
By Xiao Chen, Yuanhe Fan, Hongliang Tu, and Yuan Luo
Assessing the clinical efficacy of different therapeutic options for KOA will aid clinicians in treating patients.
 While clinicians recognize the positive role of physical therapy in improving symptoms and functionality in knee osteoarthritis (KOA) patients, these methods may differ in mechanisms of action, applicability, and efficacy variances. Thus, the aim of this study was to assess and compare the clinical efficacy of various therapeutic options in treating patients with KOA.
While clinicians recognize the positive role of physical therapy in improving symptoms and functionality in knee osteoarthritis (KOA) patients, these methods may differ in mechanisms of action, applicability, and efficacy variances. Thus, the aim of this study was to assess and compare the clinical efficacy of various therapeutic options in treating patients with KOA.
Methods
The authors performed a comprehensive search of PubMed, Embase, OVID, Cochrane Library, and Web of Science databases from their inception to December 10, 2023, identifying randomized controlled trials (RCTs) examining the effects of therapeutic options on KOA. Two researchers independently performed literature screening, data extraction, data collection and organization, and quality assessment. The data obtained were subjected to statistical analysis and graphical representation using Stata 17.0 software.
Results
In total, 139 RCTs encompassing 9,644 KOA patients and involving 12 therapeutic options were included: low level laser therapy (LLLT), high intensity laser therapy (HILT), transcutaneous electrical nerve stimulation (TENS), interferential current (IFC), short wave diathermy, ultrasound, lateral wedged insole, knee orthoses, exercise, hydrotherapy, kinesio taping (KT), and extracorporeal shock wave therapy (ESWT). Per the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) pain score, knee orthoses were determined to be the most likely to yield the best results, followed by exercise and HILT. In terms of WOMAC function score, knee orthoses emerged as the technique with the highest likelihood of being optimal, followed by hydrotherapy and ESWT. Knee orthoses ranked highest in effectiveness concerning the WOMAC stiffness score, followed by exercise and hydrotherapy. For the total WOMAC score, hydrotherapy demonstrated the highest probability of being the best technique, followed by exercise and HILT. Regarding the visual analog scale (VAS)-rest, hydrotherapy exhibited the greatest likelihood of being the optimum technique, followed by HILT and LLLT. In terms of VAS-activity, knee orthoses had the highest probability of being the best technique, followed by LLLT and exercise. Overall, knee orthoses had the highest probability of being the best technique, followed by hydrotherapy and exercise. (Figure.)
Discussion
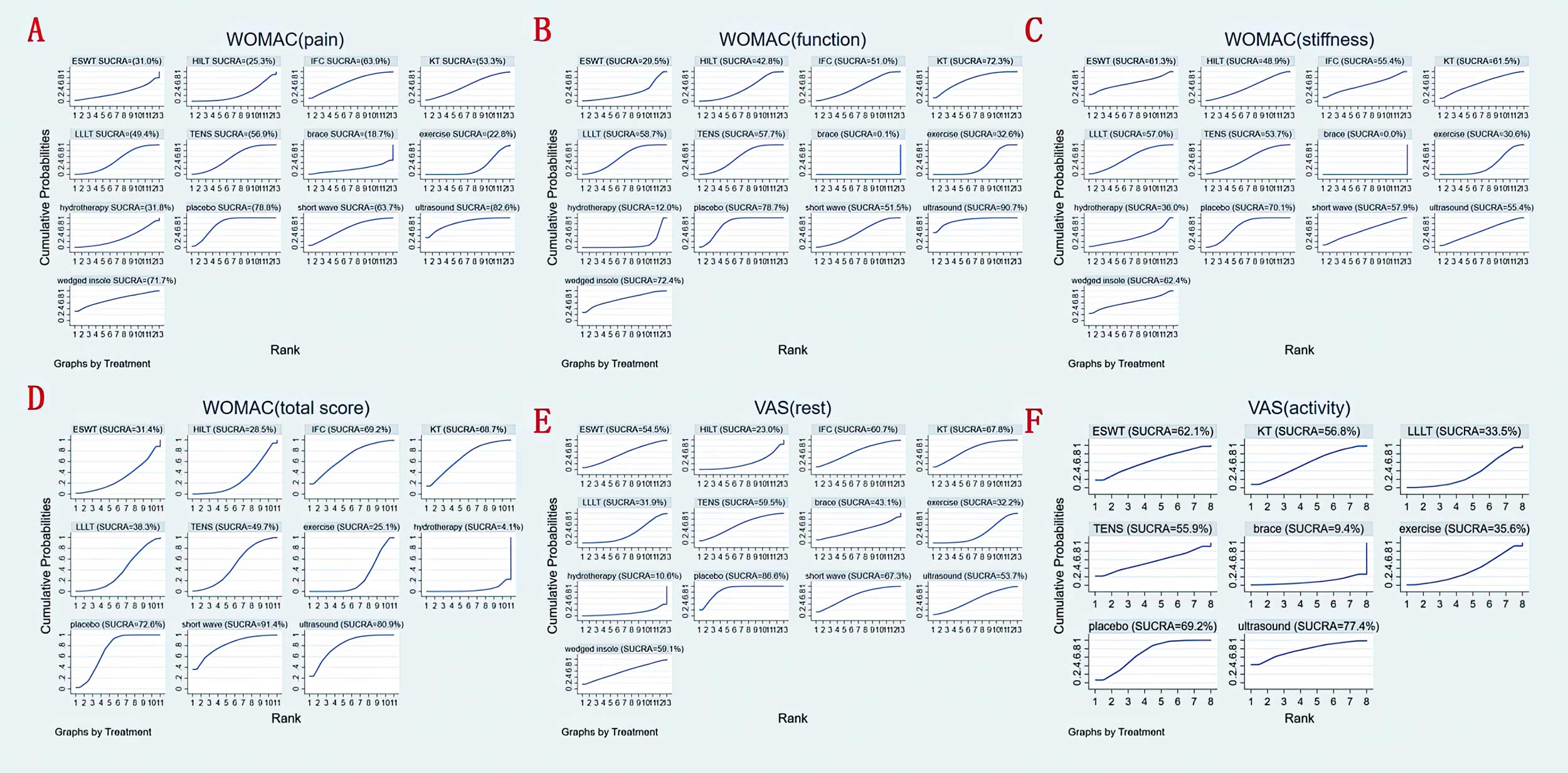
Figure. Surface under the cumulative ranking (SUCRA) for (A) WOMAC pain score, (B) WOMAC function score, (C) WOMAC stiffness score, (D) total WOMAC score, (E) VAS-rest and (F) VAS-activity at last follow-up.
