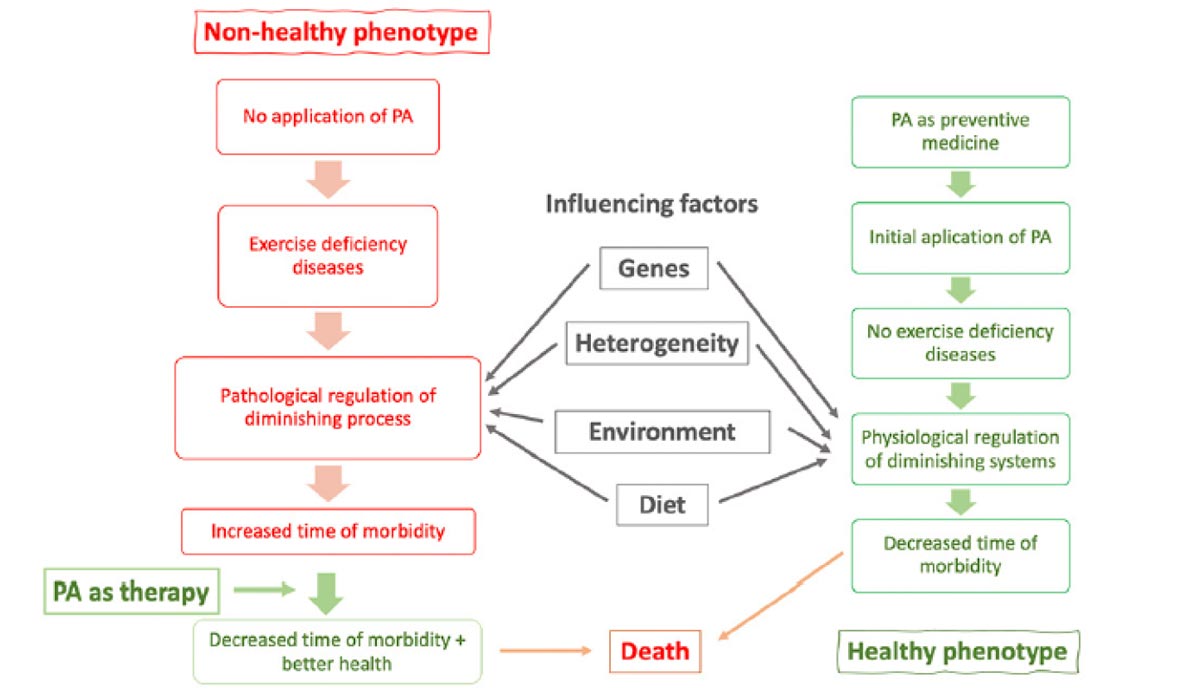
Figure 1. The left-hand side shows the application of PA as a therapeutic agent to pathologies that have developed because of a lack of exercise. This side reflects pathological, not physiological changes. The effects of these pathologies can be ameliorated by PA. The right-hand side shows the application of PA as preventative medicine and the maintenance of effective but diminishing physiological function. This side is investigated by the science of physiology and ageing. Both sides are in constant decremental change because of the inherent ageing process. The center shows major effectors of both pathological and physiological processes. PA = physical activity.
The human aging process is universal, ubiquitous, and inevitable. Every physiological function is being continuously diminished. Aging and a sedentary lifestyle are associated with declines in muscle function and cardiorespiratory fitness, resulting in an impaired capacity to perform daily activities and maintain independent functioning. However, in the presence of adequate exercise/physical activity (PA) these changes in muscular and aerobic capacity with age are substantially attenuated. Additionally, both structured exercise and overall PA play important roles as preventive strategies for many chronic diseases, including cardiovascular disease, stroke, diabetes, osteoporosis, and obesity; improvement of mobility, mental health, and quality of life; and reduction in mortality, among other benefits. Notably, exercise intervention programs improve the hallmarks of frailty (low body mass, strength, mobility, PA level, energy) and cognition, thus optimizing functional capacity during aging. In these pathological conditions, exercise is used as a therapeutic agent and follows the precepts of identifying the cause of a disease and then using an agent in an evidence-based dose to eliminate or moderate the disease.
Prescription of PA/structured exercise should therefore be based on the intended outcome (eg, primary prevention, improvement in fitness or functional status, or disease treatment), and individualized, adjusted, and controlled like any other medical treatment. In addition, in line with other therapeutic agents, exercise shows a dose-response effect and can be individualized using different modalities, volumes, and/or intensities as appropriate to the health state or medical condition.
