
iStockphoto.com 471781867
The ankle is a frequent site of arthropathy in patients with hemophilia, but orthotic devices and orthopedic shoes can help relieve this pain. New research suggests that carbon fiber ankle foot orthoses and orthopedic shoes also appear to have gait-related advantages in this patient population.
By David Oleson, PT, PCS; Katherine Stribling, PT, DPT, PCS; Jamie Beckwith, PT, DPT; Laura Fox, PT, DPT, PCS; Felicity Case, PT, DPT, PCS; Nancy Durben, MSPT, PCS; and Michael Recht, MD, PhD
Hemophilia is a genetic disorder characterized by less than normal amounts of coagulation factors VIII (FVIII) and IX (FIX). The clinical features of FVIII and FIX deficiencies are identical. Persons with less than 1% FVIII or FIX are said to have severe hemophilia and most commonly bleed into their joints, causing synovial inflammation, iron deposition, cartilage destruction, and bony changes.1,2 These arthritic changes are painful and alter movement.1 In boys with arthropathy, reported changes from controls include increases in swing time, stance time, double support, single support, and base of support. Decreases from controls include step length and normalized velocity.2
Treatment of hemophilia primarily involves replacement of the missing factors by infusion. The standard of care is to infuse prophylactically to prevent bleeding. Despite prophylaxis, arthropathy remains common.1,3 In particular, the ankle is a frequent site of bleeding in hemophilia.3 Pain relief in this population is elusive, and promotion of activity and participation in daily life and desired activities are common physical therapy goals.4
In our treatment center, the Hemophilia Center at Oregon Health & Science University in Portland, we have investigated ankle arthropathy from multiple perspectives. We have studied the effect of two different types of bracing on gait parameters and pain relief, as well as the effect of orthotic device use on pain, activity, and participation of persons with ankle arthropathy.
Bracing, gait, and ankle pain

Figure 1. Summary of mean (± 1 standard error) pain scores reported by patients wearing shoes only, a fracture boot, or a carbon fiber AFO. *Indicates difference at p < .05 level, pairwise comparison with multiple testing adjustment.
Bracing to relieve ankle pain from hemophilic arthropathy has long been used, but the effects of these devices on gait had never been analyzed. In our study, we chose to compare the gait parameters associated with a carbon fiber floor reaction ankle foot orthosis (AFO) and a fracture boot.5
Fracture boots and AFOs both restrict ankle range of motion to relieve pain during gait caused by joint destruction and loss of joint space. Fracture boots absorb weightbearing through their rigid walls and mimic normal propulsion during walking with a curved sole.6,7 AFOs relieve pain similarly. For patients with hemophilia and ankle arthropathy, they are typically custom fabricated of thermoplastic material, are rigid, and are worn inside the shoe; this typically requires the patient to wear a larger shoe size than usual. In addition, both types of devices can be hot and uncomfortable to wear.7 In our clinical experience, people with hemophilia and ankle arthropathy shun the use of these types of devices.
For our study, we used a fracture boot with a pneumatic liner and a carbon fiber AFO.
Carbon fiber floor reaction AFOs are lighter than fracture boots but are equally able to absorb the forces of walking. They have a single strut on the lateral side. Unlike typical AFOs, they do not require a larger shoe, are easy to put on and take off, and are not hot to wear. These braces were much more acceptable to our patients during early trials.
We studied the gait parameters of 17 people with severe hemophilia and unilateral ankle arthropathy using a 14-foot electronic sensor-embedded walkway. Participants walked at self-determined speed four times in each of three conditions: with shoes bilaterally and no brace, with a shoe on the unaffected foot and a fracture boot on the affected foot, and with a shoe on the unaffected foot and a carbon fiber AFO and shoe on the affected foot.
Pain was assessed using an 11-point (0-10) numerical rating8 scale and was assessed before and after each walking trial. Pain scores were divided into three categories (0 = no pain, .5 – 2 = moderate pain, > 2 = severe pain).
