

By Dr. Hooman Mir, DPM, MSci, FAPWCA
UTRGV, School of Podiatric Medicine
Department of Podiatric Medicine, Surgery & Biomechanics
Orthokine® is the proprietary name for a German-developed autologous conditioned serum (ACS) therapy now advanced in musculoskeletal medicine for joint pain. In scientific literature and clinical contexts, Orthokine is used interchangeably with the generic designation autologous conditioned serum (ACS), with PubMed-indexed authors favoring ACS for generalizability. This distinction matters for practitioners and researchers tracking the evolution and efficacy of biologics in orthopedic settings. This article reviews the history, science, clinical application, advanced techniques, and safety outcomes for ACS (Orthokine) and enhanced platelet-rich plasma (PRP) therapies—emphasizing their transformative role in lower extremity joint care.
Historical Evolution of PRP and ACS
PRP was originally developed in the mid-20th century for hematologic treatments, then gained traction in surgery, wound care, and orthopedics through the 1980s–1990s. Activated platelets release growth factors and cytokines accelerating tissue repair. In Germany during the late 1990s, Orthokine emerged as the leading ACS approach—where patient blood is incubated with glass beads, creating serum highly enriched in anti-inflammatory agents, especially interleukin-1 receptor antagonist (IL-1Ra). Today, both PRP and ACS form the pillars of biologic therapy in osteoarthritis and sports injuries.
 Science and Physiology
Science and Physiology
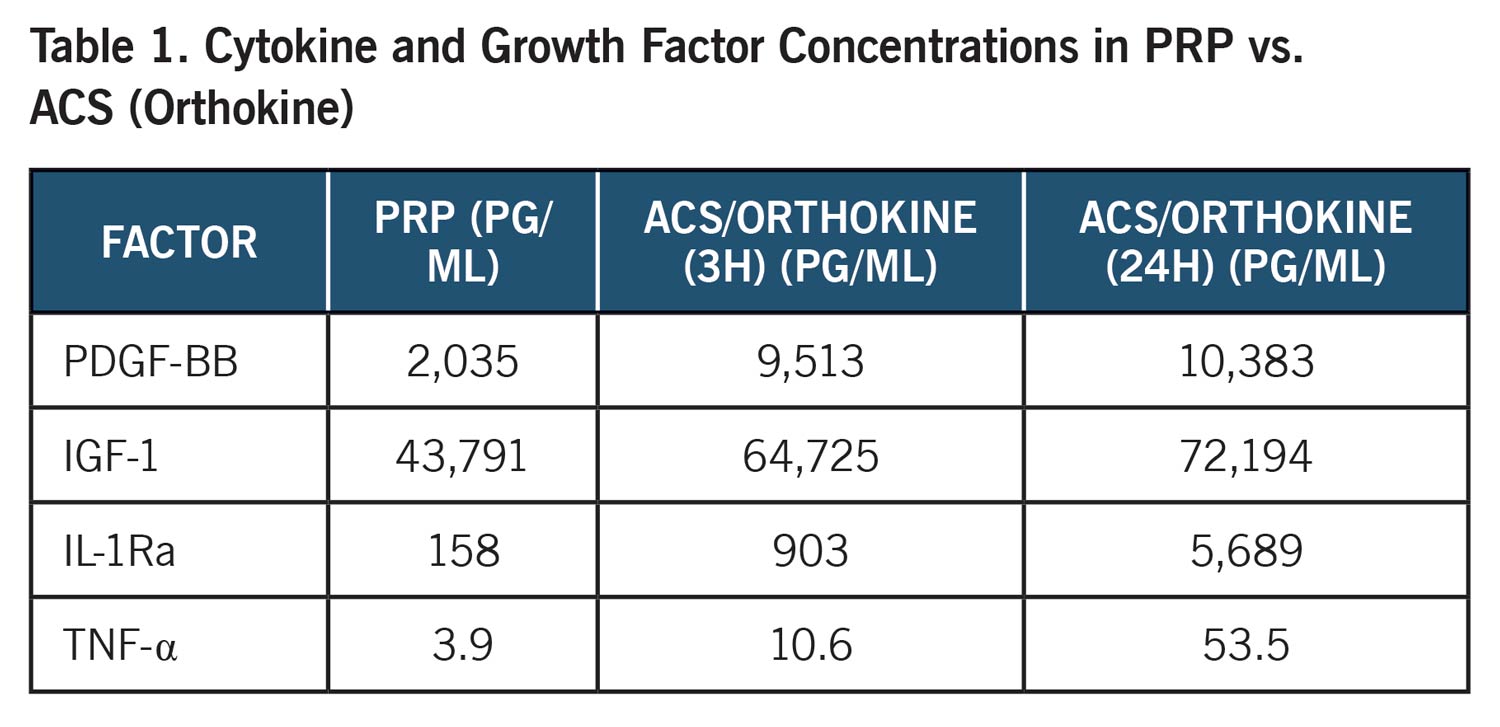
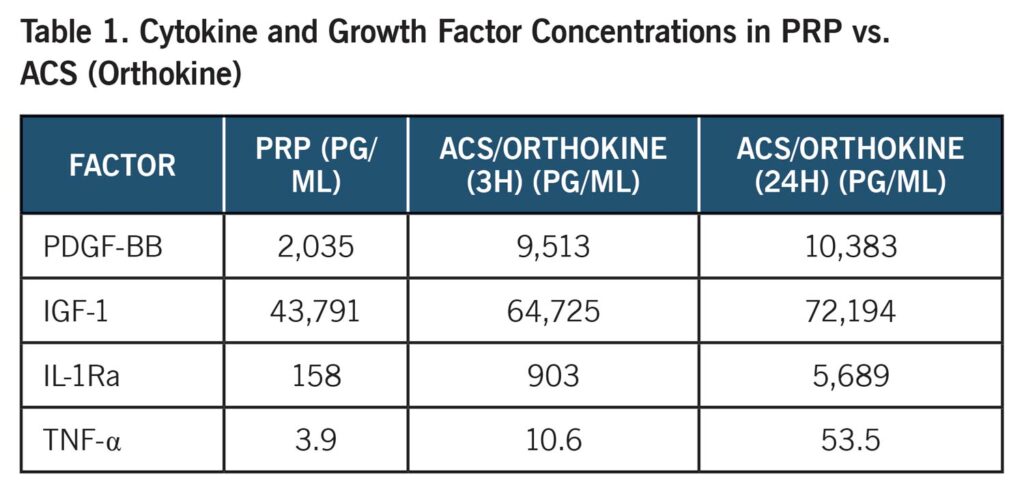
Growth Factors, Cytokines, and Mechanisms
Platelets—and monocyte incubation with glass beads—produce key molecules for healing:
PDGF, IGF-1, TGF-β, VEGF, EGF and IL-1Ra (Orthokine/ACS focus)
Orthokine/ACS magnifies IL-1Ra and growth factors, directly suppressing cytokine-driven joint degeneration.
 Clinical Applications in the Lower Extremity
Clinical Applications in the Lower Extremity
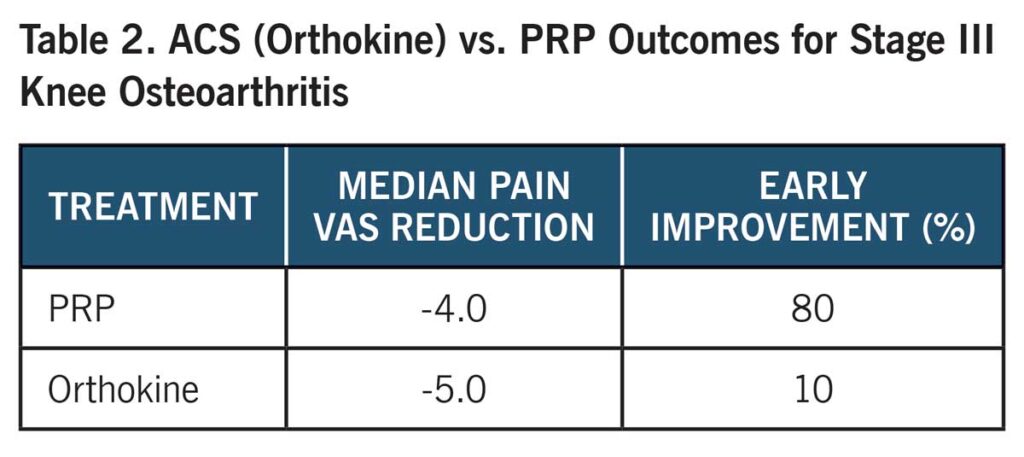
Knee Joint
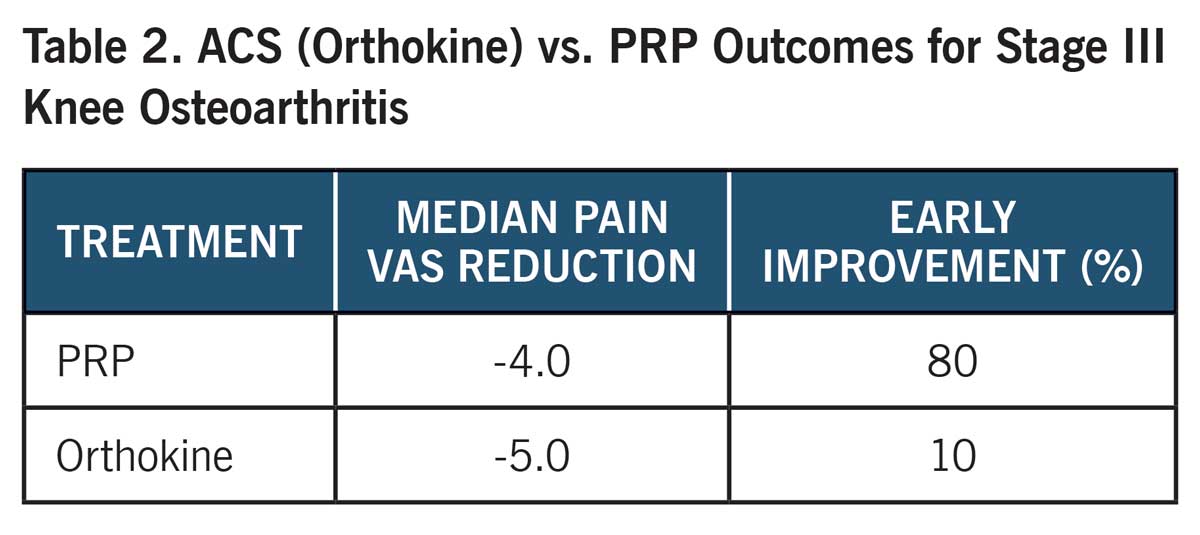
PRP and ACS/Orthokine therapy are established for knee osteoarthritis, with meta-analyses and RCTs showing pain relief, functional improvement, and patient satisfaction exceeding that of hyaluronic acid and corticosteroids.
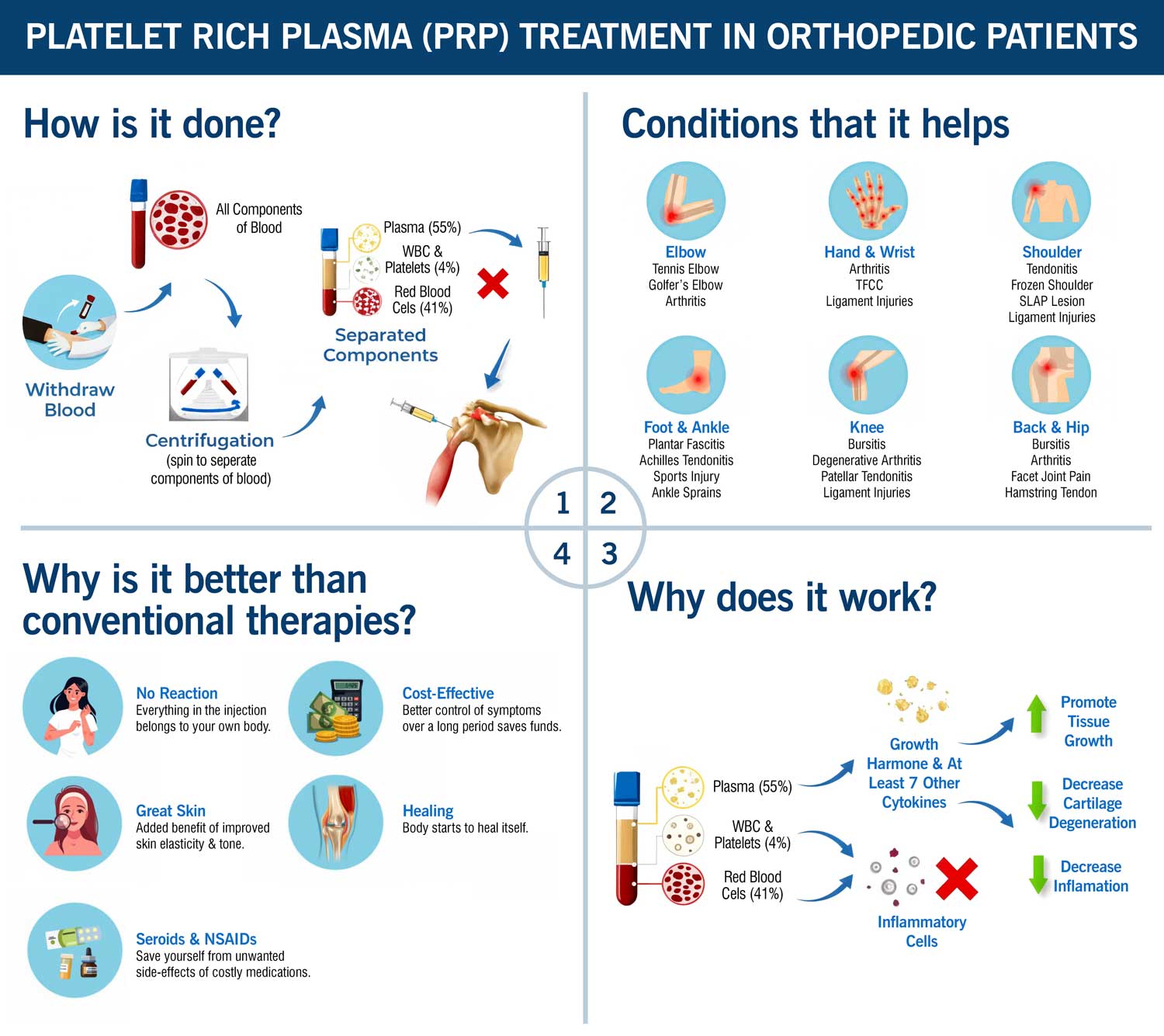
 Figure: Schematic representation of platelet-rich plasma (PRP) knee therapy. The image shows blood collection, centrifugation to concentrate platelets, and targeted injection into the knee joint for regenerative treatment of joint pain. |
