
By Leland Jaffe, DPM, FACFAS.CWSP
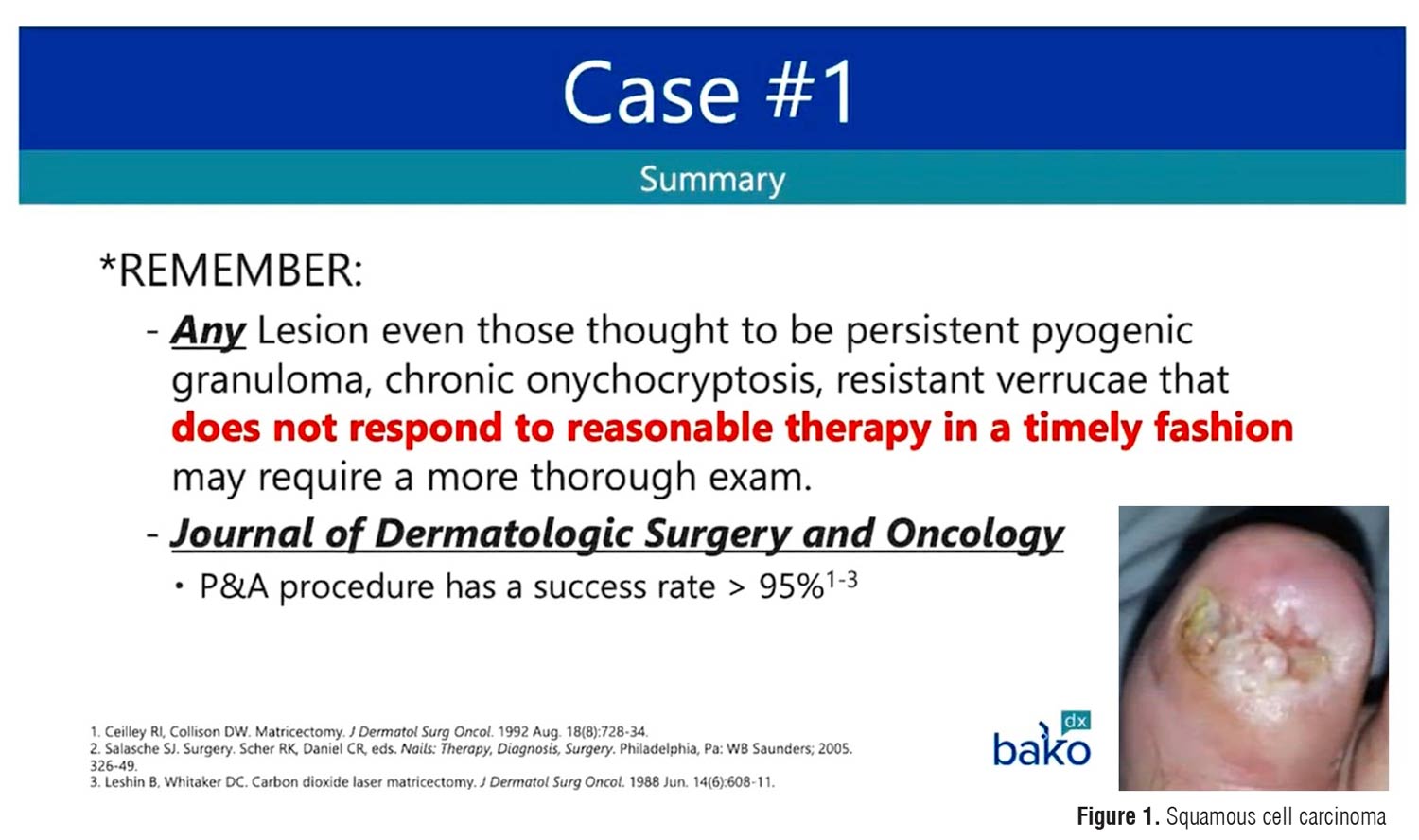
1. Why is performing a biopsy so important in podiatric dermatology? Performing a biopsy is crucial for achieving diagnostic accuracy. Podiatric physicians may biopsy less frequently than their dermatology counterparts, but an earlier biopsy can significantly improve patient care. Many skin conditions can mimic common podiatric issues, and a biopsy allows for histopathological examination, which can definitively rule out or confirm various diagnoses, including malignancies, inflammatory conditions, and infections. Delaying biopsy when treatment is ineffective can lead to prolonged suffering and potentially worse outcomes, as illustrated by the case of the squamous cell carcinoma initially misdiagnosed as a chronic ingrown toenail issue.