Findings
Pain relief and gait-related effects of bracing the painful ankle were studied on both the braced and nonbraced sides. Each participant served as their own control. Pain was relieved significantly (p < .05) with both devices compared with the shoes-only (no brace) condition. There was no difference in pain reduction between the fracture boot and carbon fiber AFO treatments (p = .999). (Figure 1.)
Compared with the nonbraced condition, we found use of a fracture boot on the involved ankle decreased the number of steps taken per unit of time (cadence) and increased step time (time needed for one foot-to-next-foot contact), swing time (time the foot is in the air), and cycle time (time needed between one foot contact and the next foot contact of the same foot). (Figure 2.)
Step time, swing time, and cycle time parameters tell us about the dynamic effects of bracing. The treatment effects associated with these gait parameters may be due to the differences in size and weight of the two braces. This may also be responsible for the changes noted in cadence, as the heavier fracture boot may require the limb to move more slowly, so fewer steps per minute would be generated.
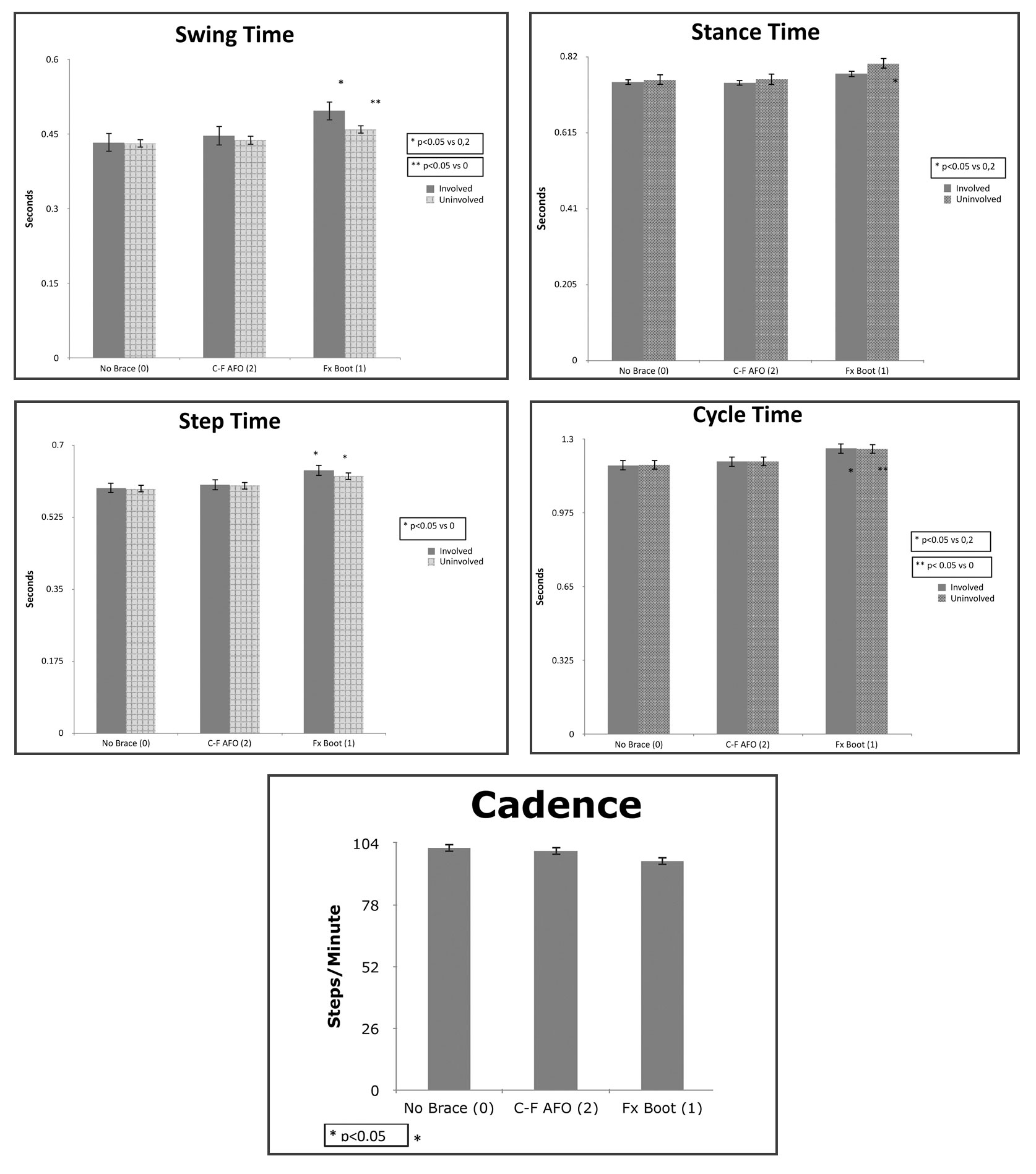
Figure 2: Summary of mean (± 1 standard error) gait parameters associated with three treatment conditions (no brace [0], fracture boot [1], and carbon fiber AFO [2]). *, ** Indicate between-group differences at p < .05 level, pairwise comparison with multiple testing adjustment.
A fracture boot is not only heavier but also longer than a shoe alone, and therefore longer and heavier than a shoe with a carbon fiber AFO. Advancing of the limb wearing a fracture boot may require greater energy and may explain the increases in swing, cycle, and step times noted when compared with the no-brace condition. This added weight and length of the fracture boot may also explain the differences noted in swing time of the uninvolved limb when a fracture boot is worn on the involved limb.
