
By James McGuire, DPM, LPT, LPed, FAPWHc
“Variability is the law of life, and as no two faces are the same, so no two bodies are alike, and no two individuals react alike and behave alike under the abnormal conditions we know as disease.”
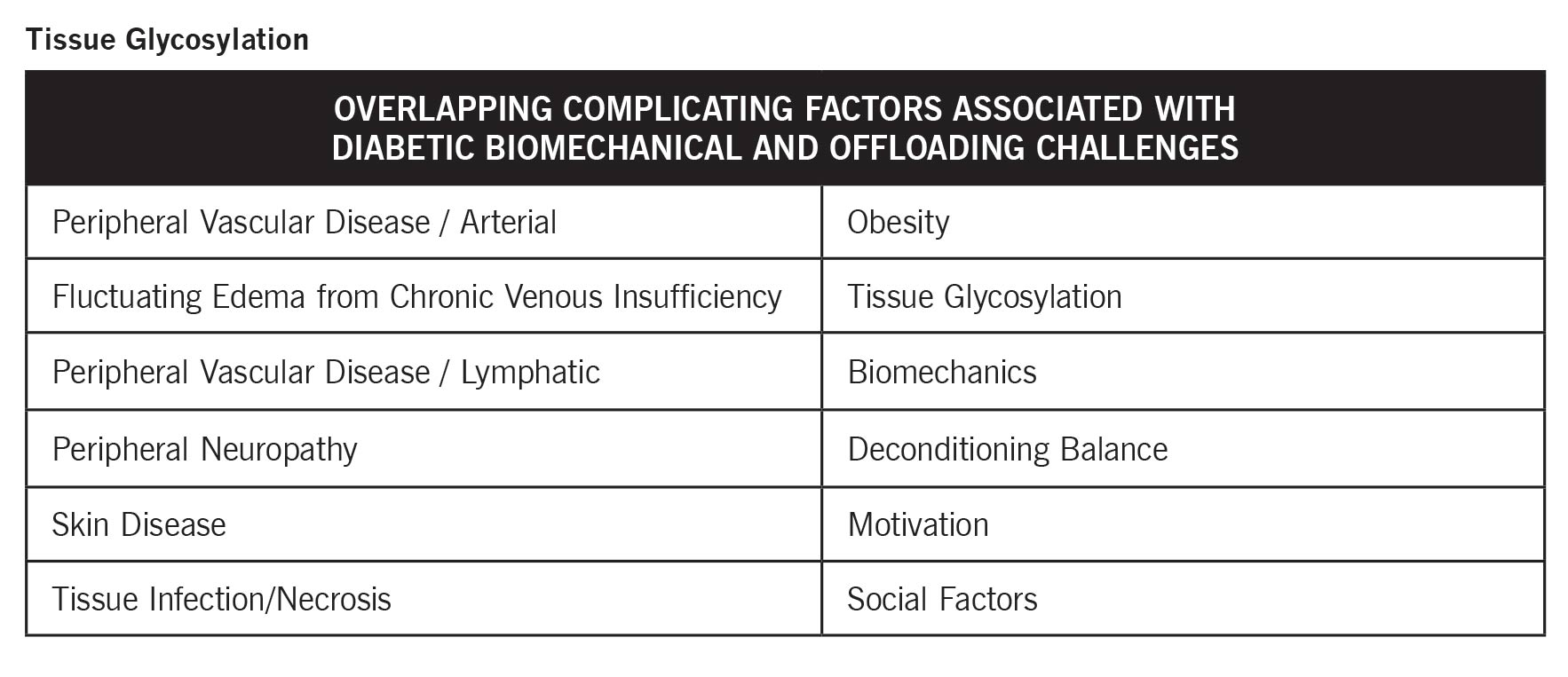
 The biomechanics of the diabetic foot are an intricate interplay of physiological and mechanical challenges that necessitate specialized care strategies. Diabetes often triggers changes in foot structure and function as a result of complications including peripheral neuropathy, vascular issues, and obesity. Additionally, tissue glycosylation adds rigidity to muscles and joints, exacerbating biomechanical imbalances. These changes lead to increased plantar pressure, impaired balance, and heightened ulceration risk, especially in areas such as the metatarsal heads. The underpinning forces of gravity further contribute to alignment difficulties, pushing the foot toward a more stable, yet problematic, plantar grade position. Understanding and addressing these biomechanical challenges are crucial for effective diabetic foot care, aiming to mitigate risks and enhance patient outcomes.
