
Shutterstock.com #1349223794
Foot drop, a complex condition that can have a significant impact on independent ambulation, can have many causes. Treatment options vary by cause. These authors provide a review of the condition from etiology through treatment.
By Subhadra L. Nori, MD, and Michael F. Stretanski, DO
Foot drop (also known as steppage gait) is an inability to lift the forefoot due to the weakness of dorsiflexors of the foot. This, in turn, can lead to an unsafe antalgic gait, potentially resulting in falls.
The etiologies behind this presentation are varied and include muscular, neurologic, spinal, autoimmune and musculoskeletal disorders. Depending on the etiology, treatment options differ.
A thorough understanding of the underlying pathophysiology is necessary before designing a treatment plan. This article will review the etiology, clinical features, diagnosis, and treatment.
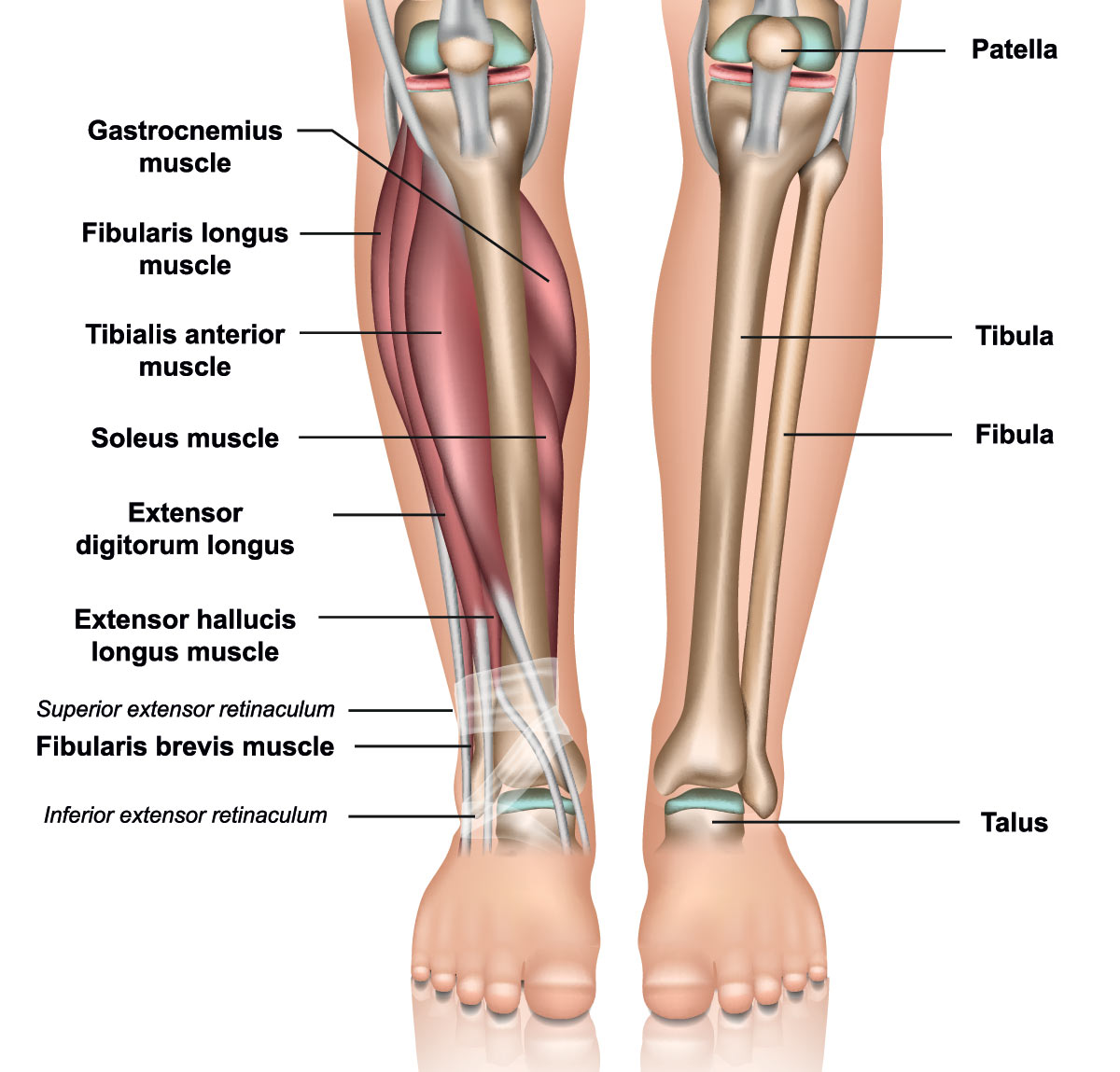
Anatomy
Lumbar nerve roots
There are 5 lumbar vertebrae. The lumbar nerve roots emerge from the lateral spinal recess formed by the inferior facet of the rostral vertebrae and the superior facet of the caudal vertebra. The L5 nerve root exits between the L5 and S1 vertebrae.