Overall, knee orthoses provide the most effective treatment for KOA by (1) improving joint biomechanics by adjusting the knee joint’s force line to evenly distribute load and reduce excessive stress on cartilage and soft tissues; (2) enhancing joint stability by limiting excessive knee movement in unstable conditions, thereby reducing injury risk and pain; (3) alleviating muscle fatigue by supporting surrounding muscles and reducing their workload to maintain joint function; (4) adjusting proprioception to improve patients’ awareness of knee joint position and movement, enhancing joint control; and (5) reducing the inflammatory response by limiting inflammation spread and easing related symptoms.
For pain reduction, this study demonstrates that aquatic therapy is particularly effective and low impact. Evidence has shown that this therapy, which can involve exercise in water or the use of water’s properties for treatment, significantly reduces pain and enhances physical function through heat stimulation and buoyancy. Increased water depth provides greater buoyancy, unloading the joints and consequently easing the pain associated with KOA.
This study reveals that HILT, in terms of overall efficacy, is surpassed only by knee orthoses, hydrotherapy, and exercise therapy. In terms of pain alleviation, the efficacy of both HILT and LLLT is secondary only to that of hydrotherapy. Clinically, LLLT has been shown to mitigate pain and inflammation, facilitate healing and tissue repair, and enhance blood circulation. HILT, providing concentrated laser energy over a brief period, penetrates deeper into tissues, eliciting a more potent biostimulative and anti-inflammatory response.
Substantial evidence supports the improvement of KOA symptoms, including pain, functionality, and quality of life, through exercise intervention, with aerobic and mind-body exercises showing the most significant benefits for pain and function, while strengthening and flexibility/skill exercises are the next best options. A prior network meta-analysis conducted by Mo et al. investigated the clinical efficacy of 5 different exercise therapies for the management of KOA, including aquatic exercise (AE), stationary cycling (CY), resistance training (RT), traditional exercise (TC), and yoga (YG). The findings concluded that AE (for pain relief) and YG (for alleviating joint stiffness, improving knee function, and enhancing quality of life) are the most effective interventions, followed by RT, CY, and TC. This study considers various exercise therapies as a single intervention for comparison with other treatment modalities, indicating that exercise therapy is effective in improving knee joint function and warrants broader clinical application.
This study’s conclusions align with prior findings indicating that while pulsed ultrasound is moderately effective for pain improvement, it does not significantly enhance other knee joint functions.
Wedge insoles, similar to knee orthoses, primarily aim to alleviate knee joint stress by modifying joint load. Clinically, lateral wedge insoles are predominantly utilized. However, studies indicate that they do not outperform neutral devices in pain reduction. The reduction of the knee adduction moment by only 5–6% may be insufficient for pain alleviation. Additionally, factors like the sagittal moment and muscle co-contraction might have a more profound impact on the medial knee load, suggesting that a decrease in the adduction moment alone is not adequate to improve KOA function and pain.
When evaluating overall treatment efficacy, emphasis is placed on the WOMAC score and the resting VAS pain score, as these assessments are nearly universally conducted in the literature, thus offering a more robust framework for both direct and indirect comparative analyses.
Conclusion
This study aimed to ascertain the comparative effects of various physical therapies for KOA, to aid clinicians in precisely selecting the most suitable physical therapy method based on individual patient conditions, enhancing treatment efficacy, reducing unnecessary medical resource wastage, and providing robust guidance and evidence for future research directions. The findings suggest that knee orthoses may be the most recommended therapeutic option for the KOA followed by hydrotherapy and exercise.
Xiao Chen, Yuanhe Fan, and Hongliant Tu are affiliated with the Department of Orthopedics, the First People’s Hospital of Neijiang, Neijiang, China.
Yuan Luo is affiliated with the Department of Rehabilitation, the First People’s Hospital of Neijiang, Neijiang, China.
This article has been excerpted from “Clinical efficacy of different therapeutic options for knee osteoarthritis: A network meta-analysis based on randomized clinical trials.” PLOS ONE 20(6): e0324864. https://doi.org/10.1371/journal.pone.0324864. Editing has occurred, including the renumbering or removal of tables and figures, and references have been removed for brevity. Use is per CC-BY 4.0 International.