2. What “red flags” should prompt a podiatric physician to consider a biopsy for a nail or skin condition? Several clinical scenarios should raise suspicion and prompt consideration for a biopsy. These include:
- Lack of response to standard treatments: If a common condition such as an ingrown nail or presumed fungal infection doesn’t improve with appropriate therapy within a reasonable timeframe (eg, 2 chemical matrixectomies without success or lack of improvement with antifungal treatment), further investigation is warranted.
- Unusual presentation or location: Lesions appearing in atypical locations (eg, a non-healing ulcer on the side of a toe or a lesion on a non-weightbearing surface that resembles a diabetic foot ulcer) should be viewed with suspicion.
- Prolonged duration or progression: Skin lesions or wounds that persist for an extended period (eg, a wound present for 4–6 years without typical venous disease signs) or show progressive changes despite treatment should be biopsied to rule out underlying pathology, including malignancy.
- Suspicious clinical features: While not always obvious, changes in a lesion’s appearance, such as rapid growth, unusual coloration (or lack thereof in cases of amelanotic melanoma), or features inconsistent with the presumed diagnosis, should increase the index of suspicion for a more serious condition.
- History of predisposing factors: A history of significant trauma (eg, previous burn injury) in the area of a non-healing wound should raise suspicion for malignant degeneration (Marjolin’s ulcer) and necessitate early biopsy.
3. What are some examples of diagnostic miscues you’ve seen in your practice?
- A squamous cell carcinoma (Figure 1) of the great toenail bed initially treated as a recurring ingrown toenail with multiple phenol matrixectomies.
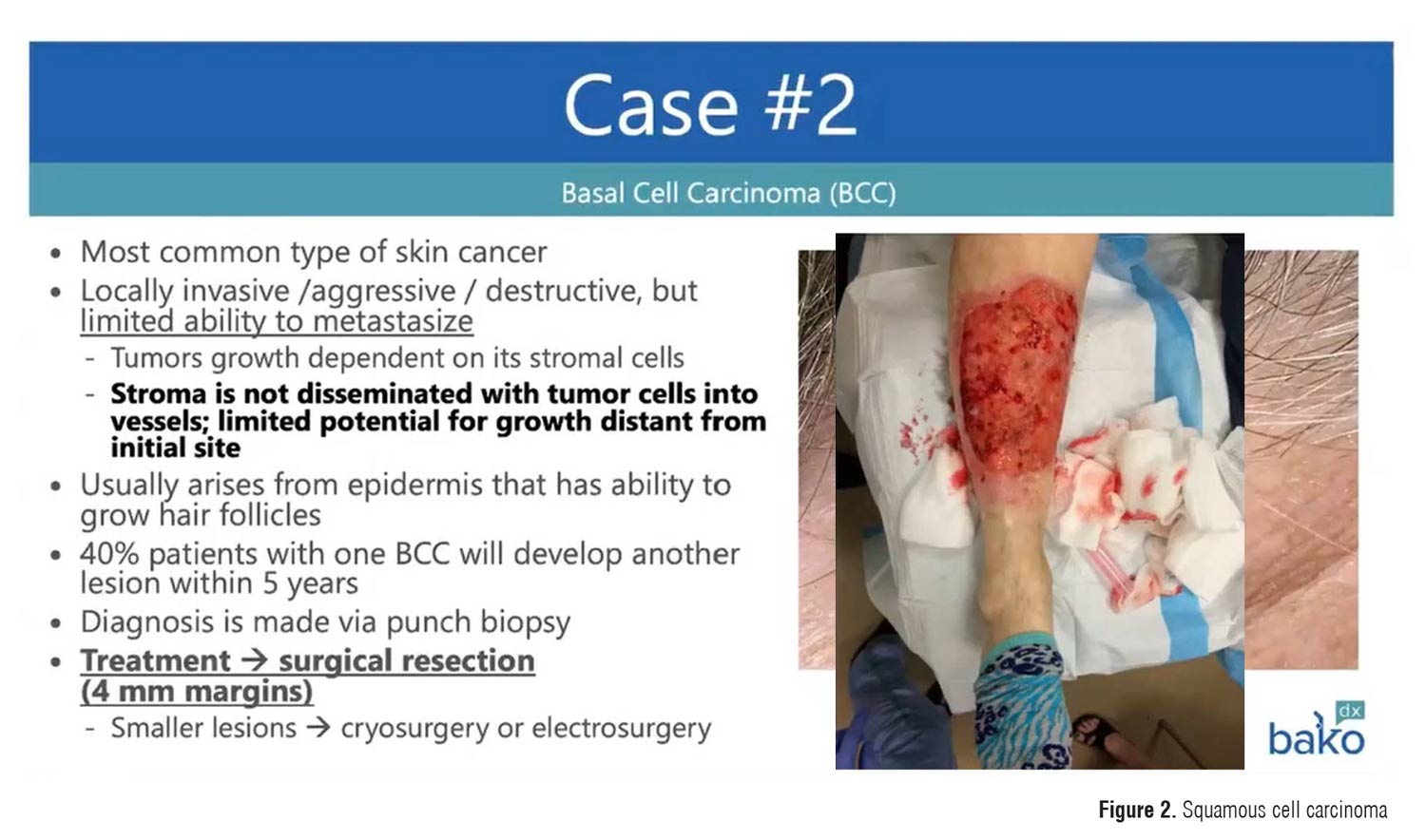
- A basal cell carcinoma (Figure 2) on the lower leg misdiagnosed and treated for years as a venous stasis ulcer.
- A squamous cell carcinoma on the toe of a patient with diabetes and neuropathy initially managed as a typical diabetic foot ulcer.
- A squamous cell carcinoma arising in a chronic burn scar on the lower leg, where the history of the burn injury should have prompted earlier suspicion for malignancy.
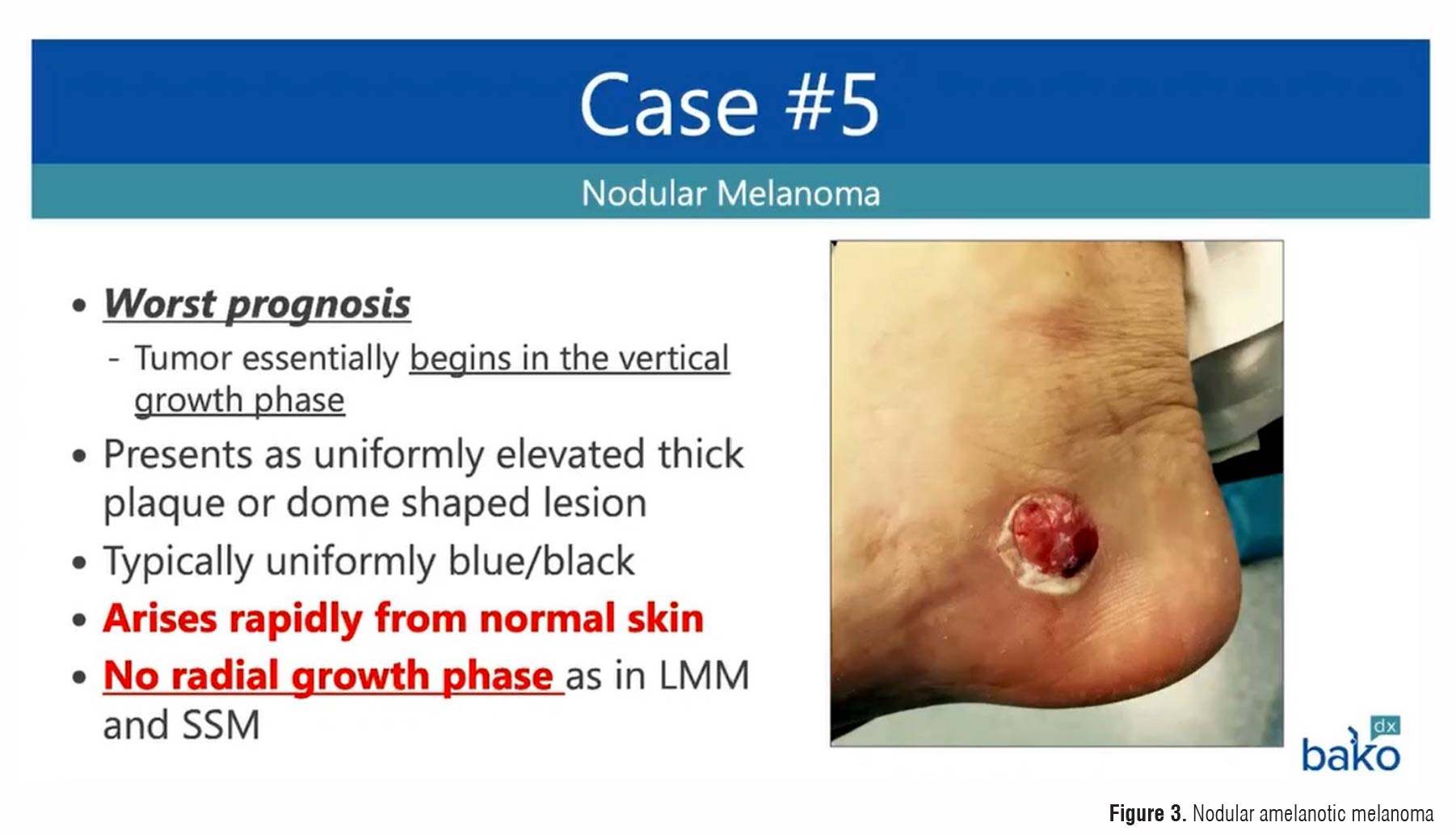
- A nodular amelanotic melanoma (Figure 3) on the medial calcaneus initially thought to be related to an insect bite or a benign skin tumor.
- Bullous pemphigoid, an autoimmune blistering disease, initially presenting as a seemingly friction-induced blister.
- Acral spongiotic dermatitis (numular eczema) misdiagnosed and treated as tinea pedis due to a moccasin-like distribution of erythema and scaling.
- Pyoderma gangrenosum, a rare inflammatory skin condition, initially mistaken for an infected lesion or spider bite.
