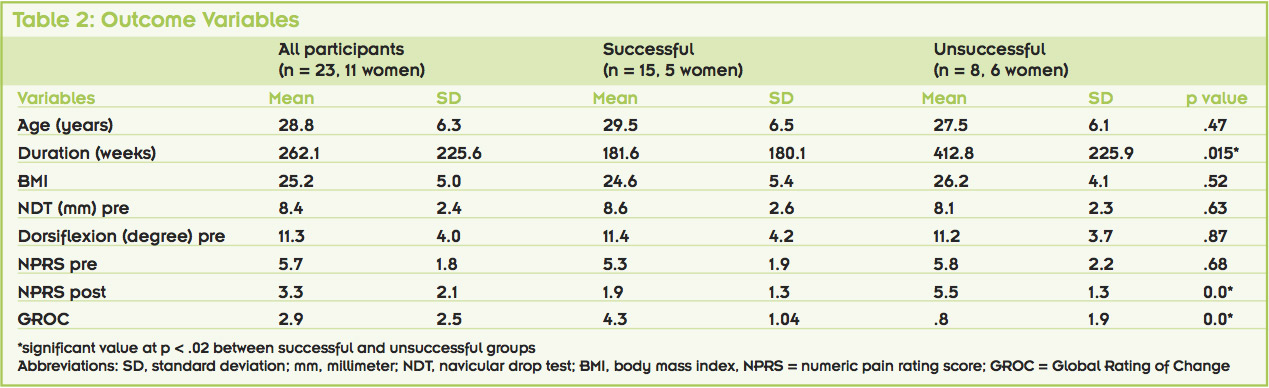
The lead author of this paper has investigated factors related to the foot and ankle and the pelvis and hip in individuals with MTSS. In 2010, Loudon and Dolphino34 published an article investigating the effectiveness of a combination of gastroc-soleus stretching and foot orthoses in diminishing pain in individuals with MTSS. Twenty-three people (11 women) participated in the study, ranging in age from 22 to 44 years (mean = 28.8, SD = 6.3). Participants were runners or walkers who ran or walked at least 10 miles per week and experienced MTSS.
We assessed navicular drop, dorsiflexion range of motion, BMI, duration of symptoms, and pain score on the first visit. All participants were then given a stretching program for the gastroc-soleus and a pair of flexible off-the-shelf orthoses made with an upper layer of Aliplast and a supportive layer of Plastazote with a neutral base.
 After three weeks of the intervention, pain level and the Global Rating of Change (GROC) were obtained for each participant.35 All subjects reported they were compliant with the intervention. We then dichotomized the participants into a successful group (determined as a 50% improvement in pain level) and an unsuccessful group. Fifteen had a successful outcome (65.2%), while eight individuals did not meet the threshold for success (34.8%).
After three weeks of the intervention, pain level and the Global Rating of Change (GROC) were obtained for each participant.35 All subjects reported they were compliant with the intervention. We then dichotomized the participants into a successful group (determined as a 50% improvement in pain level) and an unsuccessful group. Fifteen had a successful outcome (65.2%), while eight individuals did not meet the threshold for success (34.8%).
Table 2 displays the variables of this study. Both postintervention pain level and GROC score were statistically different between groups. The 65.2% success rate in our study was less than the 88% rate that Eickhoff et al33 found in collegiate cross-country runners prescribed off-the-shelf orthoses for MTSS.
The two initial impairment measures, ankle dorsiflexion and navicular drop test, were not different between the two groups. However, these were not measured at the completion of the study, which would have been ideal. The mean duration of symptoms for the participants in our study was 262.1 ± 225.6 weeks. For the successful group, the duration was 181.6 ± 180.1 weeks, which was significantly less than the unsuccessful group (412.8 ± 225.9 weeks). These outcomes would support early intervention, which can make a difference in the success of using orthoses and stretching. Age was not significantly different between groups.
