
 By Angela Kelley, PA-C, MSM
By Angela Kelley, PA-C, MSM
Varicose veins (VVs)—those bulging, twisted blood vessels typically seen on the legs—are more than an esthetic issue. They can be painful and affect patients’ quality of life; left untreated, they can lead to life-threatening chronic venous insufficiency and venous ulcers. And when seen or mentioned, will always warrant a clinician’s attention.
VVs are a common occurrence noted in healthcare. This primer, which will appear as 2 articles, includes data published within the last 5 years with information in Part I not only on how to diagnose VVs, but also on the anatomy and pathophysiology related to development, risk factors for occurrence, clinical presentation, and differential diagnoses. Part II, which will appear next month, will include information on treatment, prevention, and complications of this condition. There are additional terms that will be explored such as chronic venous insufficiency (CVI), and chronic venous disease (CVD); however, it is important to note at the outset that these terms are not interchangeable with the term varicose veins.
Definitions
Varicose Veins
Varicose veins (VVs) are superficial veins that are dilated and bulging with diameters measuring 3 mm or greater that can progress to become more enlarged and more tortuous.1 Patients with VVs can be either asymptomatic or have pain and even bleeding if progression occurs. VVs are the most common manifestation of CVD and usually manifest as stage C2 in the CEAP (see below).2
Chronic Venous Disease
Chronic venous disease (CVD) is a general term describing complications in the venous system caused by dysfunctional valves and venous reflux.3 Differentials related to CVD should include causes of lower extremity edema including hypoalbuminemia, cardiac insufficiency, hypothyroidism, and more.2,4
Chronic Venous Insufficiency
Chronic venous insufficiency (CVI) is mainly caused by ambulatory venous hypertension due to abnormal blood flow from reflux of venous valves, obstruction of venous valves, or a combination of both.1 The causes of CVI include VVs as well as reticular veins, telangiectasias, pigmentation, edema, lipodermatosclerosis, eczema, venous ulcers, and atrophie blanche. These additional exam findings are important to note to determine differential diagnoses that could cause venous abnormalities.5
CEAP Classification
VVs represent one aspect of venous disease, which is generally reported using the international standard known as CEAP: Clinical-Etiology-Anatomy-Pathophysiology Classification (Table 1).2 CEAP, which is based on clinical manifestations of chronic venous disorders, helps to standardize diagnoses, improve communications among clinicians, and facilitates research. Class C0 represents no visible sign of venous disease; classes C1–3 typically denote CVD, while classes C4-6 are indicative of the more severe CVI.
Anatomy | Physiology | Pathophysiology
The venous system is just 1 part of the entire circulatory system that keeps blood and lymph fluids flowing in the body. The venous system is responsible for returning deoxygenated blood back to the heart. This is accomplished through an intricate network of perforating, superficial, and deep veins. In other words, venous blood is carried from the skin to the superficial veins, which are then channeled into the deep veins of the lower limbs. Typically, deep veins are located within the same vascular sheath as the artery of the same name, which allows arterial pulsations to aid venous return.
Using a system of internal valves and the pumping action of both the large lower limb muscles and the vascular smooth muscle cells within the veins themselves, these veins support the correct direction of blood flow throughout the entire venous system.1 It is important that each of these components function properly to counter the pull of gravity and thus avoid pooling of blood in the lower extremities (pooling here means slower return to the heart, not stagnation).6 (See Figure 1.)
Pressure within the entire circulatory system is affected by changes in postural position: venous pressure in the lower extremities is estimated around 90 mm Hg when standing and lessens to 30 mm Hg when lower extremities are elevated or while walking.1 Walking activates a pumping action in the lower extremity muscles serving as a natural aid in blood flow. Although venous valves are typically bicuspid and unidirectional for the purpose of directing blood flow back to the heart, complications in these valves can lead to a reflux of blood in the opposite direction.6-8 It is important to note that not all lower extremity veins contain valves (particularly in the feet),1 which can affect venous return in patients with an incompetent venous system.