The biomechanics of the diabetic foot are an intricate interplay of physiological and mechanical challenges that necessitate specialized care strategies. Diabetes often triggers changes in foot structure and function as a result of complications including peripheral neuropathy, vascular issues, and obesity. Additionally, tissue glycosylation adds rigidity to muscles and joints, exacerbating biomechanical imbalances. These changes lead to increased plantar pressure, impaired balance, and heightened ulceration risk, especially in areas such as the metatarsal heads. The underpinning forces of gravity further contribute to alignment difficulties, pushing the foot toward a more stable, yet problematic, plantar grade position. Understanding and addressing these biomechanical challenges are crucial for effective diabetic foot care, aiming to mitigate risks and enhance patient outcomes.
Why such a focus on diabetes? Numbers tell the story: 38.4 million people in the United States have diabetes, that’s 11.6% of the US population. Only 29.7 million are diagnosed. That leaves 8.7 million people undiagnosed, meaning 22.8% of adults with diabetes are undiagnosed. These are the patients we need to be watching for.
Tissue glycosylation is a prevalent issue in diabetic patients, resulting from the binding of glucose to amino acids, impacting joints, connective tissues, muscles, and nerves throughout the body. This process leads to increased stiffness in tissues, ultimately affecting the biomechanics of the diabetic foot. Understanding the implications of tissue glycosylation is crucial in managing the associated challenges.
Glycosylation results in the stiffening of joints and connective tissues, reducing their flexibility. This decreased range of motion impacts various joints in the foot, including the subtalar and midtarsal joints, contributing to a loss of eversion mobility. Consequently, the rigidity in joints places additional stress on the forefoot, altering load distribution and exacerbating biomechanical inefficiencies.
Reduced tissue flexibility from glycosylation affects overall biomechanical function. The limited joint movement leads to compromised propulsion during walking, where people with diabetes push off with a pronated foot due to the inability to effectively resupinate. This lack of dynamic stability impairs normal gait function, increasing the likelihood of stress-related injuries and ulcerations.
The windlass mechanism, essential for arch stabilization and efficient propulsion, is significantly affected by glycosylation. The stiffening of the plantar fascia disrupts this mechanism, leading to a locked, pronated foot position. This altered foot function transfers excessive force to the forefoot and particularly the interphalangeal joints, commonly resulting in ulceration sites for diabetics.
Challenges of Neuropathic Lower Extremities
 Patients with diabetes often face neuropathic complications which can profoundly influence the biomechanics and health of the lower extremities. These issues arise from both sensory and motor neuropathies, adding to the complexity of diabetic foot care.
Patients with diabetes often face neuropathic complications which can profoundly influence the biomechanics and health of the lower extremities. These issues arise from both sensory and motor neuropathies, adding to the complexity of diabetic foot care.
Muscle Atrophy and Gait Alterations: Chronic neuropathy in these patients contributes to muscle atrophy, particularly in the plantar muscles and larger leg muscles. This atrophy leads to delayed and weakened muscle firing, slowing walking speed and shortening step length. The changes in muscle function result in a more cautious and unstable gait, further increasing musculoskeletal strain.