Importantly, exercise therapy is often directed at several physiological systems simultaneously, rather than targeted to a single outcome as is generally the case with pharmacological approaches to disease management. There are diseases for which exercise is an alternative to pharmacological treatment (such as depression), thus contributing to the goal of deprescribing of potentially inappropriate medications (PIMS). There are other conditions where no effective drug therapy is currently available (such as sarcopenia or dementia), where exercise may serve a primary role in prevention and treatment. Therefore, this consensus statement provides an evidence-based rationale for using exercise and PA for health promotion and disease prevention and treatment in older adults. Exercise prescription is discussed in terms of the specific modalities and doses that have been studied in randomized controlled trials for their effectiveness in attenuating physiological changes of aging, disease prevention, and/or improvement of older adults with chronic disease and disability. Recommendations are proposed to bridge gaps in the current literature and to optimize the use of exercise/PA both as a preventive medicine and as a therapeutic agent.
Physical activity and exercise for health promotion, disease prevention, and treatment in older adults

a. Original Borg Scale of Perceived Exertion from 6 (easy) to 20 (maximal); b. Intensity is increased by decreasing the base of support [e.g., progressing from standing on two feet while holding on to the back of a chair to standing on one foot with no hand support); by decreasing other sensory input (e.g., closing eyes or standing on a foam pillow); by perturbing the centre of mass (e.g., holding a heavy object out to one side while maintaining balance, standing on one leg while lifting the other leg out behind the body, or leaning forward as far as possible without falling or moving feet); or by dual-tasking (adding a secondary cognitive [e.g., naming animals] or physical (e.g. juggling) task while tandem walking].
The world population is aging, and adults ≥ 65 years old are projected to double in number to ~ 1.5 billion in 2050. Due to a concurrent increase in life expectancy, people ≥ 80 years of age are projected to triple in number between 2019 and 2050 to 426 million. Population aging impacts many sectors, including healthcare, quality of life (social), retirement, and caregiving, and most importantly, is associated with an age-related burden of non-communicable chronic diseases and disability. The human aging process is universal, ubiquitous, inevitable, and decremental. Every physiological function is being continuously diminished. At around 20–30 years of age humans have acquired all the physiological development that they will attain. From that stage the aging process commences, although the rate of change is heterogeneous. This process will continue up to 6 or 7 decades ending in death. There is a range between 2 distinct phenotypes of aging, shaped by patterns of living—experiences and behaviors, and in particular by the presence or absence of ‘healthful’ levels of PA and exercise (ie, a sedentary lifestyle). In this consensus, the terms ‘physical activity’ and ‘exercise’ should be interpreted as follows: PA is any bodily movement produced by skeletal muscles that significantly increases energy expenditure. The intensity and duration of PA can vary substantially. Exercise is a subcategory of PA that is planned, structured, and repetitive, in which bodily movements are performed with or without the explicit intent of improving or maintaining of 1 or more components of physical fitness (ie, aerobic capacity, muscle strength power, and endurance, balance, coordination, and flexibility).
Table 1 details the consensus panel’s exercise recommendations for optimal aging and maintenance of functional capacities in older adults. (See also page 13, Major Geriatric Syndromes for Which Exercise May Be Beneficial as a Preventive.)
Of particular import for LER readers:
Gait training recommendations. Several trials investigating the effects of exercise interventions on gait ability (velocity and stability) in older individuals with frailty have yielded conflicting results. Whereas some studies showed improvements in gait ability after the physical training period, others found no improvement. Interestingly, the bulk of studies demonstrating improvements in gait ability utilized multicomponent exercise programs, while others used only resistance exercises or a combination of aerobic training and yoga. Gait ability is a strong predictor of survival in older adults and its maintenance should be prioritized in the oldest-old. Aerobic exercises such as walking with changes in pace and direction, treadmill walking, step-ups, and stair climbing, among others, are valuable modalities to achieve aerobic fitness adaptations and gait and mobility improvements. Weight bearing aerobic activities that simulate real-life activities are preferable whenever possible. For those patients with severe arthritis or balance impairment, aquatic exercise, seated steppers, or recumbent cycles may be more tolerable alternatives. Generally, however, if someone cannot support their body weight independently, the initial priority should be resistance (strength and power) training, as well as balance training, before moving to ambulation and other forms of weight bearing aerobic exercise. The duration of the exercise component may start at 5–10 minutes (or less) during the first weeks of training and progress to 20–30 minutes in the long term. The intensity of this exercise component is generally proportional to heart rate and can be increased from moderate to vigorous as fitness and confidence improve. If the heart rate can no longer function as an accurate measure of exercise intensity due to arrhythmias, beta-blockers, or functioning pacemakers, clinicians can use perceived exertion scales instead. If cognitive impairment precludes the use of subjective perceived exertion, observer-rated perceived exertion (respiratory rate, ability to talk, sweating, or facial expression) can be substituted.
