 By Nicola O’Malley, Susan Coote, Fiona McCullough Staunton, Eileen O’Connor, and Amanda M. Clifford
By Nicola O’Malley, Susan Coote, Fiona McCullough Staunton, Eileen O’Connor, and Amanda M. Clifford
Research has shown that more than half of people with multiple sclerosis and Parkinson’s disease will fall within a 3- or 6-month period, respectively, while nearly 75% of stroke survivors fall within a year of the stroke occurring.
Clinical trials evaluating the effectiveness of falls prevention interventions for people with multiple sclerosis (MS), Parkinson’s disease (PD), and stroke measure heterogeneous outcomes, often omitting outcomes that are meaningful to patients. Fall events can have detrimental consequences for individuals, including physical injury, reduced psychosocial wellbeing, and increased dependence. On a societal level, falls result in substantial healthcare utilization and increased acute and long-term care needs. The aim of this study was to develop a consensus-based core outcome set (COS) for evaluating mixed-diagnosis falls prevention interventions for this population in non-acute and community settings.
Methods
Previously published research undertaken by the team, including a qualitative study with 20 patients and a review of the literature, were used to derive a long list of potential outcomes. A multi-stakeholder, consensus meeting was conducted to agree upon the final COS and to provide a recommendation for a single outcome measure for each outcome in the COS.
Results
