 By Patrick DeHeer, DPM FACFAS, FFPM RCPS (Glasg)
By Patrick DeHeer, DPM FACFAS, FFPM RCPS (Glasg)
Non-Weight-Bearing Examination
The non-weight-bearing examination is the foundation of a comprehensive biomechanical assessment. It allows the clinician to evaluate intrinsic structure, available joint range of motion, and inherent pathomechanics without the confounding influence of body weight and compensation. Isolating individual joints and segments in an unloaded state is critical for identifying pathology, determining deformity correctability, and establishing a reliable baseline that informs all subsequent clinical decision-making. Understanding the foot and ankle in this state allows for more accurate interpretation once the patient is standing and walking.
Ankle Joint Range of Motion
The ankle joint functions around a triplanar axis that deviates significantly from the cardinal planes—approximately 82° from the sagittal plane, 8° from the transverse plane, and 20–30° from the frontal plane. Because of this orientation, dorsiflexion and plantarflexion represent the primary observable motions.
Normal total ankle range of motion is approximately 65–75°, typically consisting of 10–20° of dorsiflexion and 40–45° of plantarflexion.
Functional requirements vary by activity. Normal gait requires only about 30° of total ankle motion, whereas stair climbing and incline walking demand substantially more—often 37–56°.
 Clinical Interpretation
Clinical Interpretation
- Decreased dorsiflexion suggests anterior ankle impingement or an osseous block.
- Decreased plantarflexion may indicate posterior impingement, including os trigonum pathology.
- Absent motion is highly concerning and typically reflects advanced osteoarthritis or prior ankle arthrodesis.
Equinus Assessment (Silfverskiöld Test)
The Silfverskiöld test remains a cornerstone of the biomechanical exam, primarily for distinguishing gastrocnemius from gastro-soleal equinus. However, its role has evolved. While essential for documentation, it should no longer be used in isolation to dictate the choice between tendo-Achilles lengthening and gastrocnemius recession.
The traditional “Root method,” which places the subtalar joint in neutral, has demonstrated poor inter- and intra-rater reliability and should be considered outdated. An evidence-based alternative emerged in 2017.
Gatt et al. demonstrated superior reliability using a maximal supination technique. Dayton et al. corroborated these findings radiographically, showing that the tibiotalar angle remains unchanged between pronated and supinated foot positions—confirming that observed differences in motion are due to soft-tissue restriction rather than osseous alignment.
 Evidence-Based Technique
Evidence-Based Technique
- Position the patient prone or supine.
- Maximally supinate the foot to lock the midtarsal joint.
- With the knee fully extended, dorsiflex the hindfoot and measure motion.
- Repeat with the knee flexed.
While often labeled “ankle dorsiflexion,” this motion more accurately represents hindfoot dorsiflexion, as ankle and subtalar motion cannot be clinically isolated.
Pathologic equinus is defined as –5° or less of dorsiflexion with the foot maximally supinated and the knee extended.
Functionally, normal gait requires 10–20° of dorsiflexion during the second rocker. When this is unavailable, compensation occurs. Proximal compensation may include excessive knee and hip flexion or increased lumbar lordosis. More commonly, compensation occurs distally as sagittal-plane collapse through the midfoot—often at the naviculocuneiform joint—placing pathologic stress on the posterior tibial tendon and spring ligament.
Subtalar Joint Range of Motion
Subtalar joint (STJ) assessment is critical, particularly for distinguishing flexible from rigid flatfoot deformities. Normal motion consists of approximately 25–30° of inversion and 5–10° of eversion, for a total arc of 30–40°.
A key clinical question—especially in cavus evaluation—is whether the heel can evert to perpendicular. This single finding is often more surgically relevant than the Coleman block test. Failure to evert suggests a rigid deformity that may be better treated with subtalar arthrodesis rather than osteotomies.
STJ axis position has significant implications. A medially deviated axis predisposes to pronation and arch collapse, whereas a laterally deviated axis reinforces cavus mechanics.
Decreased STJ motion is commonly seen following ankle arthrodesis and after Evans calcaneal osteotomy, which has been shown to reduce STJ motion by approximately 30%.
Midtarsal Joint Examination
With the heel neutralized to lock the subtalar joint, the forefoot is assessed through all 3 planes of motion. This serves as an effective screening tool for midfoot arthritis and tarsal coalitions, including naviculocuneiform coalition.