Effects of PA/exercise interventions on falls Multicomponent exercise programs including combinations of resistance training, balance and/or gait retraining; less commonly, resistance exercise alone, or an alternative exercise intervention such as Tai Chi or dance programs have been shown to reduce falls in older adults. Aerobic training alone, by contrast, has been shown to increase falls and fracture risk. Based on the evidence that such multicomponent exercise interventions are more effective in improving most, if not all, of the frailty syndrome hallmarks (ie, poor balance, reduced muscle strength, poor gait ability, and increased incidence of falls), it is the recommended strategy for this condition. Current evidence, however, on reducing falls with physical training among community-dwelling older adults with cognitive impairment (ie, any stage of Alzheimer’s disease and related dementias, or mild cognitive impairment) is insufficient at this time to inform evidence-based recommendations or treatment decisions for clinical practice.
Conclusions
Insufficient PA/exercise and excess sedentary behaviors are potent risk factors for all-cause and cardiovascular mortality, obesity, sarcopenia, frailty, and disability, among other chronic diseases associated with aging. Being physically active and having a healthy diet (coupled with no smoking and moderate alcohol consumption and the maintenance of appropriate body mass) are integral to maintaining health and well-being at all ages. Exercise and PA offer clinical benefits across a wide range of diseases and disabilities with no upper age limit. An appropriate exercise prescription should be included in all healthcare recommendations in the effort to enhance functional independence, psychological well-being, and quality of life through the promotion of exercise for all older adults, whether fit or frail, of any age. PA (including structured exercise participation) influences key drivers of aging even in the oldest-old, including chronic inflammation, mitochondrial dysfunction, myokine release, autophagy, oxidative damage, and insulin-like growth factor signaling. Exercise and PA improve physical function and quality of life, and reduce the burden of non-communicable chronic diseases and premature overall mortality including cause-specific mortality from cardiovascular disease, cancer, and chronic lower respiratory tract diseases. The beneficial effects of exercise are global (ie, acting at both the physiological multisystem and functional capacity level). Exercise interventions are currently more useful than pharmacological interventions that target single systems (eg, inflammation or anabolic hormones) for managing frailty. Declines in muscle function and cardiorespiratory fitness with aging result in impaired ability to perform daily activities and maintain Independence. Accordingly, the treatment of frailty should be focused on improvement in overall functionality, complementary to the diagnosis and treatment of specific diseases. Exercise is medicine, and the prescription of PA/structured exercise should therefore be based on the intended outcome (eg, primary prevention, improvement in fitness or functional status, or disease treatment), and should be individualized, and controlled like any other medical treatment. The prescription of exercise for health-related outcomes must consider not only dose-response relationships with volume and intensity, but also modality-specific adaptations which are requisite for certain outcomes to be achieved. Since most patients will present with more than 1 disease, an efficient prescription to optimize both safety and efficacy is mandatory as described in this consensus statement. Importantly, beyond its practical benefits, long-term physical exercise results in less harm among older adults than maintaining usual activity levels or usual care, independent of participants’ age, physical function, or cognition status at baseline. Considering the accumulated evidence of the benefits of exercise in frail older adults over many decades, it is not justifiable to not prescribe physical exercise to these individuals, and 1 of the main challenges for the future is to integrate exercise programs as a mandatory part of the care of pre-frail/frail older patients in all hospital, outpatient, and aged care settings.
This article has been excerpted from Izquierdo M, Merchant RA, Morley JE, et al. International Exercise Recommendations in Older Adults (ICFSR): Expert Consensus Guidelines,” from the Journal of Nutrition, Health & Aging. 2021;25(7):824-853. Editing has occurred, including the renumbering of tables, and references have been removed for brevity. Use is per CC BY.





