
Photo Credit: Heather Ellicott
Like a good medical exam, a medical bike fit starts before the patient ever gets on the bike. Talking with cycling patients before any assessments can facilitate the diagnostic process.
By Andrea Myers, PT, DPT
Bike fitting is a service that has been offered in bike shops and studios for decades. Bike fitting is also a medical service offered by physicians, physical therapists, chiropractors, and other qualified health care providers. When bike fitting is performed by a properly trained medical practitioner, it can be a valuable tool to diagnose and prevent injuries. At its core, bike fitting is a specialized form of posture and gait analysis. Medical practitioners are uniquely qualified to provide this specialized service to our patients.
A complete bike fit aims to improve a rider’s comfort, efficiency, and aerodynamics on the bike. It may also be used by medical practitioners to diagnose and treat fit-related injuries. Injured runners require running gait analysis for proper evaluation and treatment. Similarly, injured cyclists need cycling gait analysis for complete evaluation and treatment. Walking gait analysis involves biomechanical assessment of two phases: stance phase (closed kinetic chain phase) and swing phase (open kinetic chain phase).1 Complete gait analysis (whether it is walking, running, or cycling) requires an understanding of both normal and abnormal gait mechanics.
Normal Cycling Mechanics and Posture
Cycling gait analysis involves biomechanical assessment of the rider during two phases: propulsion (downstroke) and recovery (upstroke). The propulsion phase occurs just after top dead center (12:00 or 0°/360° crank position) to just before bottom dead center (6:00 or 180° crank position). The recovery phase occurs just after bottom dead center to just before top dead center. The greatest muscle activity occurs in the propulsive phase. The propulsive phase is characterized by high activity in the gluteus maximus, the quadriceps, hamstrings (biceps femoris, semitendinosus, and semimembranosus), and the gastrocnemius. The recovery phase is characterized by activity in the hamstrings, gastrocnemius, anterior tibialis, and rectus femoris. During the recovery phase, the hip, knee, and ankle flexors work primarily to unload the pedal. 2,3
At top dead center (TDC), the hip and knee are at maximal flexion values. The ankle moves from dorsiflexion to plantarflexion, typically achieving peak dorsiflexion at a 50° – 70° crank angle.2 The exact amount of hip and knee flexion at TDC depends on crank length, saddle height, and individual rider physiology. At bottom dead center (BDC), the hip and knee are at minimum flexion values. The ankle is in maximum plantarflexion; the exact amount depends on fore-aft cleat positioning and individual pedaling style. In the recovery phase, the hip and knee flex, and the ankle moves from plantarflexion to dorsiflexion.2,3
Normal cycling posture varies based on cycling discipline and individual riding style. The following discussion is most applicable to road cyclists who use clipless pedals. Other cycling disciplines, such as mountain biking or track, have specialized characteristics that require different fit considerations. A discussion of these characteristics is beyond the scope of this article.
In general, a rider’s cervical spine should be in mid-range extension, thoracic spine in mild flexion, lumbar spine in flexion, and pelvis in anterior rotation.2 There should not be any part of the thoracic or lumbar spine that shows excessive flexion as compared to the other vertebral segments; the rider should have a “flat-back” appearance as a result of the moderate anterior pelvic tilt. The shoulders should be at approximately 90° of flexion and in neutral horizontal abduction/adduction, elbows in mid-range flexion and mild pronation, and wrists in slight flexion. The rider should be in a position of stability and joints should not be at end range.
Cycling is primarily a sagittal plane activity. However, some frontal and transverse plane motion is seen in healthy, well-trained cyclists, and should be considered normal. Tibial internal rotation occurs during the propulsion phase, which is accompanied by pronation. Tibial external rotation occurs during the recovery phase and is accompanied by supination. There should be minimal frontal plane motion of the knee; however, slight medial knee movement begins at TDC and reaches its peak around a 90° crank angle.3 Frontal plane movement of the trunk should be minimal. If excessive frontal plane trunk movement is present, it is possible that the saddle is too high or the saddle is too narrow and not properly supporting the ischial tuberosities. Excessive trunk frontal plane motion may also be a compensation for fatigued hip and knee extensors.