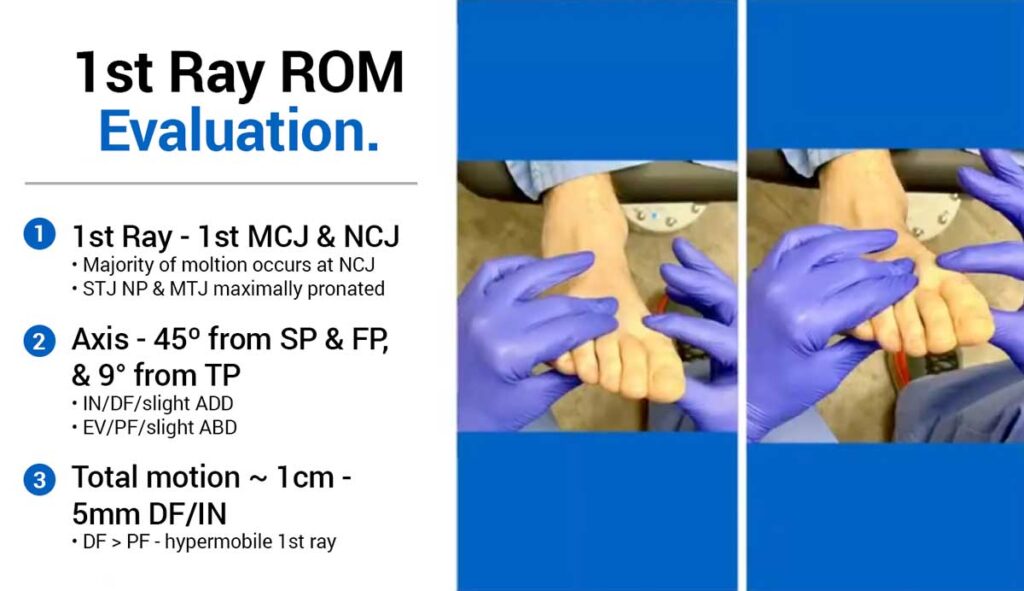
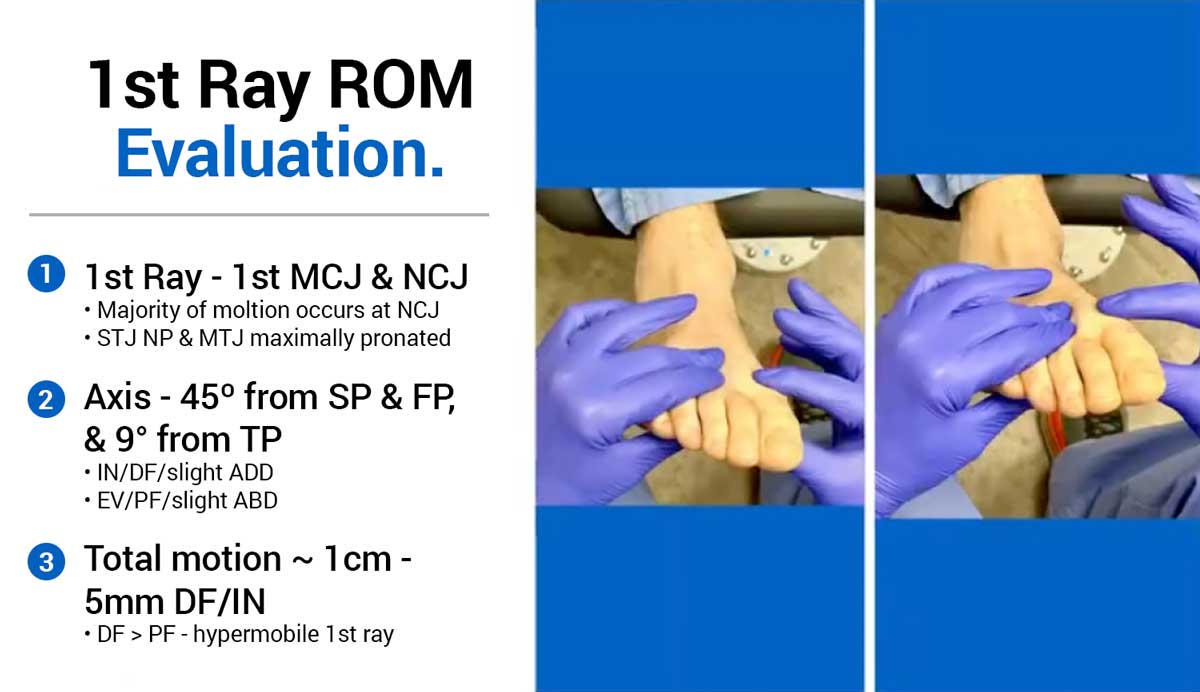
First Ray Examination
The first ray—comprising the first metatarsocuneiform and naviculocuneiform joints—moves along a triplanar axis approximately 45° from both sagittal and frontal planes.