Although the pathogenesis of VVs is not fully understood, damaged or improperly working valves and changes that cause dilation and remodeling of the vessel walls as well as the loss of tone have been identified.3,9 Those changes include hypoxia, inflammation, increased filling pressure in the veins, activation of the endothelium, and dysregulation of metalloproteinases and tissue inhibitors, as well as genetic factors and other underlying risk factors.9,10 VVs have been identified as the first clinical evidence of CVD.11

Figure 1. The lower extremity venous system, and changes to varicose veins. The lower extremity has an intricate system of superficial and deep veins connected by perforator veins. Excessive vein wall dilation and incompetent venous valves lead to superficial dilated spider veins or engorged and tortuous varicose veins. Image reprinted from Chen Y, Peng W, Raffetto JD, Khalil RA. Matrix Metalloproteinases in Remodeling of Lower Extremity Veins and Chronic Venous Disease. Prog Mol Biol Transl Sci. 2017;147:267-299. DOI: 10.1016/bs.pmbts.2017.02.003. Elsevier Copyright ©2017; all rights reserved.
Risk Factors
Environmental: Risk factors for the development of VVs are multifaceted:1,3,5,6,9,10
- Increasing age
- Standing for long periods of time
- Trauma to the lower extremity
- Obesity
- Smoking
- Family history
- Pregnancy and other states of elevated estrogen
- Sedentary lifestyle
Additional risk factors such as high systolic blood pressure,10 Caucasian race,6 chronic constipation leading to increased intra-abdominal pressure,6 and decreased mobility6 have also been recognized.