 Figure: Clinical administration of platelet-rich plasma (PRP) therapy for knee osteoarthritis. A physician in sterile technique injects PRP directly into the knee joint to promote tissue regeneration and reduce pain. |
 Ankle Joint and Sinus Tarsi
Ankle Joint and Sinus Tarsi
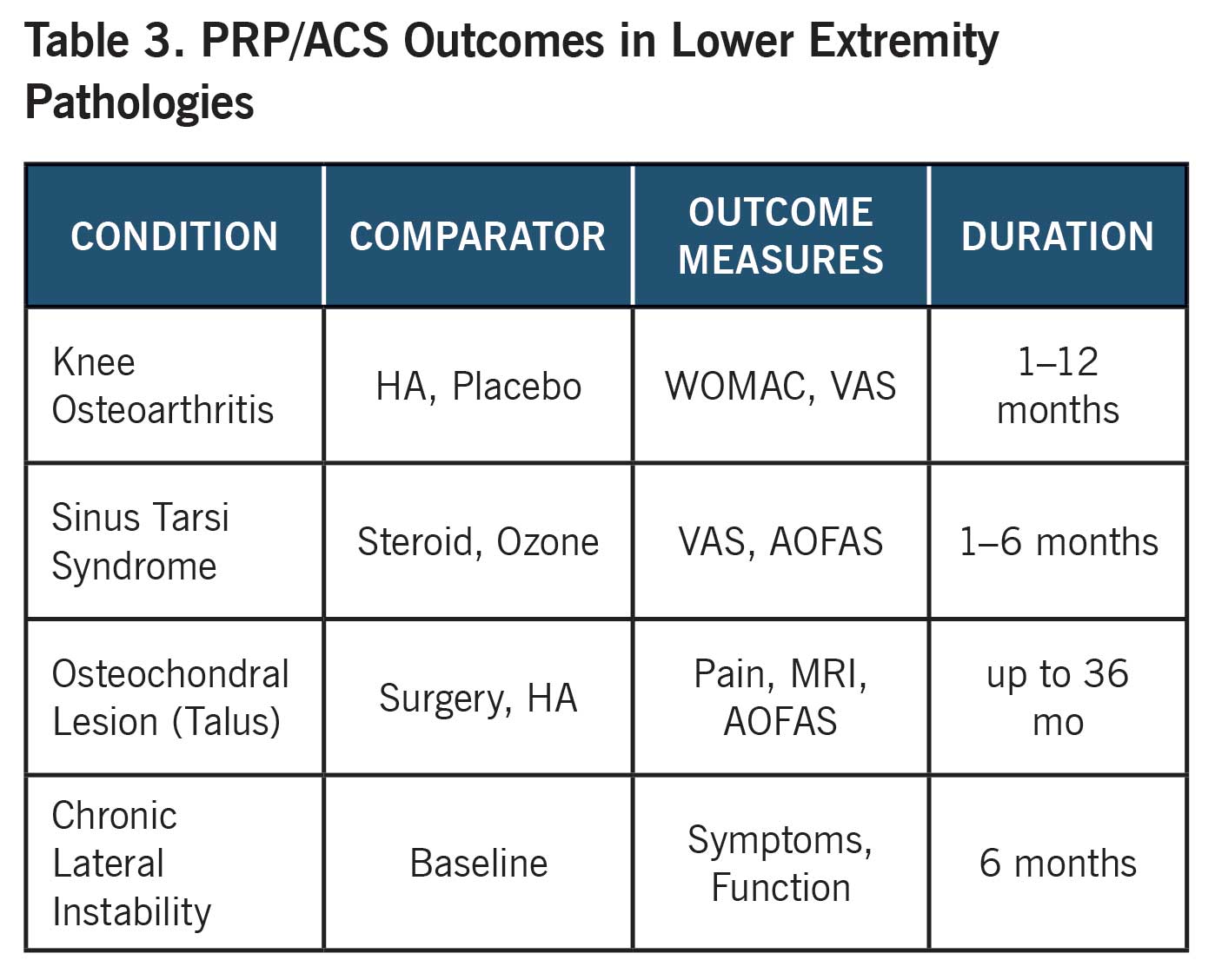
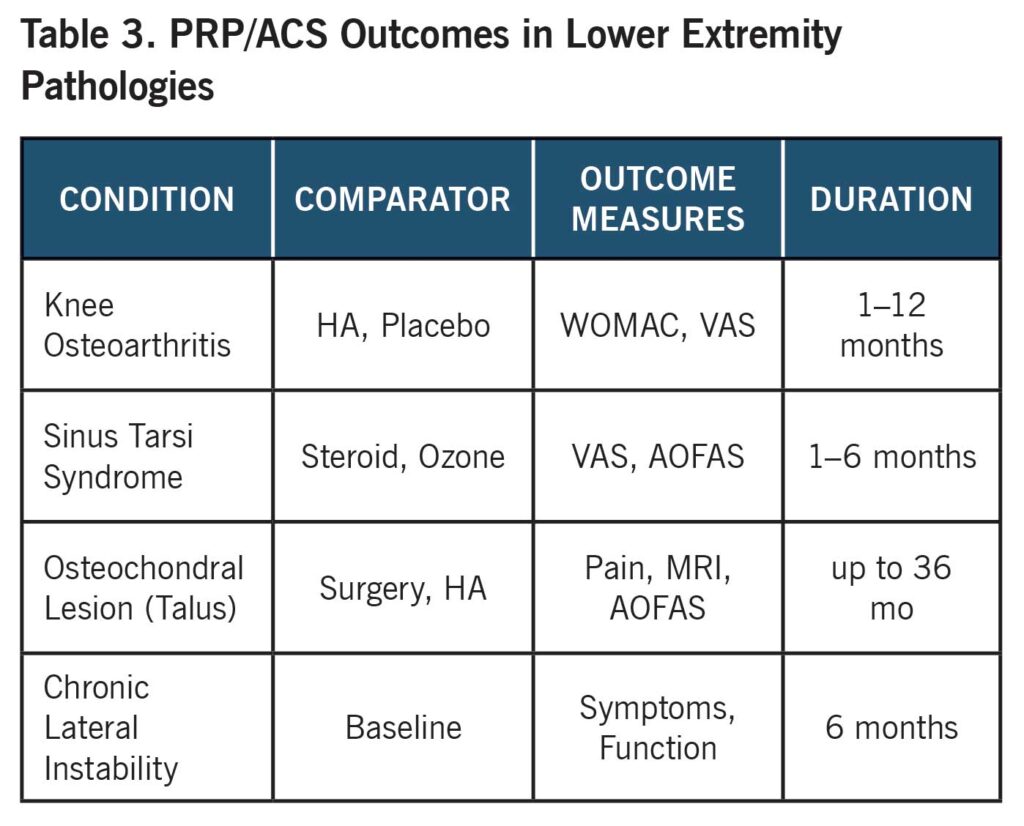
ACS and PRP are expanding to ankle OA, osteochondral lesions, and sinus tarsi syndrome—where inflammation predominates after trauma.
- Sinus tarsi syndrome: PRP/ACS are as effective as steroid and ozone, with better durability of relief.
- Osteochondral talar lesions: PRP/ACS used as stand-alone or with scaffolds, resulting in functional and imaging improvements.
- Chronic ankle instability: PRP speeds symptom reduction and rehabilitation outcomes.