Forty-eight participants were recruited across 4 stakeholder groups (researchers, patients, clinicians, and service-planners/policymakers). Forty-two participants (87.5%) completed all 3 rounds of the surveys, and 62 outcomes were considered for inclusion in the COS. Fifteen participants attended the consensus meeting where they agreed upon the final COS and accompanying measurement instruments: fall incidence, injurious fall incidence, quality of life, falls self-efficacy, fear of falling, activity curtailment due to fear of falling, and cost-effectiveness.
Fall incidence
Recommendation: Fall incidence, reported as falls per person per year, should be assessed in all future mixed-diagnosis falls prevention interventions for people with MS, PD, and stroke. Fall events should be prospectively recorded daily with follow-up by team members at least monthly to reduce recall bias. A fall event should be defined as “an unexpected event in which the participant comes to rest on the ground, floor, or lower level.”
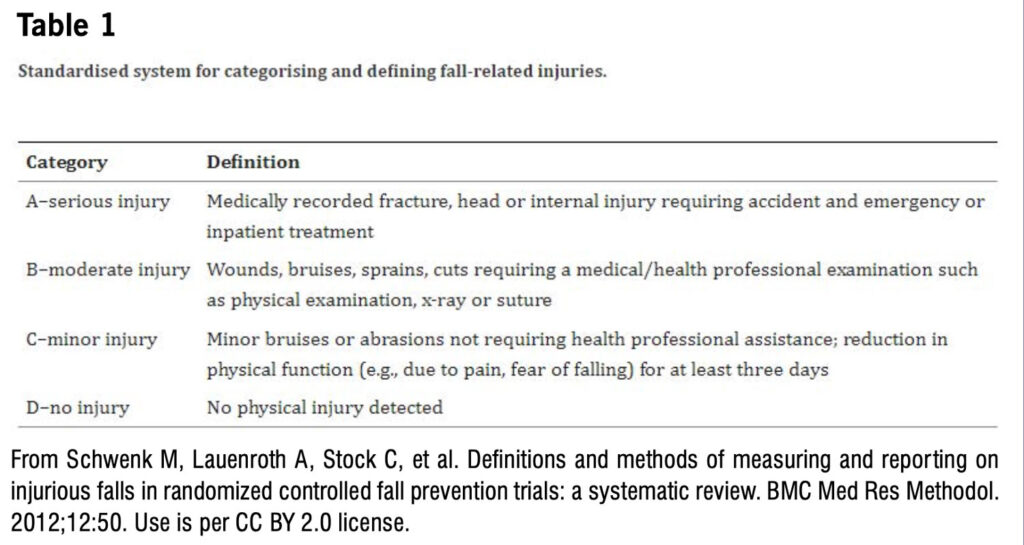
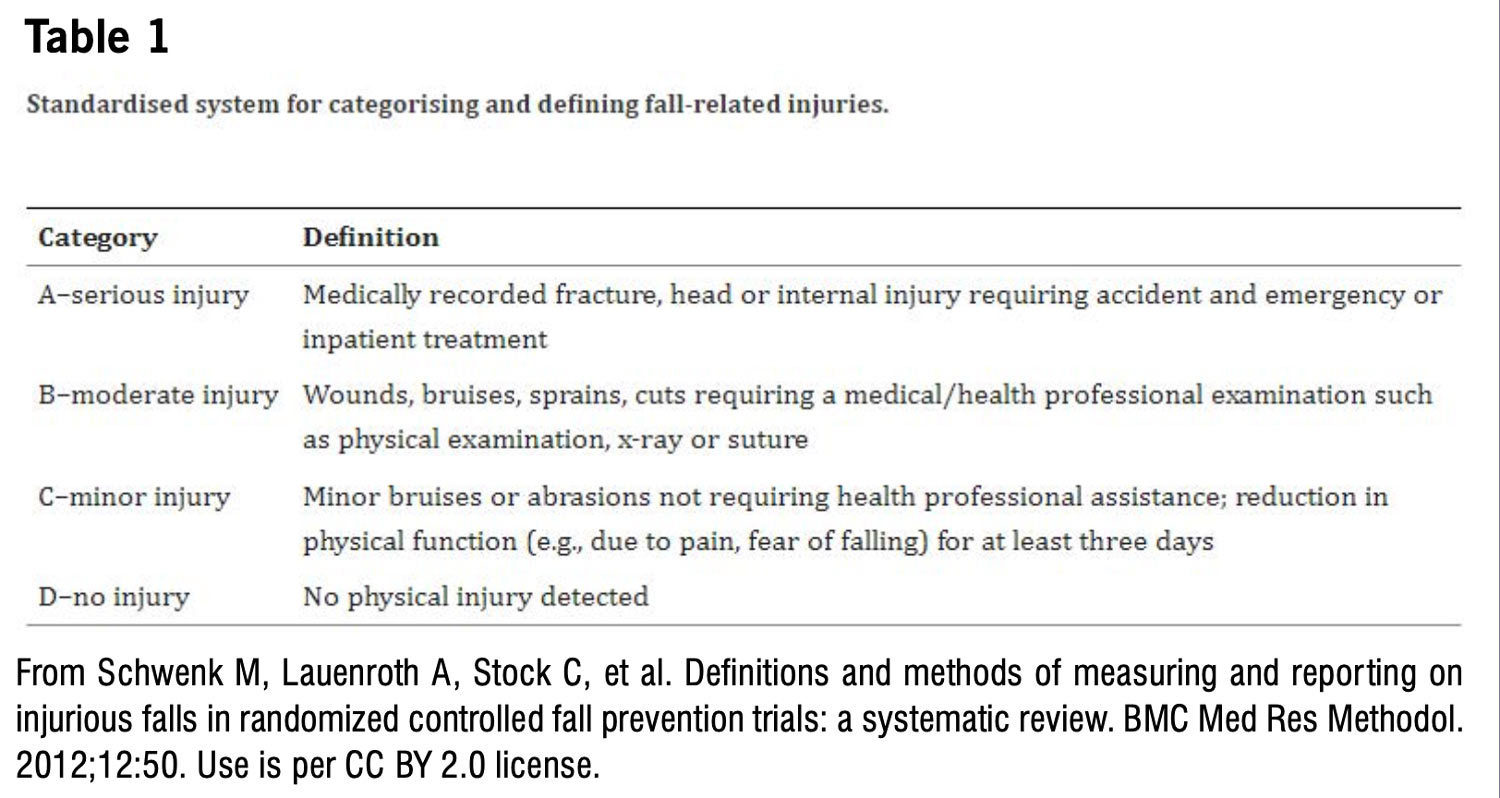
Injurious fall incidence
Recommendation: Injurious fall incidence, reported as injurious falls per person per year, should be assessed in all future mixed-diagnosis falls prevention interventions for people with MS, PD, and stroke. Injurious falls should be prospectively recorded daily with follow-up by team members at least monthly to reduce recall bias. The standardized system for categorizing and defining fall related injuries proposed by Schwenk et al. (2012) should be used (Table 1).