Genetic: A 2018 study published in PLoS One9 that looked at genetic data on more than 408,000 European ancestry individuals reported finding the most likely causal genes as well as variants that related to hypertension and certain traits of blood cells. Additional findings indicated genetic correlation related to certain associations of VVs in individuals whose jobs require long periods of standing, those who have VVs and develop deep vein thrombosis (DVT), and other correlations, as well as indications from plasma protein levels that are related to size-proportional traits such as height, weight, waist circumference, and others. Additional genetic correlations have been found to increase the risk for VVs including 30 novel genome loci related to blood pressure encoding and the development, integrity, and maturation of vascular channels.3
Prevalence
Presence of VVs has been noted in nearly one third of the population age 18–64,6 with increased occurrences with age. Research shows VVs are present in 30% of adults in developed countries9 and lower extremity VVs in particular are believed to be the 7th most common reason for physician referral in the United States.12 The cost associated with VVs treatment was $290.59 million in the United States in 2016 and was expected to rise to $396 million by 2021.10 Those same authors also noted that 1 out of every 65 patients have a VV treatment performed yearly.
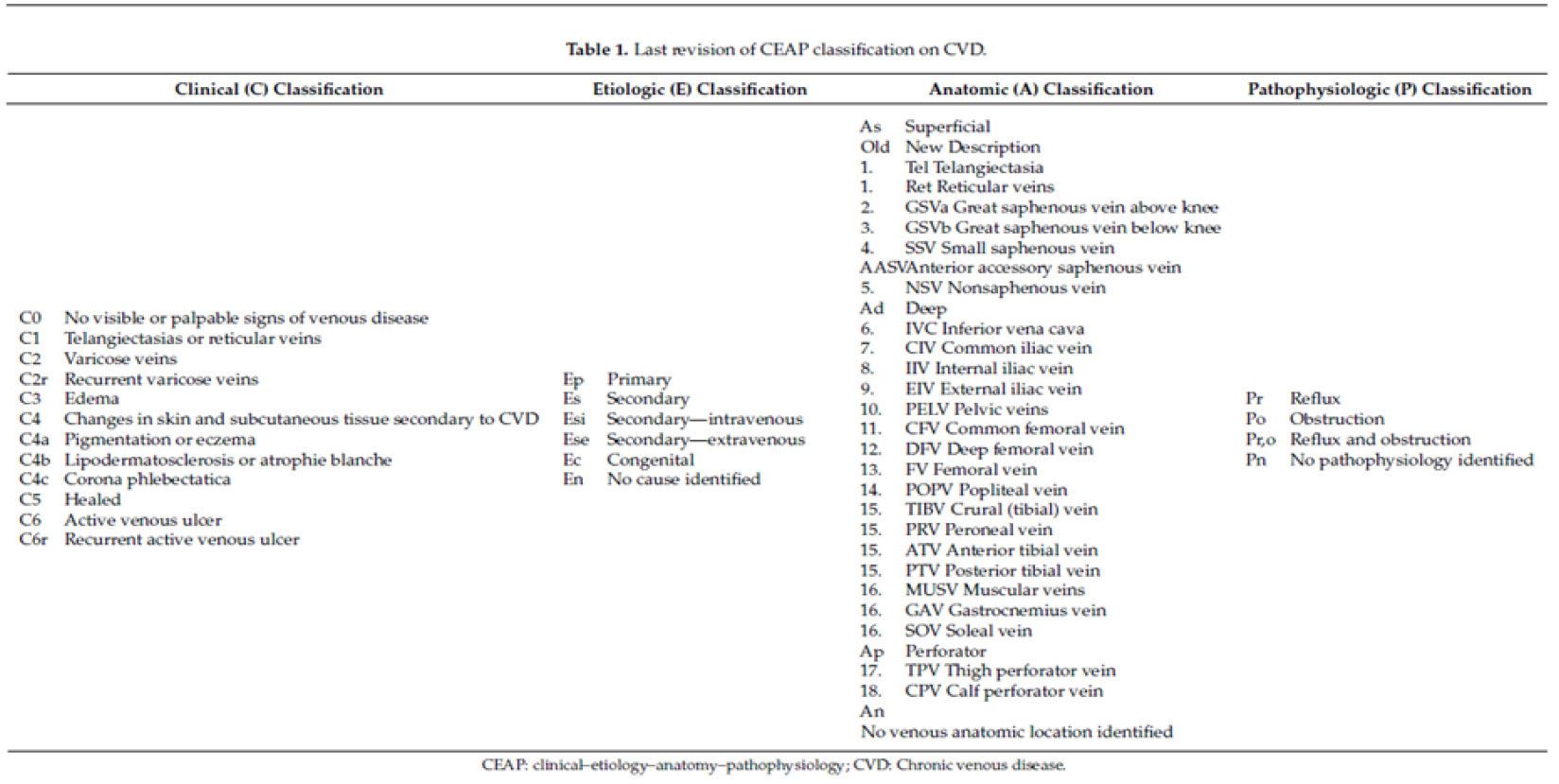
Image reprinted from reference 2. Use is per the Creative Commons Attribution (CC BY) license.
History
The subjective history of varicose veins can be either an asymptomatic presentation or 1 with various levels of pain.1 Often, patients present with an interest in treatment for cosmetic purposes.