Lumbar plexus
The lumbar plexus is composed of the anterior rami of spinal nerves L1-L4. Multiple nerves emerge from this plexus. The iliohypogastric and ilioinguinal nerves supply the transverse abdominis and internal oblique muscles. The obturator nerve supplies the adductors of the thigh. The femoral nerve is a large nerve that supplies the quadriceps femoris group and continues as the saphenous nerve which is the sensory nerve to the medial leg.
Sciatic nerve
The sciatic nerve is the largest branch of the lumbosacral plexus and consists of nerve roots L4 to S4. It travels in the posterior thigh to the popliteal fossa. Here it divides into 2 branches: the tibial and the common fibular (historically peroneal) nerves. The tibial innervates hamstrings, plantar flexors, and invertors of the foot.
Common fibular nerve
The common fibular nerve is the lateral terminal branch of the sciactic and runs laterally across the lateral head of the gastrocnemius muscle. It then continues around the fibular head where it is subcutaneous and so is vulnerable to compression. As it passes between the fibula and fibularis longus muscle it divides into the deep and superficial fibular nerves. The deep fibular nerve innervates ankle and toe-extensors and supplies sensation to a small area at the first web space between the first and second toes. The superficial fibular nerve supplies the main evertors of the foot, the fibularis longus, and brevis muscles. The superficial fibular sensory branch supplies sensation to the dorsum of the foot and lateral calf.
Etiology
Pearls and Other Issues
- Foot drop is an inability to lift the forefoot due to the weakness of the dorsiflexors.
- This may be a result of muscular-skeletal or nervous system pathology.
- A thorough evaluation should include medical history, physical examination and necessary imaging, and or electrodiagnostic studies.
- Depending upon the etiology, either surgical or non-surgical options are exercised.
- Prognosis depends upon the extent of nerve damage and the viability of the remaining muscles.
- A comprehensive approach, including referrals to appropriate services, will result in a better outcome.
- Careful analysis of the presenting history and physical examination is essential to arrive at the proper diagnosis.
- Management is contingent upon diagnosis and severity.
Compressive Disorders
Entrapment syndromes of the fibular nerve at various locations along its anatomical pathway can lead to compressive neuropathy. Of these, common fibular neuropathy at the fibular head is the most common mononeuropathy affecting the leg. The fibular nerve is quite superficial near the head of the fibula, making it vulnerable to pressure palsies. Anatomic variations of the biceps femoris muscle, between the gastrocnemius and distal biceps, can contribute to the formation of a tunnel that can predispose to compression of the nerve. Other contributing factors include weight loss, prolonged bedridden status, tight casts, space-occupying lesions, and bone metastasis involving the fibular head.
Sciatic nerve compression between the two heads of the piriformis muscle leading to foot drop has been reported.
Compression palsies in the ICUs due to protracted bed rest, have been known to occur. Approximately 10% of patients that stay in the ICU for a period longer than 4 weeks are expected to develop paresis of the fibular nerve. Critical illness polyneuropathy involving multiple motor and sensory nerves can also present with foot drop. Depending on the extent of involvement, weakness can be bilateral. Patients with diabetes are more vulnerable to these compression neuropathies.
Lumbar radiculopathy is also a common cause of foot drop. L5 radiculopathy is the most common lumbar radiculopathy and typically results from lumbar disc herniation or spondylitis in the spine.
Extraforaminal compression of the L5 nerve from disc herniations and bony (osteophytes or sacral ala) or ligamentous (sacroiliac ligament and lumbosacral band) compression is known to occur. Bone metastasis at the fibular head, although uncommon, can cause foot drop.