BMI has been identified as a contributing factor to MTSS. Plisky et al10 found that, after adjusting for gender and orthotic use, runners with a higher BMI had an increased risk of MTSS compared with their lower-weight counterparts. The study by Loudon and Dol- phino34 is in agreement with these findings, with the average BMI for both groups equalling 25.2, which meets the World Health Organization defintion for overweight.36 The successful group did have a slightly lower BMI (24.6) than the unsuccessful group (26.2), but this difference was not significantly different.
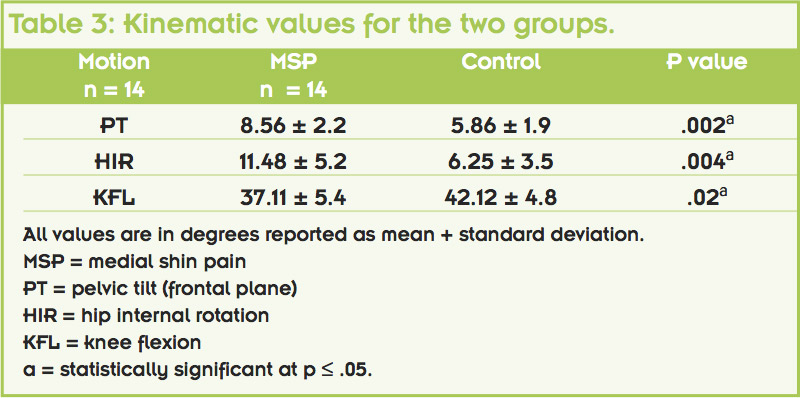
 In a second study, published in 2012, Loudon and Reiman37 investigated differences in pelvic, hip, and knee kinematics during running between two groups: uninjured athletes and those with a history of MTSS. Secondary analyses investigated differences in limbs between groups and differences between female and male athletes.
In a second study, published in 2012, Loudon and Reiman37 investigated differences in pelvic, hip, and knee kinematics during running between two groups: uninjured athletes and those with a history of MTSS. Secondary analyses investigated differences in limbs between groups and differences between female and male athletes.
Fourteen runners with a history of MTSS and 14 controls matched for sex, age, and training mileage took part in the study. We examined 3D kinematics of the pelvis, hip, and knee while the athletes ran on a treadmill at a self-selected speed. Runners with a history of MTSS demonstrated significantly greater frontal plane pelvic tilt (P = .002, effect size = .55) and peak hip internal rotation (P = .004, effect size = .51) and less knee flexion (P = .02, effect size = .46) than the control group (Table 3).
Clinical implications
During running, the lower leg segments should work in sequence. At initial contact the subtalar joint pronates until about midstance, at which time it begins to supinate to ready the limb for push-off. In conjunction with subtalar joint pronation, the tibia and femur rotate internally.38 In addition to pronation, the talocrural joint needs to dorsiflex, which facilitates knee flexion. This mechanism is needed for force absorption from the ground. Interestingly, maximal calcaneal eversion motion (a component of pronation) and maximal knee flexion motion peak at the same time during the midstance phase of running.39
The foot strikes the ground approximately 600 times per kilometer for every running mile. There is evidence that these ground reaction forces are particularly high along the medial and posterior aspects of the tibia.40 This posteromedial force may be exacerbated by limited ankle (talocrural joint) motion and/or limited knee flexion. As presented in the lead author’s studies, a lack of mobility at the ankle, knee, or both is associated with MTSS.34,37 The addition of a full-contact flexible orthosis may help with force distribution and pain symptoms in MTSS. Improving dorsiflexion motion would also help with load distribution.
Kinematically, it has been demonstrated that lack of knee flexion motion during landing from a jump is associated with increased frontal and transverse plane motion.41 In runners, Souza and Powers reported that, compared with control group, women with patellofemoral pain syndrome exhibited significantly greater peak hip internal rotation during running and other functional tasks.42 We saw this same phenomenon again in our running athletes with a history of MTSS. Runners with less peak knee flexion motion had an increase in peak hip internal rotation and frontal plane pelvic drop to the swing side. Increased levels of hip internal rotation have been found previously in runners with tibial stress fractures.43

 Although the runners in the current study did not have tibial stress fracture, MTSS may be a precursor for such fractures, so one might expect to see the same mechanism of injury. Knee flexion is one of the main mechanisms for shock absorption and, when it is lacking, compensations will be seen proximally and distally.