There were no significant differences for any of the gait parameters between the nonbraced (shoes-only) condition and the carbon fiber AFO condition. This finding, coupled with the significant differences observed between the fracture boot and the carbon fiber AFO, suggest the AFO helps to preserve a more typical and efficient gait pattern in patients with hemophilia and ankle arthropathy.
The implications of this study involve better management of pain relief, preservation of gait, and increase in participation. Our results indicate both devices were equally effective in relieving pain.
What are the effects of these devices on gait? Observation and discussion with our patients greatly informed this question. People who had tried fracture boots for their ankle pain said they felt unstable, possibly because of the boot’s different height and weight, and chose not to use a fracture boot despite good pain relief, while those who had tried carbon fiber AFOs uniformly liked and accepted them. Our results suggest using a fracture boot on a painful ankle negatively affected the dynamic aspects of gait on both the braced side and the nonbraced side. The carbon fiber AFO, however, did not affect gait parameters and relieved pain equally. Subjective comments of our study participants indicated a much greater acceptance of the carbon fiber AFO than the fracture boot.

Can we use this information to improve participation? Of our patients, those who are currently using a carbon fiber AFO are wearing it on an as-needed basis. Some wear it at work only, some wear it when they know they will be doing a specific activity that necessitates more walking than usual. Anecdotally, they all report they can do what they need to do longer and with less pain when using a carbon fiber AFO compared with shoes only. Of the patients in our study, only one is using a carbon fiber AFO and uses it as needed, and none are using a fracture boot.
Bracing is not for everyone, and personal preference must be respected. In our experience, persons with hemophilia tend to be resistant to bracing, and may not be comfortable even with a brace that is lighter, cooler, and lower-profile than a typical device.