Traumatic Injuries
Traumatic injuries often occur in association with orthopedic injuries as knee dislocations, fractures, blunt trauma, and musculoskeletal injuries. Sciatic neuropathy most commonly results from a traumatic injury of the hip or secondary to surgery. Sciatic neuropathy is the second most common mononeuropathy of the lower extremity and typically presents with foot drop.
A less common cause is lumbosacral plexopathies, which can result from traumatic injury, a complication of abdominal or pelvic surgery, or a complication of neoplasm or radiation therapy.
Neurologic Disorders
ALS (Amyotrophic lateral sclerosis), also known as motor neuron disease (MND) or Lou Gehrig disease, is a neurodegenerative disease manifested by the death of motor neurons in the anterior horn cells leading to muscle weakness, difficulty speaking and swallowing. Initial presentation can be a painless foot drop.
Cerebrovascular disease (CVA) can present as hemiplegia. Foot drop is a part of this presentation. Other signs of upper motor neuron involvement as increased muscle tone, hyperreflexia, and circumduction of the lower extremity during ambulation are also seen. Depending on the location of ischemia, aphasia can be present.
Mononeuritis multiplex is defined as the involvement of one or more sensory and peripheral motor nerves. It is usually painful and asymmetrical. It can be associated with AIDS, leprosy, hepatitis, granulomatis with polyangiitis (Wegener granulomatosis), and rheumatoid arthritis. Loss of sensation and movement may be associated with dysfunction of specific nerves. The sciatic nerve is one of the commonly affected nerves in this condition. Vasculitis of small epineuria arteries leads to damage to the axons causing disruption in nerve conduction and eventually leading to muscle weakness.
Acute inflammatory demyelinating polyneuropathy (AIDP), also called Guillain-Barré syndrome, is an autoimmune process in which progressive motor weakness, sensory loss, and areflexia is a characteristic presentation. Sensory symptoms often precede motor weakness. Autonomic dysfunction is a common accompaniment to this condition. Damage to the myelin sheath leads to segmental demyelination. A hallmark of AIDP is the slowing of nerve conduction velocities and conduction block. Foot drop can be part of the clinical presentation.
Charcot–Marie Tooth (CMT) is a primary congenital demyelinating peripheral neuropathy and is one of the most common inherited neuropathies. It affects both motor and sensory nerves. The incidence is 1 in 25,000. One of the main symptoms is foot drop along with wasting of the lower leg muscles, giving a typical “stork leg” appearance.
Somatization disorder and conversion reaction are not uncommon etiologies to foot drop. In the event of an otherwise unremarkable workup, psychiatric evaluation should be considered. It should be noted that both the needle EMG and nerve conduction portions of the electrodiagnostic medicine study will appear normal in cases of poor or no effort for ankle dorsiflexion or other motor groups.
History and Physical
A careful history and physical exam can help identify the likely cause of foot drop.
Standard musculoskeletal testing asking the patient to toe stand, heel stand, and do a deep knee bend should be observed. MRC scale rating 0-5 for the major muscle groups to the lower extremities, including ankle plantarflexion, ankle dorsiflexion, ankle inversion, ankle eversion, knee extension, knee flexion, and hip flexion should be performed and graded. Neurosensory exam for pinprick should be performed in the distribution looking for both peripheral nerves, as well as lumbar dermatomes. Muscle mass with the side to side comparison observing the major muscle group bulk areas can be done well doing manual motor testing, and side-to-side circumference measurements can be made and documented to note progression, or recovery of mass further down the road. The ASIA (American Spinal Cord Injury Association) point and motor groups are a standardization convenient for communication between professionals; however, it does not include evaluation of specific peripheral sensory nerves.
A formal electrodiagnostic medicine consult, including EMG and nerve conduction studies, is considered to be an extension of the physical examination and may need to be obtained from the subspecialist who is not commonly the first clinician to be involved in the care of the patient.
Any damage affecting the neuraxis from the roots to the peripheral nerve can lead to weakness of the muscles supplied by that nerve.