Clinical Bike Fitting Essentials
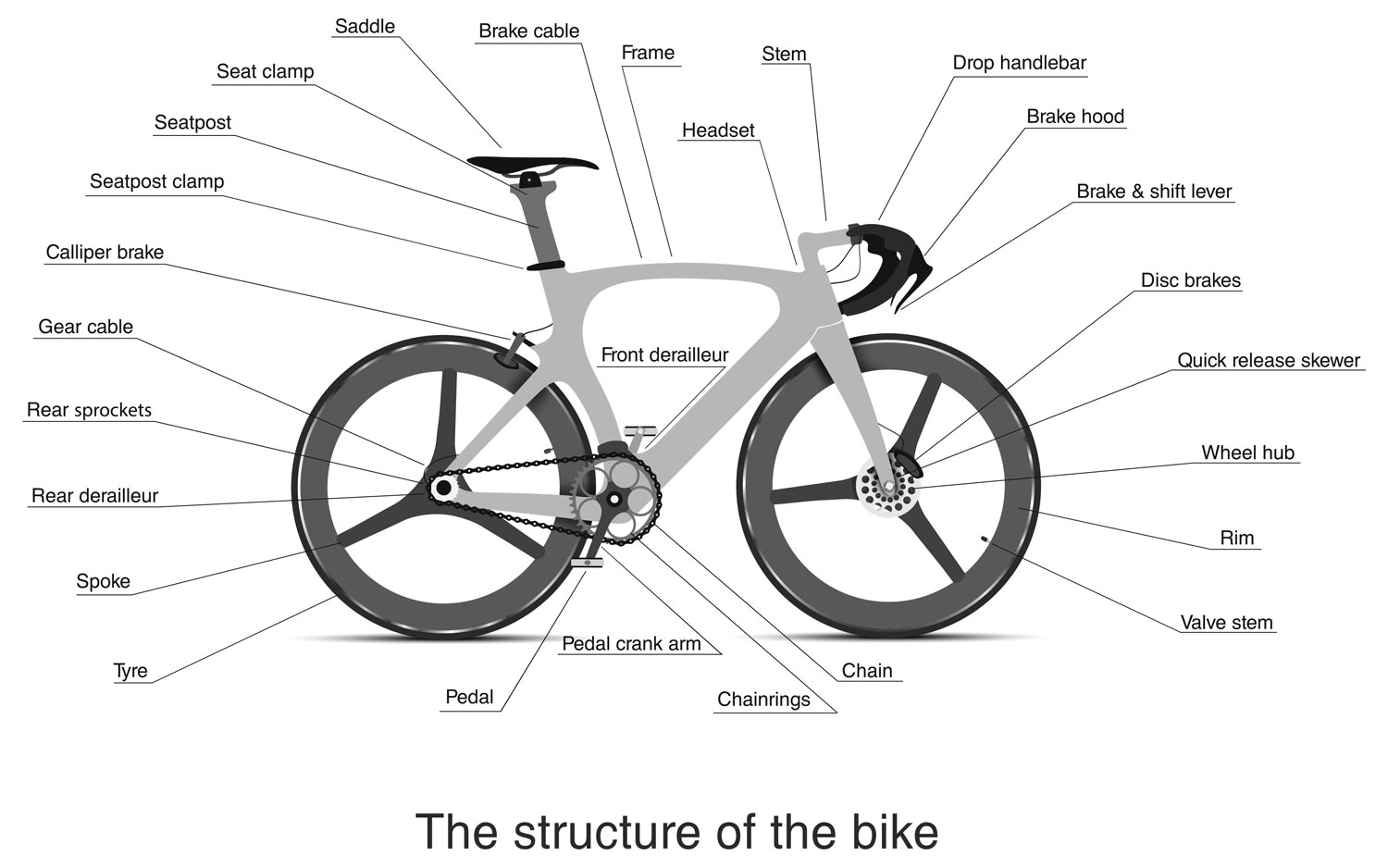
Figure 1. The components of a bicycle. © Andrei Kukla/Adobe Stock Images.