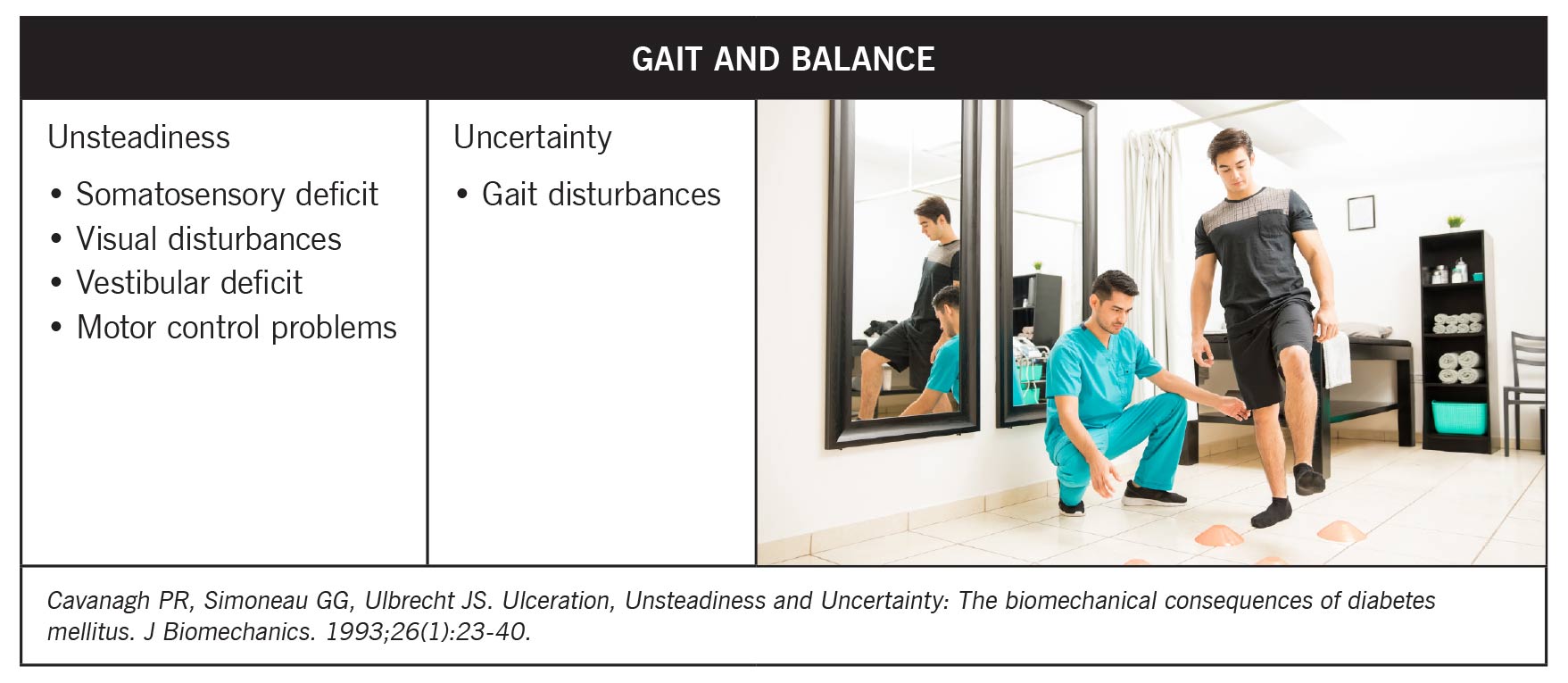
Increased Fall Risk and Balance Issues: Patients with diabetic neuropathy often experience heightened fall risk due to a combination of muscle weakness, sensory deficits, visual impairments, and vestibular issues. Their compromised balance and proprioception make it difficult to recover from stumbles, increasing their susceptibility to falls. Regular assessments and targeted physical therapy focusing on balance and strength can mitigate these risks.
 Importance of Early Sensory Screening: Preventative measures, such as early sensory screening, are invaluable in diabetic foot care. Screening with more sensitive tools, like 1- or 2-gram monofilaments, can detect sensory loss early, allowing for timely intervention and lifestyle changes to slow neuropathy progression. Addressing sensory changes before the complete loss of protective sensation is critical in reducing the risk of ulceration and further complications.
Importance of Early Sensory Screening: Preventative measures, such as early sensory screening, are invaluable in diabetic foot care. Screening with more sensitive tools, like 1- or 2-gram monofilaments, can detect sensory loss early, allowing for timely intervention and lifestyle changes to slow neuropathy progression. Addressing sensory changes before the complete loss of protective sensation is critical in reducing the risk of ulceration and further complications.