Technique
- Place the subtalar joint in neutral.
- Maximally pronate the midtarsal joint to lock it.
- Stabilize rays 2–5.
- Move the first ray dorsally and plantarly.
Normal motion is less than 1 cm, with relatively equal dorsal and plantar excursion. Hypermobility is defined by excessive dorsal motion relative to plantar motion.
Windlass Activation Test (Non-Weightbearing)
Passive hallux dorsiflexion is added to the first-ray exam to engage the windlass mechanism. Stabilization of the first ray indicates an intact windlass.
This finding directly impacts flatfoot surgical planning. An intact windlass favors medial column correction with a Cotton osteotomy. Persistent motion despite hallux dorsiflexion indicates windlass incompetence.
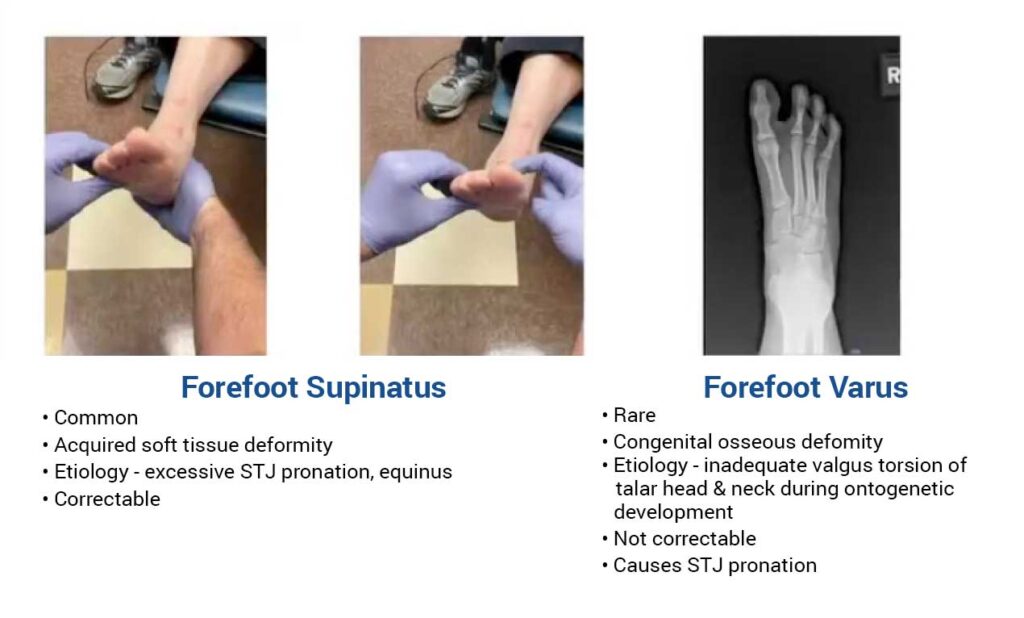
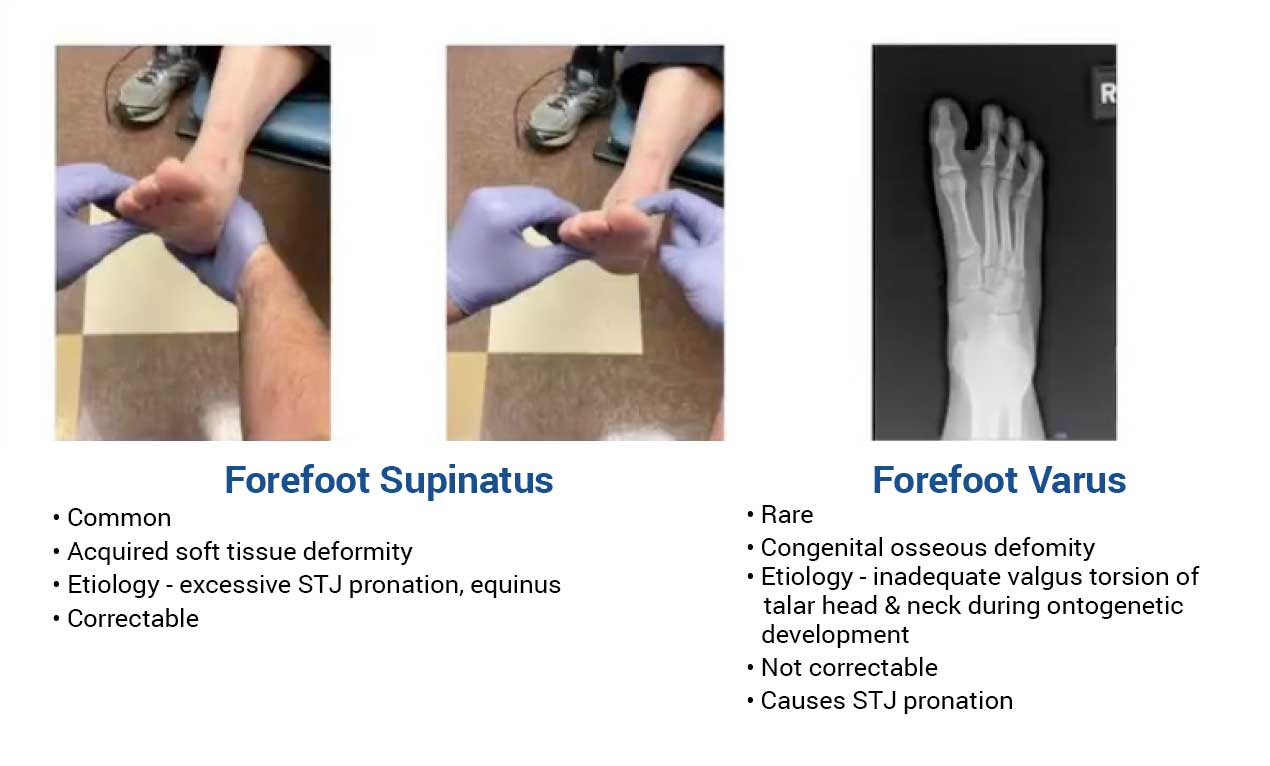
Forefoot-to-Rearfoot Evaluation
With the subtalar joint neutral and the midtarsal joint locked, the plane of the metatarsal heads is compared to the calcaneal bisection.
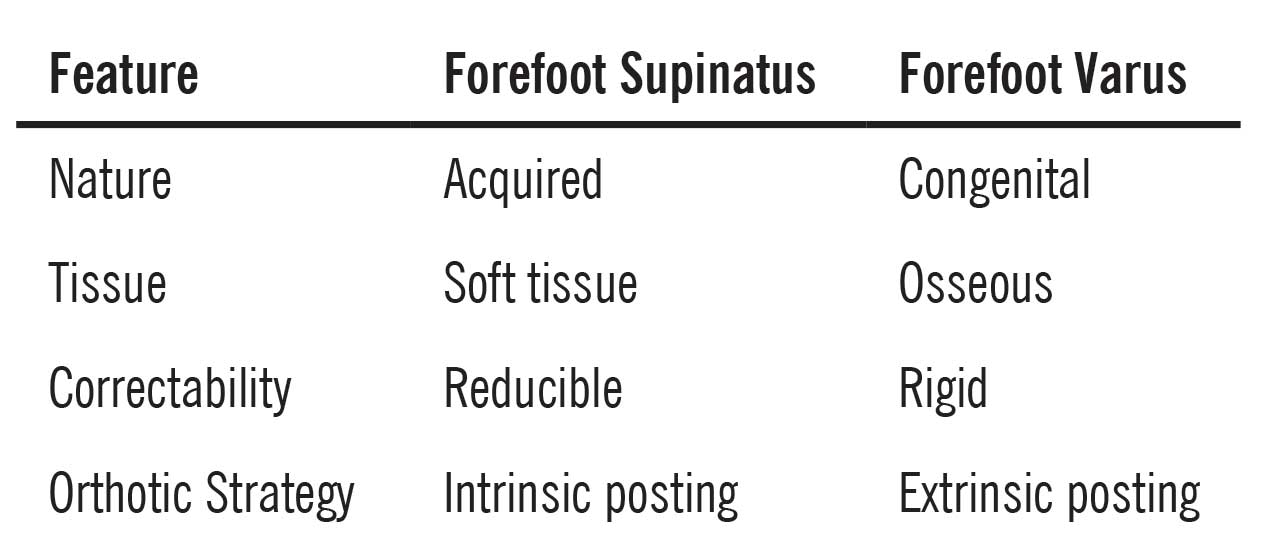
Failure to fully correct a flexible forefoot supinatus converts it into a rigid, iatrogenic forefoot varus. Compensation then shifts proximally—often to the ankle—risking deltoid ligament failure and ankle valgus. For this reason, some surgeons intentionally slightly overcorrect to forefoot valgus intraoperatively.