Although the runners in the current study did not have tibial stress fracture, MTSS may be a precursor for such fractures, so one might expect to see the same mechanism of injury. Knee flexion is one of the main mechanisms for shock absorption and, when it is lacking, compensations will be seen proximally and distally.
Clinicians can gain valuable insight by considering the entire lower extremity in a runner with MTSS. Whether the proximal or distal segment is the primary offender has yet to be determined. It is interesting to note that the pathomechanical pattern seen in MTSS is similar to one that is seen in anterior cruciate ligament injury and patellofemoral pain syndrome.44,45 Treatment for these two conditions has also focused on the foot and the hip.46,47
Conclusion
Despite its high prevalence, little is known regarding the kinematic factors associated with MTSS. It is likely a combination of variables that distinguish individuals with MTSS. There is a need to understand the risk factors associated with MTSS so that effective prevention strategies can be developed and implemented. Our research has found both distal and proximal malalignments that may contribute to MTSS. Based on our research we would recommend ankle stretching (gastroc-soleus complex), hip strengthening (gluteus medius, gluteus maximus), improvement in running technique to increase knee flexion at foot contact, and use of a full-contact insert during the pain period of MTSS.
Janice K. Loudon, PT, PhD, SCS, ATC, is an associate professor and Michael P. Reiman, PT, DPT, OCS, SCS, ATC, FAAOMPT, CSCS, is an assistant professor in the Division of Physical Therapy at Duke University Medical Center in Durham, NC.
1. Bennett JE, Reinking MF, Pluemer B, et al. Factors contributing to the development of medial tibial stress syndrome in high school runners. J Orthop Sports Phys Ther 2001;31(9):504-510.
2. Brukner P. Exercise-related lower leg pain: An overview. Med Sci Sports Exerc 2000;32(3 Suppl):S1-S3.
3. Michelson JD, Durant DM, McFarland E. The injury risk associated with pes planus in athletes. Foot Ankle Int 2002;23(7):629-633.
4. Kortebein PM, Kaufman KR, Basford JR, Stuart MJ. Medial tibial stress syndrome. Med Sci Sports Exerc 2000;32(3Suppl):S27-S33.
5. Yates B, White S. The incidence of risk factors in the development of medial tibial stress syndrome among naval recruits. Am J Sports Med 2004;32(3):772-780.
6. Reinking MF. Exercise-related leg pain in female collegiate athletes: the influence of intrinsic and extrinsic factors. Am J Sports Med 2006;34(9):1500-1507.
7. Michael RH, Holder LE. The soleus syndrome. A cause of medial tibial stress (shin splints). Am J Sports Med 1985;13(2):87-94.
8. Mubarak SJ, Gould RN, Lee YF, et al. The medial tibial stress syndrome. A cause of shin splints. Am J Sports Med 1982;10(4):210-205.
9. Viitasalo JT, Kvist M. Some biomechanical aspects of the foot and ankle in athletes with and without shin splints. Am J Sports Med 1983;11(3):125-130.
10. Plisky MS, Rauh MJ, Heiderscheit B, et al. Medial tibial stress syndrome in high school cross-country runners: incidence and risk factors. J Orthop Sports Phys Ther 2007;37(2):40-47.
11. Clement DB, Taunton JE, Smart GW, McNicol KL. A survey of overuse running injuries. Phys Sportsmed 1981;9:47-58.
12. Kaufman KR, Brodine SK, Shagger RA, et al. The effect of foot structure and range of motion on musculoskeletal overuse injuries. Am J Sports Med 1999;27(5):585-593.
13. Bouché RT, Johnson Ch. Medial tibial stress syndrome (tibial fasciitis): a proposed pathomechanical model involving fascial traction. J Am Podiatr Med Assoc 2007;97(1):31-36.