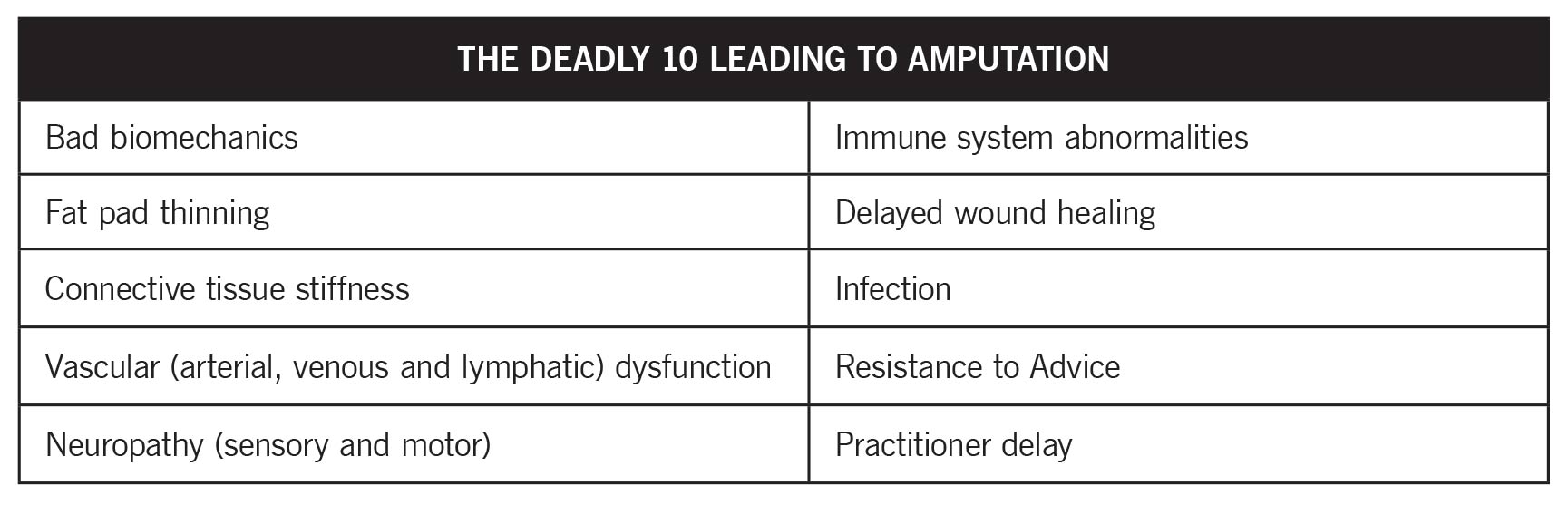
High Amputation Risk: When caring for this patient population, clinicians must be highly vigilant about the multitude of factors that elevate the risk of amputation. Known collectively as the “Deadly 10,” these include bad biomechanics, fat pad thinning, increased connective tissue stiffness due to glycosylation, vascular (arterial, venous and lymphatic) dysfunction, and neuropathy affecting sensory and motor functions. Additional risk factors encompass immune system abnormalities, which impair infection response, and delayed wound healing. A significant risk arises from patient behaviors such as resistance to proper footwear, combined with practitioner delays in addressing these issues proactively.