A lesion of the L5 root, lumbar plexus, sciatic nerve, common peroneal, or the deep peroneal nerve can potentially lead to foot drop due to the weakness of the anterior compartment musculature. The presenting symptom is the inability to ambulate as before. More specifically, weakness of the muscles in the foot that assist in dorsiflexion. There may or may not be a pain. The person will be unable to dorsiflex during the heel strike. The foot remains flat on the ground. Sometimes can also cause toe drag and inability to clear the foot. This can potentially lead to falls.
Radiculopathy affecting the fifth lumbar nerve root typically results in neuropathic pain starting in the lumbar region and radiating down the posterior thigh, anterolateral leg to the foot down to the big toe. Sensory symptoms include the medial aspect of the foot, including the first webspace. Motor symptoms include weakness of dorsiflexors and evertors of the foot.
The Following is an Example of the Care Coordination Plan
- A thorough history and physical examination
- Assessment of risk factors
- Consultation with neurology and PMR
- Order diagnostic imaging, EMG
- Provision of pain management
- Provision of the brace as needed with orthotist
- Referrals to PT and OT
- Potential surgical consultation and or intervention
- Review of skincare, fall prevention
- Follow up appointments as needed
Lumbosacral plexopathies can present with similar sensory and motor deficits that are similar to sciatic neuropathy. Weakness may also affect hip girdle muscles, including hip abduction (gluteus medius) and hip extension (gluteus maximus).
Sciatic neuropathy classically presents with sensory loss of the whole foot and weakness of ankle plantar flexors (gastrocnemius, soleus) as well as ankle inversion, and can result in a ‘flail foot.’ Hamstring muscles may also be involved resulting in knee flexion weakness. It is not uncommon for an incomplete sciatic neuropathy to present as a common peroneal neuropathy, as many times the peroneal fascicles in the sciatic nerve are more susceptible to injury than are the tibial fascicles.
In common fibular neuropathy, the patient presents with sensory and motor deficits. History may include leg crossing, prolonged kneeling, immobility, or trauma. Sensory loss or paresthesias affect the lateral leg below the knee and the anterolateral foot. Muscle weakness affects both ankle dorsiflexion (tibialis anterior), toe extension (eg, extensor hallucis longus), and ankle evertors (peroneus longus and brevis).
If only the deep fibular portion is affected, only minimal sensory deficits (limited to the web space between the first two digits) and isolated weakness of toe and ankle extensors are seen. Ankle eversion and inversion are normal.
Isolated superficial fibular neuropathy is rare and presents as the sensory deficit of the foot except for the first webspace. Only ankle eversion/inversion may be affected.
60% of the normal gait cycle consists of the stance phase and 40% of the swing phase. When one foot is in the swing phase, the other is in the stance phase. The gait cycle starts with a heel strike and ends with a heel strike on the same side. During the stance phase, the foot remains flat on the ground. In the heel strike, the foot is in dorsiflexion, preparing for gradual lowering before the stance phase. In the absence of dorsiflexors, the foot remains in plantar flexion during the stance phase. This prevents the ability to clear the ground and prepare for the next phase of the gait cycle. The patient either drags their toes or lifts the foot high to clear the ground.
Evaluation
After a careful physical exam, diagnostic testing should include plain radiographs of the pelvis and tibia and fibula to rule out fracture or dislocation. MRI may be indicated in suspected plexopathies, due to masses, or tumors. MRI of the lumbar spine, knee, and or ankle may be indicated for potential soft tissue masses in cases of compressive neuropathies. MSK ultrasound is also utilized for evidence of swelling at or proximal to the site of compression.
In many cases, an electrodiagnostic study is an important test to confirm the clinical diagnosis or provide an alternate localization and diagnosis. This study can also define the injury severity and provide information regarding prognosis. This study contains two parts: nerve conduction studies and needle electromyography. (EMG).
Treatment / Management
The approach to a patient depends upon the etiology of foot drop and the nature of the compressive lesion. Based on the evaluation and diagnostic findings, many options exist.
Surgical Options
In trauma cases, for nerve transection, nerve reconstruction should take place within 72 hours of injury. Primary nerve repair techniques, autologous nerve graft are usually performed.
For complete nerve compression, necrolysis and nerve decompression should be performed. Return to function has been reported in about 97%. A surgical release may be necessary for patients with equinus deformity.
In cases of significant nerve dysfunction, nerve or tendon transfers may be required. A detailed discussion of surgical options is beyond the scope of this article.