14. D’Ambrosia RD, Zelis RF, Chuinard RG, Wilmore J. Interstitial pressure measurements in the anterior and posterior compartments in athletes with shin splints. Am J Sports Med 1977;5(3):127-131.
15. Saxena A, O’Brien T, Bunce D. Anatomic, dissection of the tibialis posterior muscle and its correlation to medial tibial stress syndrome. J Foot Surg 1990;29(2):105-108.
16. Beck B, Osternig L. Medical tibial stress syndrome: the location of muscles in the leg and relation to symptoms. J Bone Joint Surg Am 1994;76(7):1057-1061.
17. Detmer D. Chronic shin splints: classification and management of medial tibial stress syndrome. Sports Med 1986;3(6):436-446.
18. Tweed JL, Avil SJ, Campbell JA, Barners MR. Etiologic factors in the development of medial tibial stress syndrome. J Am Podiatr Med Assoc 2008;98(2):107-111.
19. Magnusson HI, Westlin NE, Nyqvist F, et al. Abnormally decreased regional bone density in athletes with medial tibial stress syndrome. Am J Sports Med 2001;29(6):712-715.
20. Moen MH, Tol JL, Weir A, et al. Medial tibial stress syndrome: a critical review. Sports Med 2009;39(7):523-546.
21. Newman P, Adams R, Waddington G. Two simple clinical tests for predicting onset of medial tibial stress syndrome: shin palpation test and shin oedema test. Br J Sports Med 2012;46(12):861-864.
22. Delacerda FG. A study of anatomical factors involved in shinsplints. J Orthop Sports Phys Ther 1980;2(2):55-59.
23. Williams DS, McClay IS, Hamill J, Buchanan TS. Lower extremity kinematic and kinetic differences in runners with high and low arches. J Appl Biomech 2001;17(2):153-163.
24. Tiberio D. The effect of excessive subtalar joint pronation on patellofemoral mechanics: a theoretical model. J Orthop Sports Phys Ther 1987;9(4):160-165.
25. Sommer HM, Vallentyne SW. Effect of foot posture on the incidence of medial tibial stress syndrome. Med Sci Sports Exerc 1995;27(6):800-804.
26. Messier SP, Pittala KA. Etiologic factors associated with selected running injuries. Med Sci Sports Exerc 1988;20(5):501-505.
27. Zifchock RA, Davis I, Higginson J, et al. Side-to-side differences in overuse running injury susceptibility: a retrospective study. Hum Mov Sci 2008;27(6):888-902.
28. Lebrun CM. The female athlete triad: What’s a doctor to do? Curr Sports Med Rep 2007;6(6):397-404.
29. Reinking MF. Exercise-related leg pain in female collegiate athletes: The influence of intrinsic and extrinsic factors. Am J Sports Med 2006;34(9):1500-1507.
30. Reinking MF, Austin TM, Hayes AM. Exercise-related leg pain in collegiate cross-country athletes: extrinsic and intrinsic risk factors. J Orthop Sports Phys Ther 2007;37(11):670-678.
31. Davis IS. Gait retraining in runners. Orthopaedic Practice 2005;17:2.
32. Beck BR. Tibial stress injuries. An aetiological review for purposes of guiding management. Sports Med 1998;26(4):265-279.
33. Eickhoff CA, Hossain SA, Slawski DP. Effects of prescribed foot orthoses on medial tibial stress syndrome in collegiate cross-country runners. Clin Kinesiol 2000;54:76-80.
34. Loudon JK, Dolphino MR. Use of foot orthoses and calf stretching for individuals with medial tibial stress syndrome. Foot Ankle Spec 2010;3(1):15-20.
35. Juniper EF, Guyatt GH, Willan A, Griffith LE. Determining a minimal important change in a disease-specific Quality of Life Questionnaire. J Clin Epidemiol 1994;47(1):81-87.