Quality of life
Recommendation: Quality of life should be assessed in all future mixed-diagnosis falls prevention interventions for people with MS, PD, and stroke. This outcome should be measured using the 5-Level EuroQoL-5 (EQ-5D-5L) [www.euroqol.org], which is a generic instrument for describing and valuing health in terms of 5 dimensions: Mobility, Self-Care, Usual Activities, Pain/Discomfort, and Anxiety/Depression.
Falls self-efficacy
Recommendation: Falls self-efficacy should be assessed in all future mixed-diagnosis falls prevention interventions for people with MS, PD, and stroke. This outcome should be measured using the Falls Efficacy Scale-International (FES-I).
Fear of falling
Recommendation: Fear of falling should be assessed in all future mixed-diagnosis falls prevention interventions for people with MS, PD, and stroke. This outcome should be assessed using the direct question, “Are you afraid of falling?” and 5-point Likert scale: not at all, slightly, moderately, very, or extremely.
Activity curtailment due to fear of falling
Recommendation: Activity curtailment due to fear of falling should be assessed in all future mixed-diagnosis falls prevention interventions for people with MS, PD, and stroke. This outcome should be assessed using the direct question, “Do you think that fear of falling has made you cut down on any activities that you used to do?” with the following response options: yes, no, don’t know, or refused.
Cost-effectiveness
Recommendation: Cost-effectiveness should be assessed in all future mixed-diagnosis falls prevention interventions for people with MS, PD, and stroke. Researchers should consult with a health economist to determine the most appropriate way to calculate cost-effectiveness of an intervention.
 Discussion
Discussion
The study authors developed a COS of 7 outcomes for mixed-diagnosis falls prevention interventions for people with MS, PD, and stroke: fall incidence, injurious fall incidence, quality of life, falls self-efficacy, fear of falling, activity curtailment due to fear of falling, and cost-effectiveness. This represents the minimum that should be measured as many outcomes that were not included in the final COS were still considered very important outcomes by participants depending on the type of intervention involved.
Besides fall incidence, the majority of outcomes included in the final COS are currently infrequently evaluated in relevant research studies. Moreover, despite reaching the highest level of agreement across the overall group (91%) for inclusion in the final COS, activity curtailment due to fear of falling was not assessed in any of the papers in the study authors’ umbrella review.
While the selection of measurement instruments that do not require excessive resource commitment may enhance implementation of the COS, such as those outlined herein, further research is required to determine if they are the most appropriate and suitable outcome measures. This is especially true for the measurement instruments for fear of falling and activity curtailment due to fear of falling, which have not been evaluated psychometrically. Given the small number of response options for the activity curtailment outcome measure, and that a relative degree of activity curtailment may be a protective mechanism for some individuals, exploration of the responsiveness of this suggested measurement instrument should be a priority. Also of note, despite being prioritized as critically important during the survey rounds, the study authors were unable to identify any outcome measure for understanding of personal falls risk factors or falls self-management skills. Consequently, future research should focus on the development and psychometric evaluation of outcome measures for outcomes in the COS, as well as those prioritized during the survey rounds.
Conclusions
This study identified a COS for evaluating the effectiveness of mixed-diagnosis falls prevention interventions for people with MS, PD, and stroke. It is recommended that this COS and accompanying measurement instruments be used in all future trials in this research area so that findings can be combined and compared. It is also recommended that a review of this COS would take place in 4 years to ensure that it reflects advancements in the research field and to decide whether an update is required.
This article has been excerpted from “A core outcome set for evaluating the effectiveness of mixed-diagnosis falls prevention interventions for people with Multiple Sclerosis, Parkinson’s Disease and stroke,” PLoS ONE 18(11): e0294193. https://doi.org/10.1371/journal.pone.0294193. Editing has occurred, including the renumbering or removal of tables, and references have been removed for brevity. Use is per CC BY.






I stopped most of my Parkinson’s disease medications due to severe side effects and I started on herbal treatments from Limitless Herbs Centre , the treatment has made a very huge difference for me. My symptoms including body weakness and Swallowing difficulties disappeared after few months on the treatment. I am getting active again since starting this treatment.