Asymptomatic presentation could present with concerns for appearance, social impact related to relationships, restrictions related to leisure or physical activities, anxiety related to progressive deterioration into worsening conditions such as DVT or venous leg ulcers, or limitations in daily life.12
Symptomatic presentation has been shown to include the following:5,6,12

- Itching
- Pain
- Heaviness
- Leg cramps
- Numbness
- Tingling
- Skin changes
- Swelling
- Restlessness of the lower extremities
The level of pain can range from a slight discomfort to significant pain and cramping where the symptoms are worse after prolonged standing.1,5 Often, many symptoms resolve after resting and elevating the lower extremities.5 A 2017 systematic literature review found that 5–15% of men and 2–29% of women worldwide experience VVs.12
Physical Exam Findings
Physical findings related to subjective concerns can vary based on patient presentation. An examination should be performed on bilateral lower extremities regardless of unilateral or bilateral subjective concerns.6 Skin changes, such as eczema, hemosiderin deposits, lipodermatosclerosis, atrophie blanch, skin ulceration, lumps under the skin, and edema, can be signs of early or late disease related to VVs. VVs can also present as engorged and dilated masses3 or simply enlargement of superficial veins.11 Palpation of these atypical findings should occur to compare physical findings with subjective concerns, and to note the progression of the varicosities toward more chronic venous conditions. Palpation to assess the size of the veins and ankle mobility5 are important as is palpating arterial pulses to determine the ankle-brachial pressure index6 to evaluate if chronic conditions such as ulceration are beginning. Concern would be warranted if palpation of the vein indicates a hard lump that is tender, as superficial thrombophlebitis should be ruled out. Although our focus here is on VVs of the lower extremities, clinicians should perform a more complete exam to determine if a rare pelvic or abdominal mass could be the etiology of varicosities that are present or other conditions.6
Diagnosis
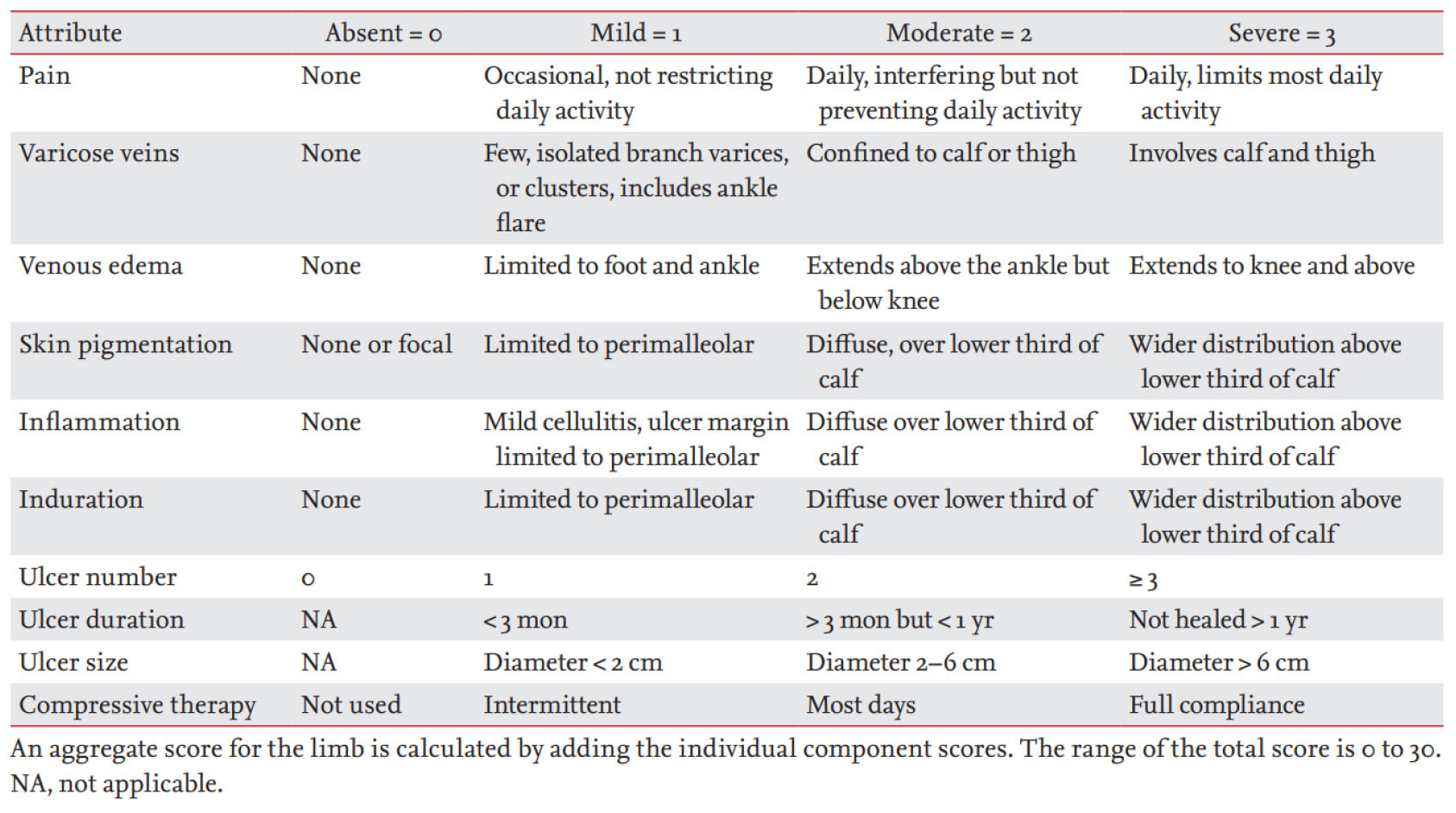
Image reprinted from reference 1. Use is per the Creative Commons Attribution (CC BY) license.