Addressing Biomechanical Imbalance
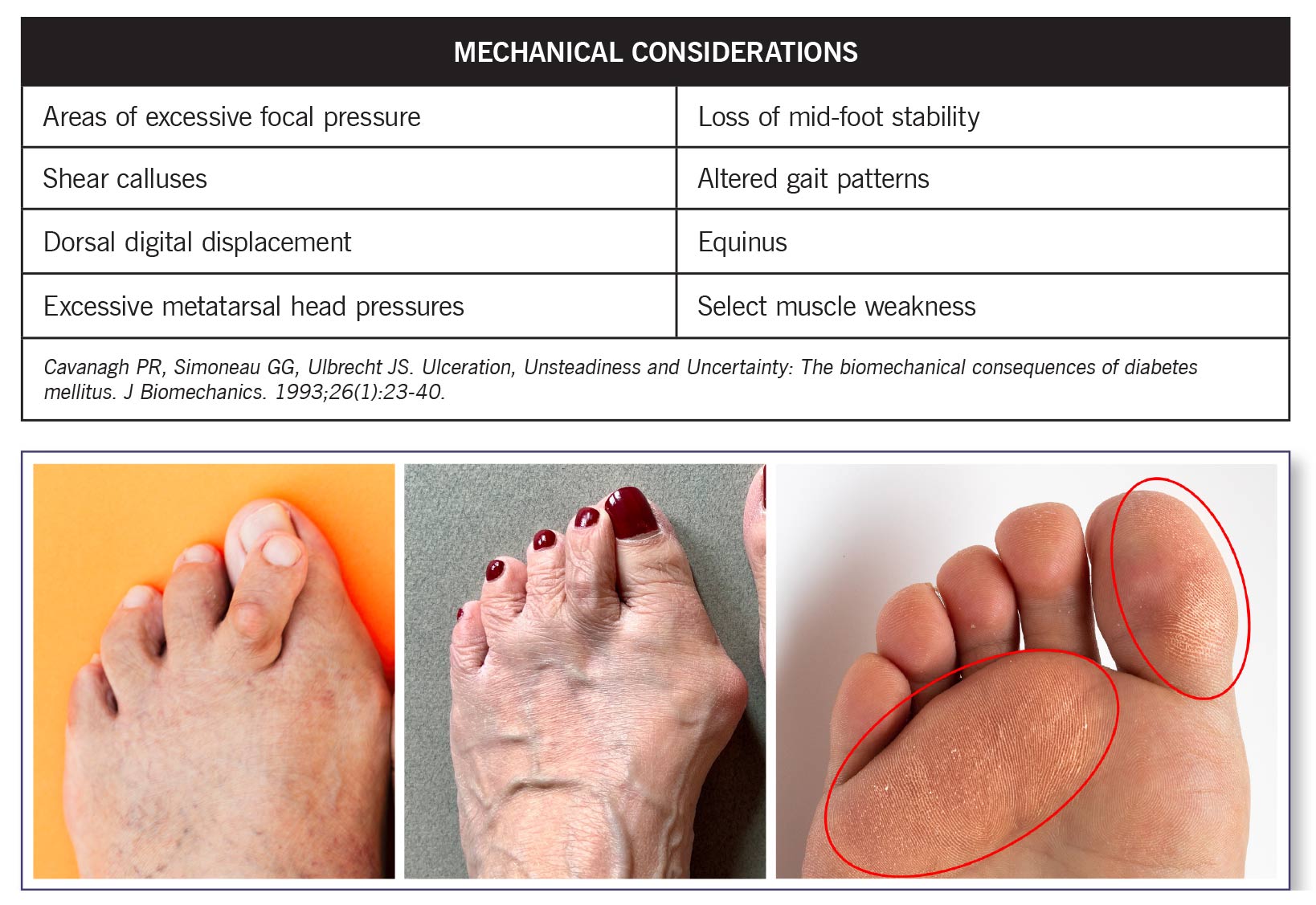
 Diabetes frequently exacerbates underlying skeletal deformities, such as hammer toes, pronation, equinus, and hallux abducto valgus. These malalignments pre-exist in many of these patients, worsening as the disease progresses due to increased glycosylation, leading to stiffer tissues and more diminished flexibility. This compounded misalignment increases focal pressure on joints and metatarsal heads, significantly contributing to ulcerations. Early recognition and corrective intervention for these skeletal issues are vital to mitigate further harm.
Diabetes frequently exacerbates underlying skeletal deformities, such as hammer toes, pronation, equinus, and hallux abducto valgus. These malalignments pre-exist in many of these patients, worsening as the disease progresses due to increased glycosylation, leading to stiffer tissues and more diminished flexibility. This compounded misalignment increases focal pressure on joints and metatarsal heads, significantly contributing to ulcerations. Early recognition and corrective intervention for these skeletal issues are vital to mitigate further harm.