Figure: Platelet-rich plasma (PRP) injection for ankle joint pathology. The procedure involves delivery of PRP into the ankle region to support healing of musculoskeletal injuries and reduce pain in conditions such as tendonitis or osteoarthritis.

Figure: Preparation of platelet-rich plasma (PRP) for therapeutic use. A technician places a blood sample into a centrifuge to separate components and concentrate platelets, a critical step in producing PRP for joint injections.
Most Advanced and Innovative Techniques
Contemporary ACS/Orthokine and PRP care utilizes:
- Ultrasound-guided injections for precise delivery intra- or peri-articularly.
- Custom ACS conditioning protocols (varying incubation, dosing).
- Combination treatment (PRP + hyaluronic acid/scaffold).
- Disease-modifying approaches for early-stage OA.
Safety, Risks, and Limitations
PRP and ACS have strong safety records. Reported adverse events are rare but happen (refer to table 4).
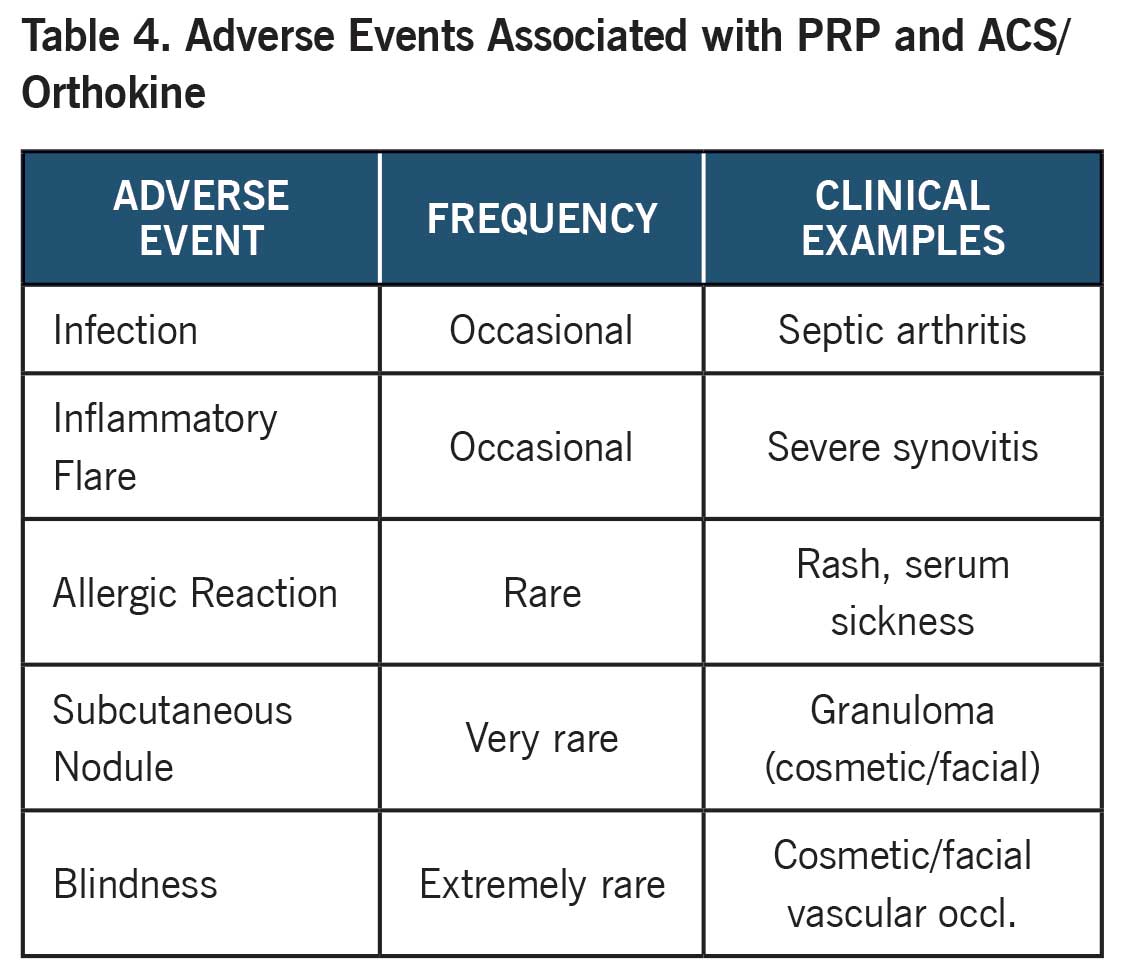