4. What is the significance of considering malignant diagnoses like squamous cell carcinoma and melanoma? Squamous cell carcinoma (SCC) and melanoma are serious forms of skin cancer that can occur on the feet and ankles. SCC has the potential to metastasize, particularly if it arises in areas of chronic inflammation, burns, or in immunocompromised individuals. Early diagnosis and surgical excision with appropriate margins are crucial for preventing local destruction and distant spread. Melanoma, especially nodular melanoma, can be aggressive and has a poorer prognosis if not diagnosed and treated early. Recognizing the possibility of these malignancies, even when clinical presentation is atypical (eg, amelanotic melanoma resembling a benign nodule), and performing timely biopsies are essential for improving patient outcomes and potentially saving lives. Involving surgical oncology for further evaluation and management is often necessary in such cases.
5. How should a podiatric physician approach a non-healing wound, and when should a biopsy be considered? For non-healing wounds, podiatric physicians should:
- Thoroughly evaluate the patient’s history, including the duration of the wound, previous treatments, associated medical conditions (eg, diabetes, vascular disease), and any history of trauma or prior skin conditions.
- Perform a comprehensive physical examination, paying close attention to the wound’s characteristics (location, size, depth, appearance of the wound bed and surrounding skin) and assessing for signs of infection or underlying vascular insufficiency.