36. Obesity and overweight. Fact Sheet #311. The World Health Organization website. http://www.who.int/mediacentre/factsheets/fs311/en. Updated March 2013. Accessed April 19, 2013.
37. Loudon JK, Reiman MP. Lower extremity kinematics in running athletes with and without a history of medial shin pain. Int J Sports Phys Ther 2012;7(4):356-364.
38. DeLeo AT, Dierks TA, Ferber R, Davis IS. Lower extremity joint coupling during running: a current update. Clin Biomech 2004;19(10):983-991.
39. Dierks TA, Davis I. Discrete and continuous joint coupling relationships in uninjured recreational runners. Clin Biomech 2007;22(5):581-591.
40. Milgrom C, Finestone A, Hamel A, et al. A comparison of bone strain measurements at anatomically relevant sites using gauges versus gauged bone staples. J Biomech 2004;37(6):947-952.
41. Pollard CD, Sigward SM, Powers CM. Limited hip and knee flexion during landing is associated with increased frontal plane knee motion and moments. Clin Biomech 2010;25(2):142-154.
42. Souza RB, Powers CM. Predictors of hip internal rotation during running: an evaluation of hip strength and femoral structure in women with and without patellofemoral pain. Am J Sports Med 2009;37(3):579-587.
43. Milner CE, Hamill J, Davis IS. Distinct hip and rearfoot kinematics in female runners with a history of tibial stress fracture. J Orthop Sports Phys Ther 2010;40(2):59-66.
44. Ford KR, Myer GD, Hewett TE. Valgus knee motion during landing in high school female and male basketball players. Med Sci Sports Exerc 2003;35(10):1745-1750.
45. Powers CM. The influence of altered lower-extremity kinematics on patellofemoral joint dysfunction: a theoretical perspective. J Orthop Sports Phys Ther 2003;33(11):639-646.
46. Sutlive TG, Mitchell SD, Maxfield SN, et al. Identification of individuals with patellofemoral pain whose symptoms improved after a combined program of foot orthosis use and modified activity: a preliminary investigation. Phys Ther 2004; 84(1):49-60.
47. Powers CM. The influence of abnormal hip mechanics on knee injury: a biomechanical perspective. J Orthop Sports Phys Ther 2010;40(2):42-51.






I might agree with “Tweed et al18 proposed that MTSS “is not an inflammatory process of the periosteum but instead a stress reaction of the bone that has become painful” but I have had many early MTSS athletes with MRIs revealing early periosteal involvement.
BMI may have a secondary role as it increase ground reaction forces but it sure is not a primary role. I see far too many distance runners with low BMI and MTSS to believe BMI is a primary factor. Repetitive ground reaction forces in the distance runner is a multiplier that makes up for low BMI. I find that football players in the first month to 6 weeks of training show up in droves with MTSS. Virtually all the athletes I have treated (considerable over the last 25 year period servicing major university athletic program as well as a private practice with a large athletic population) with posterior tibial stress reactions and stress fractures all report a common history of classical MTSS that begins with a painful area about 2″ in length. As it progress to a stress reaction/fracture that painful area narrows considerably to just directly at the point where the reaction/fracture is involved. This area is at most 3/8″ long, often is swollen and is extremely pain to palpation.
I cannot imagine using any foot orthoses with plastazote and a neutral base on MTSS athletes. Plastazote has a life expectancy of about 2 weeks in any athlete. My experience is that the common denominator in all MTSS, stress reactions/fractures is that they all are pronators. Using a neutral base orthotic on a pronator does not correct for any pronation. Combined with a Plastazote “supportive layer” and I can see why the authors improvement rate was only 50%. I would suggest custom orthotics with better materials management: 275# football players destroy plastazote in a matter of days and a 140# distance runner will compress it in a few weeks. One has to adjust materials for the level of activity, size of the athlete and shoe limitations. I stress biomechanical correct first and add shock absorption if the shoe allows it. Obviously soccer shoes would not accommodate an extra layer of polyurethane like a training shoe.