First Metatarsophalangeal Joint Motion
Non-weight-bearing dorsiflexion should exceed 65°. During weight-bearing, this decreases to approximately 20–40° due to blocked first-ray plantarflexion. A useful rehabilitation pearl is comparing hallux dorsiflexion to that of the second toe to provide patients with a clear visual benchmark.
 Weight-Bearing Examination
Weight-Bearing Examination
Weight-bearing assessment reveals the functional consequences of previously identified pathomechanics. Static observations provide context for dynamic gait analysis.
Standardized Stance
Patients should stand in the Saltzman–El-Khoury “straight position”—feet parallel and shoulder-width apart—for consistency and reliability.
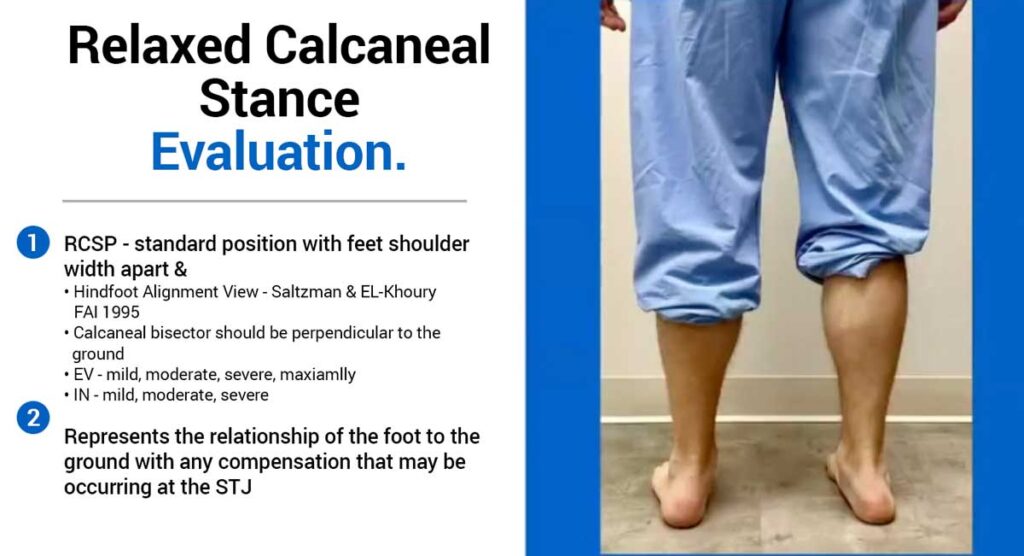
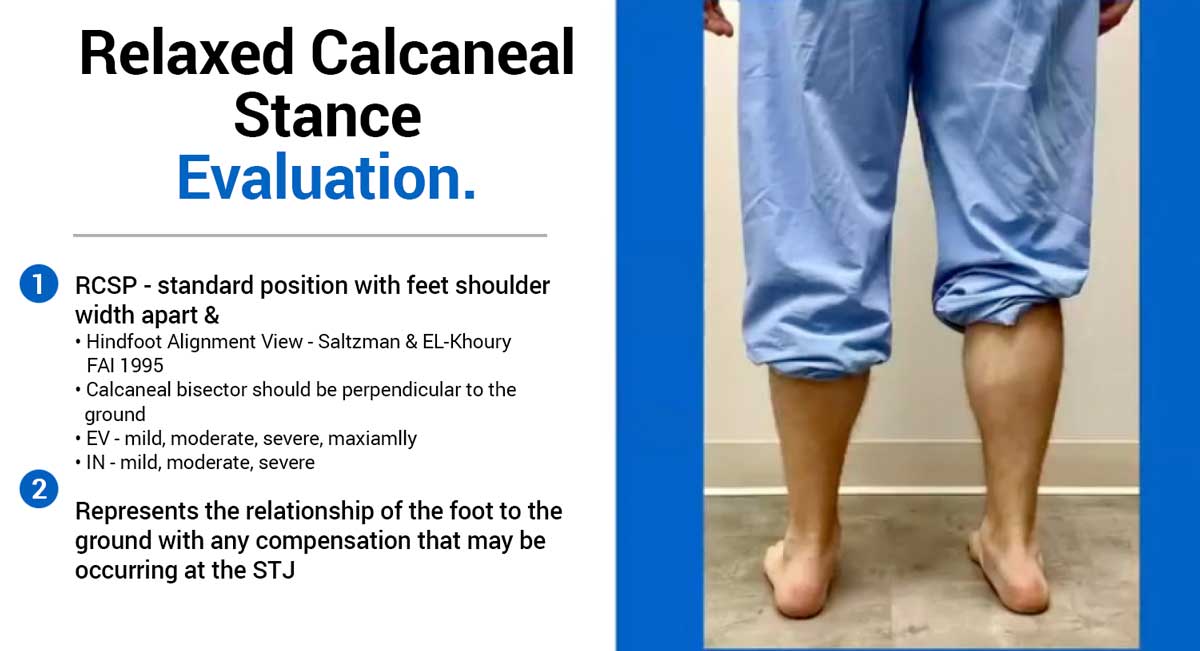
Resting Calcaneal Stance Position
Heel position is observed posteriorly and documented qualitatively as mild, moderate, severe, or maximally everted/inverted.
Medial Arch
Arch height is assessed visually and documented as increased or decreased (mild to collapsed).
Heel Rise Testing
- Double-limb heel rise: Assesses plantarflexion strength and hindfoot reducibility.
- Single-limb heel rise: Isolates posterior tibial tendon function. Inability to perform indicates advanced flatfoot pathology.
Hubscher Maneuver
Passive hallux dorsiflexion during stance assesses windlass function. A positive test recreates the arch and inverts the heel. Patients must remain relaxed to avoid false results.
Dynamic Gait Analysis
Gait analysis synthesizes all prior findings and is indispensable to accurate diagnosis.
Technique
- Examiner seated low.
- Patient walks toward and away multiple times.
- Smartphone video allows slow-motion review.
- Evaluate each limb independently.
Rocker System Overview
- First rocker: Anterior group eccentrically controls foot slap.
- Second rocker: Posterior tibial, intrinsics, peroneus longus, and soleus eccentrically stabilize and slow tibial progression.