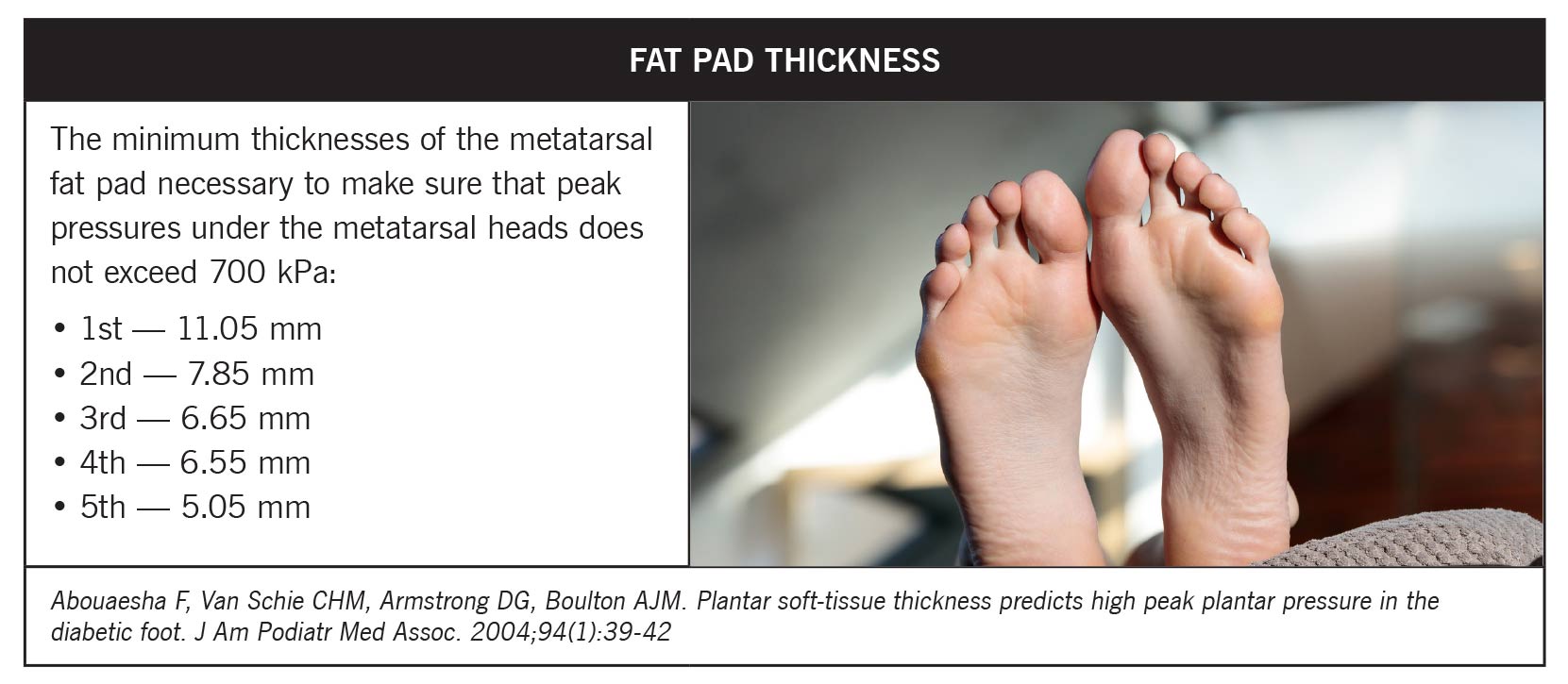
A major challenge in diabetic foot biomechanics is the thinning and stiffening of the metatarsal fat pad. Typically, these fat pads cushion the foot and distribute pressures seamlessly during activity. In people with diabetes, diminished thickness compromises this function, increasing the risk for plantar ulcers. The lowest required thickness thresholds are notably absent in diabetic patients, amplifying plantar pressures and ulcer sites. Emphasizing the maintenance or artificial support of fat pad thickness is crucial in managing these risks.