The essential components of a bike fit are the rider interview, physical evaluation, on-the-bike assessment and adjustments, post-fit instructions and documentation, and patient/client education. A complete bike fit always begins with the rider interview, which is essentially the subjective portion of a medical exam. The rider interview should include discussion of past and current medical history, reason for getting a fit, riding history, riding and/or competitive goals, current exercise routine, and any other specific rider concerns. It is important to understand what each individual rider wants out of the fitting experience. This is similar to understanding a patient’s goals for physical therapy treatment. Improving communication improves outcomes. The off-the-bike physical evaluation should be comprehensive and include cycling specific functional movement tests.
Fitters may use various types of technology during a bike fit, including a goniometer, plumb line, laser level, motion capture, and pressure mapping. More technology does not always result in a better fit outcome. No matter what technology a fitter uses, the fitter needs to be able to understand the data and know how to use it to help their patients.
The bike fitting profession is full of formulas and methods that help a fitter set saddle height, saddle fore-aft, handlebar reach, handlebar width, saddle-to-handlebar drop, and cleat positioning. A fitter should have a deep understanding of the components of a bicycle (Figure 1), including the various clipless pedal systems a rider may use. Cleats are fastened onto the bottom of the shoe with screws and are adjustable in 2–3 planes depending on the specific pedal system (Figure 2). Most brands of clipless pedals are adjustable in all three planes: anterior-posterior, medial-lateral, internal and external rotation. A good medical bike fit does not blindly adhere to a particular formula, but takes into account each rider’s unique anatomy and biomechanics. For example, to set saddle height, one formula would dictate that knee flexion at BDC should be 25° – 30°, whereas another says 35° – 40° is the correct range. How does a medical fitter determine the right knee flexion angle at BDC for a particular client? The fitter should take into account the rider’s flexibility; neural tissue tension; available hip, knee, and ankle range of motion; pedaling style; possible leg length discrepancy; any joint pathomechanics; and intended type of riding (road racing, commuting, etc.). Medical fitters should use this approach throughout a bike fit: one grounded in clinical reasoning and based on your medical assessment of the patient’s unique characteristics.
Common Fit-Related Postural and Gait Deviations
Many fit-related postural and gait deviations may be found in a cyclist. When assessing the upper body, static postural deviations are common. A fitter may find excessive cervical extension or thoracic flexion, shoulder internal rotation, shoulder horizontal abduction, shoulder horizontal adduction, shoulder flexion > or < 90°, full elbow extension, or wrist extension. Any of these findings may contribute to pain or injury. Findings of excessive cervical extension, thoracic flexion, shoulder flexion > 90°, or full elbow extension may indicate that the handlebar reach or drop is too large. Patients with these findings may complain of back or neck pain or saddle discomfort. Shoulder flexion 90° may result in shoulder, elbow, or wrist pain; or median or ulnar nerve paresthesias. Findings of shoulder internal rotation, shoulder horizontal adduction, or wrist extension may indicate bars that are too narrow. Patients may complain of paresthesias in the median or ulnar nerve distributions, wrist or hand pain, or cervicothoracic pain. Bars that are the wrong width (too wide or narrow) may also impair breathing by reducing ribcage expansion.