- Consider ordering appropriate diagnostic tests, such as vascular studies (eg, venous duplex for suspected venous ulcers) or cultures if infection is suspected.
- Establish a differential diagnosis, considering not only common causes of foot ulcers but also less frequent conditions, including malignancies and inflammatory dermatoses.
- Have a low threshold for performing a biopsy, especially if the wound does not respond to appropriate treatment within a reasonable timeframe (eg, no significant reduction in size of a non-infected diabetic foot ulcer within 4 weeks). Biopsy should also be considered if the clinical presentation is atypical or suspicious for a non-ulcerative pathology.
6. What are the different types of skin biopsies, and when might each be appropriate?
- Punch biopsy: A small, circular piece of skin is removed using a cylindrical blade. This is useful for sampling a specific area of a lesion and can provide full-thickness samples. A 2–3 mm punch biopsy is useful for initial evaluation of various skin conditions.
- Shave biopsy: A thin layer of skin is shaved off the surface. This is suitable for superficial lesions and can be diagnostic for certain conditions. A deep shave biopsy with a dermablade might be considered for a lesion like a suspected pyogenic granuloma or for initial sampling of a lesion where the depth isn’t the primary concern initially.
- Excisional biopsy: The entire lesion is removed along with a margin of surrounding normal skin. This is often the preferred method for suspected melanomas to ensure complete removal and accurate staging based on depth. A narrow-margin excisional biopsy is generally recommended for suspected melanomas.
- Incisional biopsy: Only a portion of a larger lesion is removed. This is useful when the lesion is too large to excise entirely or when multiple areas need to be sampled.
The choice of biopsy technique depends on the clinical presentation, suspected diagnosis, and location of the lesion. For suspected melanomas, a narrow margin excisional biopsy is generally recommended. For other conditions, punch or shave biopsies may be sufficient for diagnosis.
7. What is direct immunofluorescence (DIF), and when is it a useful diagnostic tool? DIF is a specialized laboratory technique used to detect the deposition of antibodies and complement proteins in skin tissue. It is particularly useful in diagnosing autoimmune blistering diseases, such as bullous pemphigoid, and certain connective tissue disorders. In the case presented, DIF was useful in identifying the IgG antibody deposition along the epidermal-dermal junction, confirming the diagnosis of bullous pemphigoid, which would not have been possible with standard histopathological staining alone. When autoimmune blistering conditions are suspected based on clinical presentation, a biopsy sample should be sent in Zeus or Michael’s medium (in addition to formalin-fixed tissue) to allow for DIF testing.
8. What is the importance of interprofessional collaboration in managing complex dermatological conditions of the foot and ankle? Interprofessional collaboration is vital in managing complex dermatological conditions. When a podiatric physician diagnoses or suspects conditions like squamous cell carcinoma, melanoma, bullous pemphigoid, or pyoderma gangrenosum, involving specialists such as dermatologists, surgical oncologists, rheumatologists, and wound care specialists is crucial. Surgical oncologists are essential for the definitive surgical management of skin cancers and for evaluating the risk of metastasis. Dermatologists can provide expertise in diagnosing and managing a wide range of skin conditions, including complex or rare cases. Rheumatologists are necessary for the systemic management of autoimmune diseases like bullous pemphigoid. A collaborative approach ensures that patients receive comprehensive care, accurate diagnosis, appropriate treatment, and optimal outcomes. It is critically important to refer patients with diagnosed squamous cell carcinoma or melanoma to surgical oncology and involving rheumatology in the management of bullous pemphigoid.
Leland Jaffe, DPM. FACFAS, CWSP, is currently a Podiatric Physician with the Endeavor Health Medical Group in Chicago, IL. Before this appointment, he served as an Associate Professor with the Scholl College of Podiatric Medicine at Rosalind Franklin University.
This article is a summary of Dr. Jaffe’s presentation from the 2025 No-Nonsense Seminar held March 7–9. To view the full presentation with questions and answers—and see the agenda for the 3-day program, visit https://nononsense2025.lerexpo.com. Continuing education credits are available for this and many of the lerEXPO programs.