Addressing these biomechanical issues involves a multi-faceted approach. Incorporating targeted physical therapy programs encourages Achilles stretching to reduce pressure transferred to the forefoot. Custom orthotics can aid in redistributing pressure and correcting gait issues by providing adequate plantar support and realigning foot posture. Additionally, educating patients on lifestyle changes, including diet and exercise, can slow down progressing symptoms and improve overall foot health.
Footwear & Orthotics/Physical Therapy & Stretching
 Footwear and orthotics play a pivotal role in diabetic foot management. Properly fitted shoes with adequate support can prevent pressure-induced injuries and complications. The use of rocker sole designs in diabetic footwear is particularly beneficial. Such designs help offload stress from the forefoot, facilitating smoother and safer gait by reducing peak plantar pressures. Orthotic devices, whether rigid or accommodative, support foot alignment, provide total contact for pressure distribution, and minimize high-pressure spots prone to calluses or ulcers. Engaging patients in the selection of appropriate footwear and overcoming vanity or resistance to recommended options is crucial. Educating patients on the long-term benefits of recommended footwear choices can help prevent re-ulceration and potential amputations, empowering them to actively participate in their care and management.
Footwear and orthotics play a pivotal role in diabetic foot management. Properly fitted shoes with adequate support can prevent pressure-induced injuries and complications. The use of rocker sole designs in diabetic footwear is particularly beneficial. Such designs help offload stress from the forefoot, facilitating smoother and safer gait by reducing peak plantar pressures. Orthotic devices, whether rigid or accommodative, support foot alignment, provide total contact for pressure distribution, and minimize high-pressure spots prone to calluses or ulcers. Engaging patients in the selection of appropriate footwear and overcoming vanity or resistance to recommended options is crucial. Educating patients on the long-term benefits of recommended footwear choices can help prevent re-ulceration and potential amputations, empowering them to actively participate in their care and management.
Physical therapy (PT) is greatly underutilized yet essential in managing diabetes-related foot complications. PT programs focusing on Achilles stretching can improve ankle range of motion and alleviate forefoot pressure. Balance and gait training enhance proprioceptive feedback, reduce the fall risk, and strengthen muscles weakened by neuropathy. Regular PT engagement can address the destabilizing impact of neuromuscular deficits in diabetic patients.
Conclusion
 The biomechanics of the diabetic foot presents unique challenges in managing the neuropathic lower extremity. Addressing these complexities necessitates a multifaceted approach, involving proper footwear, orthotics, physical therapy, and patient education. Clinicians must be proactive in recognizing risk factors and intervening early. Factors like peripheral vascular disease, tissue glycosylation, and fat pad atrophy significantly impact the foot’s health. By adopting comprehensive strategies, including frequent monitoring and employing tools like rocker sole shoes and specialized orthotics, healthcare providers can reduce the risk of ulceration and amputation, enhancing overall diabetes care and foot health.
The biomechanics of the diabetic foot presents unique challenges in managing the neuropathic lower extremity. Addressing these complexities necessitates a multifaceted approach, involving proper footwear, orthotics, physical therapy, and patient education. Clinicians must be proactive in recognizing risk factors and intervening early. Factors like peripheral vascular disease, tissue glycosylation, and fat pad atrophy significantly impact the foot’s health. By adopting comprehensive strategies, including frequent monitoring and employing tools like rocker sole shoes and specialized orthotics, healthcare providers can reduce the risk of ulceration and amputation, enhancing overall diabetes care and foot health.
James McGuire, DPM, LPT, LPed, FAPWHc, is Director of the Leonard S. Abrams Center for Advanced Wound Healing and Professor at Temple University School of Podiatric Medicine.
This article is a summary of Dr. McGuire’s presentation titled, “Biomechanics of the Diabetic Foot; Unique Challenges of the Neuropathic Lower Extremity,” from the 2025 No-Nonsense Seminar, March 7-9, 2025, hosted by the North Central Ohio Academy of Podiatric Medicine. To view the 60-minute slide presentation with questions and answers, visit https://nononsense2025.lerexpo.com/. Continuing education credits are available for many lerEXPO programs.