The lower extremities move reciprocally to power the bicycle. Many common gait deviations are found that provide useful data in diagnosing injury. Shirley Sahrmann, PT, PhD, developed the concept of Movement System Impairment Syndromes to identify faulty movement patterns that can lead to injury.4 This concept can be applied and expanded to understand bike fit-related pain and injury. There are several common faulty lower extremity movement patterns that are found in cyclists. A fitter may find excessive hip abduction and external rotation, genu varum, and supination. Riders with this presentation may complain of lower back, anterior or lateral hip, knee, or lateral foot pain. The initial correction for this finding is to widen the rider’s stance width. This can be achieved by moving the cleat medially, using a pedal with a longer spindle, or installing pedal spindle extenders. These riders often excessively rotate their cleats to promote a heel-in position, which will also likely need to be addressed. Often, correcting hip, knee, and foot alignment by normalizing stance width and cleat rotation will also correct faulty foot alignment. Forefoot and rearfoot posting with wedges or custom orthoses should be done after correcting movement impairments of the hip and knee.

Figure 2. How to adjust a cycling cleat. The cleat fastens to the shoe through 2-4 screws depending on the brand. The cleat may be moved anterior-posterior, medial-lateral, and internal and external rotation (adjustability depending on specific pedal system). © weerapat1003/Adobe Stock Images.
Another common faulty movement pattern is found in the rider with hip adduction and internal rotation, genu valgum, and pronation. These riders may complain of lower back, anterior or lateral hip, knee, or medial foot pain. To correct this faulty movement pattern, the stance width often needs to be decreased. This is achieved by moving the cleat laterally or using a pedal with a shorter spindle. An additional finding at the cleat may be excessive heel out, which should also be reduced.
A third faulty movement pattern is found in the rider with a saddle that is too high. This will result in ipsilateral trunk side flexion, hip adduction, increased knee extension, and increased plantarflexion with the crank at BDC. These riders may complain of lower back pain, abnormal nerve tissue tension symptoms in the sciatic nerve or its branches, saddle sores, posterior knee pain, iliotibial band symptoms, calf cramping, or foot pain or paresthesia.
Conversely, a saddle that is too low will result in contralateral trunk side flexion and excessive hip and knee flexion at TDC and excessive knee flexion and dorsiflexion at BDC. These riders often complain of lower back pain, anterior or lateral hip pain, anterior knee pain, and foot pain or paresthesia. In addition to raising saddle height, a fitter may consider using shorter cranks to further reduce the amount of hip and knee flexion at TDC. This intervention is particularly beneficial for riders with reduced available hip or knee flexion range of motion due to arthritis or other joint pathology.
A more complex faulty movement pattern is the rider who demonstrates excessive trunk, hip, and knee movement in the frontal and transverse planes that does not follow any of the above patterns. The problem is often a saddle that is too narrow and does not adequately support the ischial tuberosities. These riders often have a great variety of complaints, including saddle sores, lower back pain, knee pain, and foot pain. Selecting the correct width and model of saddle is often a matter of trial and error due to the variation in saddle shapes as well as how a rider sits on the saddle. Riders use varying amounts of anterior pelvic tilt throughout a ride. Variables such as terrain (hilly or flat) and level of effort influence the way a rider sits on a saddle. Riding at higher intensities partially unweights the ischial tuberosities due to the increased torque placed on the pedals.
Diagnosing Cycling Injuries
Cycling injuries fall into two general categories: traumatic and repetitive. Traumatic cycling injuries occur from crashes and may require temporary or permanent modifications to the rider’s position to accommodate for the injury. Cyclists are at high risk for repetitive use injuries due to the highly repetitive nature of cycling.2,3 If a cyclist pedals at 90 rpm, they will perform 5400 revolutions in a 1-hour ride. Most competitive cyclists train at least 8 hours per week, which would equal 43,200 revolutions per week. Repetitive cycling injuries are often caused by incorrect bike fit or neuromusculoskeletal pathology. A patient with a repetitive cycling injury will not get better without correction of the patient’s bike fit and/or addressing the patient’s specific physiological impairments. More often than not, both the bike and the rider need to be assessed and corrected for an optimal outcome.