Carefully controlled preparation and patient screening are essential to minimize risks and optimize efficacy.
Dr. Hooman Mir, DPM, MSci, FAPWCA, is a Tenure-Track Assistant Professor of Medicine and Faculty Senator at UTRGV School of Podiatric Medicine. Dr. Mir is an alumnus of Temple University School of Podiatric Medicine and completed his surgical internship at Mount Sinai Hospital in New York. Dr. Mir’s commitment to podiatric academic medicine is defined by a series of distinctive firsts: the first Doctor of Podiatric Medicine (DPM) to receive full NIH tuition reimbursement for a Master of Science in Clinical Investigation at UT Health San Antonio; the first DPM to graduate from Harvard Medical School’s prestigious T2T Program; the first DPM and only faculty member in the UTRGV Health System inducted into the historic Harvard Club of Boston; and the first DPM at UTRGV Health System ever to be accepted into the School of Medicine’s PhD program in Human Genetics—focused on Precision Medicine in Diabetes—now embarking on his second year of doctoral study.
- Cheng, P. G., Yang, K. D., Huang, L. G., Wang, C. H., Ko, W. S., & Toh, W. S. (2023). Comparisons of cytokines, growth factors and clinical efficacy between platelet-rich plasma and autologous conditioned serum for knee osteoarthritis management. Biomolecules, 13(3), 555. https://doi.org/10.3390/biom13030555
- Arita, A., & Tobita, M. (2024). Adverse events related to platelet-rich plasma therapy and future issues to be resolved. Regen Ther, 26, 496–501. https://doi.org/10.1016/j.reth.2024.07.004
- PRP Injections for the Treatment of Knee Osteoarthritis. (2025). PMCID: PMC11874499.
- Platelet-rich plasma therapy: an effective approach for managing knee osteoarthritis. (2023). PMCID: PMC10729545.