Orthotic use
Joint damage from hemarthroses result in painful bony changes that can be exacerbated during weightbearing. Because of this, foot orthoses have long been a component of treating patients with hemophilic arthropathy of the ankle.6,9,10
Some studies have addressed the impairments and activity limitations associated with hemophilia, but only a few have looked at participation, and most have focused on children and adolescents.11-17
One study18 used 3D gait analysis and the Revised Foot Function Index (FFI-R)19,20 to compare the effect on hemophilic ankle arthropathy of custom-fabricated orthopedic shoes and custom-fabricated orthopedic inserts. The FFI-R asks questions about foot function in five domains: pain, stiffness, difficulty, activity limitation, and social and emotional outcomes. In this study, FFI-R scores suggest both orthopedic shoes and orthopedic inserts provide pain relief. The gait analysis results showed the orthopedic shoes were associated with improved propulsive function at the ankle, while the orthopedic inserts had only a limited effect on gait.18
To study the effects of orthotic use on participation, we surveyed 16 men with moderate and severe factors VIII and IX deficiencies and ankle pain using the Foot Function Index (FFI).21 The FFI is a Likert-type scale that includes questions related to pain, disability, and activity level.22,23 We also asked participants subsequent questions about how satisfied they were with their activity with and without orthotics.21 Comparison of mean scores showed no differences in pain levels but significant improvements in activity (disability on the FFI) and participation (subsequent questions) with orthotic device use compared with no orthotic use.21
These results prompted an ongoing qualitative study to identify common themes and perspectives related to ankle function and orthotic device use. Study participants also completed the FFI-R in an attempt to look at associations between qualitative findings and objective data. The FFI-R was chosen due to its comprehensive range of domains.22,23
In this ongoing study,24 17 interviews involving men with moderate to severe factor VIII and IX deficiencies have been transcribed and coded. To date, themes identified include impact of pain on daily life, individualization of management, self-advocacy, unique psychosocial challenges, the role of learning from others with hemophilia, and the desire for respectful acknowledgment by healthcare professionals of their experience dealing with their bleeding disorder. Interviews are still being conducted.
Pilot data from the FFI-R show a positive trend in participation (eg, a lower score for activity limitation) for orthotic device users. Data trends also suggest fewer social issues among those using orthotic devices. There were no trends associated with age. However, this study is ongoing; data are still being collected and analyzed, and should not be taken as conclusive at this point.24
Summary
Separate studies show ankle pain can be relieved with bracing,5 as well as with foot orthoses and orthopedic shoes.18 The same studies suggest carbon fiber AFOs do not alter the gait cycle, whereas fracture boots do,5 and that orthopedic shoes are associated with improved gait while foot orthoses have a limited effect.18
The FFI-R appears to be a sensitive tool to evaluate the effects of foot orthoses and participation in persons with hemophilia.18,24 Qualitative data suggest individuality and respect for personal knowledge and experience need to be taken into account in the management of hemophilic ankle arthropathy.24
David Oleson, PT, PCS, and Nancy Durben, MSPT, PCS, are physical therapists at The Hemophilia Center at Oregon Health & Science University (OHSU) in Portland. Katherine Stribling, PT, DPT, PCS; Jamie Beckwith, PT, DPT; Laura Fox, PT, DPT, PCS; and Felicity Case, PT, DPT, PCS, contributed to this paper as pediatric physical therapy residents at OHSU. Stribling and Beckwith are currently participating in hemophilia research at OHSU as coinvestigators. Michael Recht, MD, PhD, is medical director of The Hemophilia Center at OHSU.
- Blodel C, Haxaire C, Kalliolias G, et al. Blood-induced arthropathy in hemophilia: mechanisms and heterogeneity. Semin Thromb Hemost 2015;41(8):832-837.
- Thorpe DE, Dusing SC, Moore CG. Repeatability of temperospatial gait measures in children using the Gaitrite electronic walkway. Arch Phys Med Rehabil 2005;86(12):2342-2346.
- Wyseure T, Mosnier LO, von Drygalskia A. Advances and challenges in hemophilic arthropathy. Semin Hematol 2016;53(1):10-19.
- Witkop M, Neff A, Buckner T, et al. Self-reported prevalence, description and management of pain in adults with haemophilia: methods, demographics and results from the Pain, Functional Impairment and Quality of life (P-FiQ) study. Haemophilia 2017;23(4):556-565.