The clinician should use the data gathered in both the off-the-bike and on-the-bike evaluation to make a diagnosis. Abnormal biomechanics observed on the bike help support objective findings from the off-the-bike evaluation. Common fit-related cycling injuries of the trunk and lower extremities include patellofemoral pain syndromes, lumbar radiculopathies, sciatic nerve entrapments (often at the piriformis or ischial tuberosity), sacroiliac joint pain, iliotibial band syndrome, trochanteric bursitis, pes anserinus bursitis, metatarsalgia, Morton’s neuroma, Achilles tendinopathies, plantar fasciitis, and saddle sores (skin abrasion, folliculitis, or abscess).2,3 The clinician must consider the patient’s available joint range of motion, strength, flexibility, off the bike static and dynamic alignment, neural tissue tension, and joint mechanics to fully determine the correct bike fit for that patient. For example, a patient with a 40° passive straight leg raise bilaterally will not tolerate a cycling position in which the handlebars are lower than the saddle. If that patient’s handlebars are set lower than the saddle, the patient will compensate for the lack of hamstring flexibility and sciatic nerve mobility by excessively flexing the thoracic spine, fully extending the elbows, and excessively plantarflexing at BDC. This patient might complain of back pain on the bike, or they may complain of neck, thoracic, ankle, or foot pain. They may also complain of cramping in the hip adductors or plantarflexors due to this compensatory pattern. A patient with the above presentation might report a primary complaint of Achilles pain. The clinician must consider local potential contributors to the patient’s symptoms, which include pes planus, significant leg length discrepancy, or a hypermobile foot; but should also assess the entire kinetic chain to determine the biomechanical root cause of the patient’s Achilles pain.5
Conclusion
A 2018 People for Bikes survey of 14,467 Americans found that 32% of Americans age 3 and older rode a bicycle in the past year.6 Due to the COVID-19 pandemic and social distancing requirements worldwide, participation in cycling in 2020 is booming. Bike retailers are reporting record sales, including a large increase in new riders with a higher potential for injury. Improvements in cycling technology are making cycling more accessible to people with medical diagnoses. Patients with arthritis, obesity, myopathies, and neurological disorders are greatly benefiting from electronic motor-assisted bicycles. Cycling-specific prosthetics are allowing people who have undergone amputations to ride with greater comfort and efficiency. Unfortunately, according to a literature review done by Dettori and Norvell in 2006, the prevalence of non-traumatic bicycle injuries may be as high as 85%.7 Injured cyclists will require medical practitioners with a deep understanding of cycling medicine to fully address their injuries and prevent new injuries in the future.
Andrea Myers, PT, DPT, is a board-certified clinical specialist in orthopaedic physical therapy. She works as a physical therapist at Carlson Therapy Network in Bethel, Connecticut, and as a bike fitter at Class Cycles in Southbury, Connecticut.
- Magee D. Orthopedic Physical Assessment. 6th ed. St. Louis: Saunders; 2014.
- Lefever-Button S. Cycling. In: Shamus E and Shamus J, eds. Sports Injury Prevention and Rehabilitation. New York: McGraw-Hill; 2001:459-483.
- Broker J. The Biomechanics of Cycling. In: Hughes C, ed. Orthopedic Management of the Cyclist, Runner, and Swimmer. Lacrosse, WI: Orthopaedic Section, APTA, Inc.; 2013.
- Sahrmann S. Movement System Impairment Syndromes of the Extremities, Cervical and Thoracic Spines. St. Louis: Mosby, Inc.; 2011.
- Kotler, D, Babu, Ashwin N, Robidoux, G. Prevention, Evaluation, and Rehabilitation of Cycling-Related Injury. Current Sports Medicine Reports: 2016; 15(3): 199-206.
- People for Bikes. (2018). U.S. Bicycle Participation Report. People for Bikes. https://peopleforbikes.org/resources/u-s-bicycling-participation-report/
- Dettori, N.J., Norvell, D.C. Non-Traumatic Bicycle Injuries. Sports Med. 2006; 36: 7–18.