- Third rocker: Gastrocnemius contraction engages the windlass, locking Chopart’s joint while the peroneus longus stabilizes Lisfranc’s joint.
- Swing phase: Anterior group clears the foot; peroneus brevis prepares for heel strike.
Common Pathologic Gait Patterns
Antalgic, apropulsive, calcaneal, steppage, scissoring, in-toeing, hemiplegic, and toe-walking patterns each provide diagnostic clues.
Special Considerations
Limb Length Inequality
Weight-bearing long-leg radiographs are the gold standard. Tape measurements are unreliable and should not guide treatment.
Shoe Wear Analysis
Outsole wear, toe-box creasing, and insole pressure patterns often reveal chronic compensation strategies.
Conclusion
Dynamic gait analysis is not optional—it is central to high-level biomechanical evaluation. The ability to integrate static findings with real-time movement distinguishes true diagnosticians from technicians and directly drives better conservative and surgical outcomes.
Patrick A. DeHeer, DPM, is a board-certified podiatric surgeon and pediatric specialist with extensive experience in complex foot and ankle pathology. He is in private practice and serves patients at Hoosier Foot & Ankle. Dr. DeHeer completed his podiatric medical degree at the Dr. William M. Scholl College of Podiatric Medicine, residency training in Indianapolis, and a fellowship in foot and ankle arthroscopy. He is double board-certified and serves as team podiatrist for the Indiana Pacers and Indiana Fever. He is the founder of Step-by-Step Haiti and Foot Aid and has completed over 25 international medical missions.
This article summarizes Dr. DeHeer’s presentation, “Practical Biomechanical Exam: Information That Actually Drives Better Conservative and Surgical Treatment,” delivered at the 2025 No-Nonsense Seminar (March 7–9). To view the full presentation with audience questions and answers—and to see the complete agenda for the 3-day program—visit https://nononsense2025.lerexpo.com. Continuing education credits are available for this and many other lerEXPO programs.






Some great reminders here. Thanks Dr. DeHeer!