- Oleson D, Fox L, Nguyen T, et al. A comparison of two types of ankle supports in men with haemophilia and unilateral ankle pain from arthropathy. 2017;23(3):444-448.
- Querol F, Aznar J, Haya S, et al. Orthoses in haemophilia. Haemophilia 2002;8(3):407-412.
- DiLiberto F, Baumhauer J, Wilding G, Bawoczenski D. Alterations in plantar pressure with different walking boot designs. Foot Ankle Int 2007;28(1):55-60.
- Ferriera-Valente MA, Pail-Ribeiro JL, Jensen MP. Validity of four pain intensity rating scales. Pain 2011;152(10):2399-2404.
- Heim M, Steinbach T. Update on the use of orthotics in hemophilia. Orthop Rev 1988;17(10):975-978.
- Heijnen L, Buzzard BB. The role of physical therapy and rehabilitation in the management of hemophilia in developing countries. Semin Thromb Hemos 2005;31(5):513-517.
- Buxbaum NP, Ponce M, Saidi P, Michaels LA. Psychosocial correlates of physical activity in adolescents with haemopilia. Haemophilia 2010;16(4):656-661.
- Groen WG, Takken T, van der Net J, Helders PJM, et al. Habitual physical activity in Dutch children and adolescents with haemophilia. Haemophilia 2011;17(5):e906-e912.
- Ross C, Goldenberg NA, Hund D, Manco-Johnson MJ. Athletic participation in severe hemophilia: bleeding and joint outcomes in children on prophylaxis. Pediatrics 2009;124(5):1267-1272.
- Sherlock E, O’Donnell JS, White B, Blake C. Physical activity levels and participation in sport in Irish people with haemophilia. Haemophilia 2010;16(1):e202-e209.
- Czepa D, Von Mackensen S, Hilberg T. Haemophilia & exercise project (HEP): Subjective and objective physical performance in adult haemophilia patients-results of a cross-sectional study. Haemophilia 2012;18(1):80-85.
- Groen W, van der Net J, Bos K, et al. Joint health and functional ability in children with haemophilia who receive intensive replacement therapy. Haemophilia 2011;17(5):783-790.
- Hassan J, van der Net J, Helders PJ, et al. Six-minute walk test in children with chronic conditions. Br J Sports Med 2010;44(4):270-274.
- Lobet S, Detrembleur C, Lantin A-C, et al. Functional impact of custom-made foot orthoses in patients with haemophilic ankle arthropathy. Haemophilia 2012;18(3):e227-e235
- Budiman-Mak E, Conrad KJ, et al. A review of the foot function index and the foot function index – revised. J Foot Ankle Res 2013;6:5.
- Riskowski J, Hagedorn T, Hannan M. Measures of foot function, foot health and foot pain: American Academy of Orthopedic Surgeons Lower Limb Outcomes Assessment: Foot and Ankle Module (AAOS-FAM), Bristol Foot Score (BFS), Revised Foot Function Index (FFI-R), Foot Health Status Questionnaire (FHSQ), Manchester Foot Pain and Disability Index (MFPDI), Podiatric Health Questionnaire (PHQ), and Rowan Foot Pain Assessment (ROFPAQ). Arthritis Care Res 2011;63(S11):S229-S239.
- Case F, Oleson D. Effect of orthotic use on the International Classification of Functioning, Disease and Health (ICF) Model in People with Hemophilia. Paper in progress.
- SooHoo NF, Samimi DB, Vyas RM, Botzler T. Evaluation of the validity of the foot function index in measuring outcomes in patients with foot and ankle disorders. Foot Ankle Int 2006;27(1):38-42.
- Agel J, Beskin JL, Brage M, et al. Reliability of the foot function index: A report of the AOFAS outcomes committee. Foot Ankle Int 2005;26(11):962-967.
- Stribling K, Beckwith J, Durben N, et al. Attitudes and perspectives on ankle function in people with hemophilia. Study in process.