For the other etiologies, treatment is initially conservative because there may be a chance of partial or complete resolution of symptoms spontaneously overtime.
Conservative Management
This includes physical therapy and or splinting and pharmacological therapy to manage pain. The goals of conservative management are to stabilize the gait, and to prevent falls and contractures. Physical therapy focuses on stretching and strengthening muscles. Electrical stimulation techniques of the weakened dorsiflexors have shown promise. A home exercise program should be an integral part of therapy – specifically to maintain strength and range of motion of muscle groups that are working in the prevention of flexion contracture.
Splinting is utilized to minimize contractures. For complete nerve palsies with insufficient recovery, an ankle-foot orthosis (AFO) to prevent further plantarflexion should be ordered. Sufficient education and training should be included to assist in proper usage and maintenance of the brace.
For patients with numbness, instructions for skincare to prevent abrasions and ulcerations are a significant part of management and are often coordinated with the orthotist fabricating the AFO.
For pain management, topical analgesics, serotonin reuptake inhibitors, membrane stabilizers, and opioids can be used. But are not likely to result in clinical recovery.
Follow up electrodiagnostic studies to reassess the situation, looking for reinnervation should also be part of the treatment planning.
Treatment Planning
Early range of motion and potential strengthening should be planned. The electrodiagnostic study may assist in helping plan as to whether or not the patient will be needed for long-term bracing and or whether or not the weakness is likely to get worse or spread to other motor groups. Early placement into the ankle dorsiflexor brace improves gait mechanics, decreases falls, and helps to minimize other secondary musculoskeletal complaints from the altered gait cycle.
Preparation for long-term care, as to bracing, and adaptive equipment should be considered. Rehabilitation medicine services and other therapy should be directed toward the underlying etiology in addition to the foot drop itself. Staging will depend upon the underlying diagnosis such as multiple sclerosis or Lou Gehrig disease being treated differently in terms of staging compared to lumbar spinal pathology.
Complications can be a result of nerve damage itself or a consequence of gait aids and braces.
Nerve damage leading to foot drop impairs the ability to clear the ground resulting in a fall. Gait aids as walkers and canes can also be an impediment, especially on uneven surfaces. Anesthetic skin can be a source of ulceration. Abrasions can be a result of poor fitting braces. Bracing may need to be variable depending upon bulk change. In cases such as renal failure and congestive heart failure, different braces for different phases of edema and swelling may need to be provided.
As outlined above, physical therapy, occupational therapy can play a major role in whether the patient had conservative or surgical management.
Subhadra L. Nori, MD, is a physiatrist and associate professor in rehabilitation medicine at the Icahn School of Medicine in the Mount Sinai Health System in New York City, New York. Michael F. Stretanski, DO, specializes in pain management and physical medicine/rehabilitation at Interventional Spine & Pain Rehabilitation Center in Mansfield, Ohio.
This article is excerpted from “StatPearls: Foot Drop,” by the same authors which appears in the Bookshelf of the National Center for Biotechnology Information available at https://www.ncbi.nlm.nih.gov/books/NBK554393/. Its use is per the Creative Commons License 4.0; editing has occurred, and references have been deleted for length considerations.






I’ve had foot drop in both legs for 25 plus years and no one has been able to sell me the reason why. It started on the left side when I turned 63 and three years later the right foot began to drop. Is this typical to have both feet affected? or does this give some sort of clue as to the cause. If I knew the cause I might be able to deal with it other than wearing braces,great article!
“different braces for different phases of edema and swelling may need to be provided” Not a chance of this ever being possible for many financial and practical reasons. Why not consider and conventional single or double upright AFO with extra depth shoes? Also, another crucial issue with the authors assessment of foot drop is the comment “In the heel strike, the foot is in dorsiflexion”. The foot/ankle in not in dorsiflexion during swing phase, it is at 90 degrees. The ankle is only in dorsiflexion in late stance phase. When we see a person with “toe drag” in swing but also observe that the ankle is reaching it’s normal amount of dorsiflexion then we need to look higher up. Inadequate knee flexion is usually the cause. If this is the case, any choice of AFO will result in a disappointing outcome. It is always interesting to know the etiology of foot drop, but it rarely changes the decision making of whether a patient will benefit from an orthosis, or what type of orthosis is most suitable. Careful observation and patient assessment work best.