VVs are typically diagnosed via a clinical presentation from the history and physical findings of a dilated vein of 3 mm or greater in diameter that is noted when the patient is in an upright position.5 A concern for external hemorrhage of a VV leading to hemodynamically significant changes is rare but has been noted in the literature.5,13 The additional evaluations suggested for the physical diagnosis are important to determine progression of the varicosity condition as VVs are noted to be a clinical feature of CVI.1,10,11
After taking a history and performing a physical examination, the CEAP classification (Table 1) may be used to determine the stage and or progression of CVD. If VVs are present, the clinical manifestations (C) will be noted at the level of C2, whereas CVI is diagnosed at levels C3–C6, noted from simply edema (C3) and dermatological changes (C4) to healed and active ulcers (C5 and C6, respectively).2 Although the CEAP classification is helpful in determining etiology of VVs as primary, secondary, or congenital, and superficial, deep, or perforating, this classification system is static and not helpful for severity scoring.1 An additional evaluation is provided in Table 2,1 which standardizes the evaluation, assessment of severity, and treatment response.1,14,15,16
Differential Diagnoses and Tests
As discussed, differential diagnoses should be ruled out when considering the diagnosis of VVs. As noted, determining whether there is a larger underlying condition related to chronic venous disease other than VV presentation should be assessed. Determining whether varicose veins are the only manifestation of the genetic and environmental risk factors, or if the condition should be evaluated to determine progression to chronic venous insufficiency should be considered as well as ruling out more concerning differentials.
The diagnostic test of choice for VVs is venous duplex ultrasonography.5,17,18 This diagnostic modality is a painless, easily accessible, and noninvasive method for evaluating venous junctions, venous reflux, incompetent veins, and can rule out superficial and DVT.5 Other tests mentioned in the literature such as plethysmography, computed tomography, magnetic resonance venography,1 intravascular ultrasound,1 bloodwork for deep venous thrombosis, as well as genetic testing,2,3 are reserved for venous disorders that progress toward CVI, those who have a past medical history that includes thrombosis,9 or those who are preparing for surgical intervention.1
“Varicose Veins of the Lower Extremities: A Primer Part II” will appear next month and will cover treatment options and potential complications.
Angela Kelley, PA-C, is Associate Professor and Director of Didactic Education, Physician Assistant Program at Gannon University in Ruskin, Florida, and a Regional Director Health Coach with Optavia (www.optavia.com/us/en/coach/angela).
Varicose veins affect nearly one third of the adult population and are considered early warnings of the more serious chronic venous insufficiency. Early recognition and prevention are key to suppressing potential life-threatening damage and maintaining patient quality of life.
Suggested Further Readings
- Gloviczki P, Lawrence PF, Wasan SM, et al. The 2023 Society for Vascular Surgery, American Venous Forum, and American Vein and Lymphatic Society clinical practice guidelines for the management of varicose veins of the lower extremities. Part II: Endorsed by the Society of Interventional Radiology and the Society for Vascular Medicine. J Vasc Surg Venous Lymphat Disord. 2024 Jan;12(1):101670. doi: 10.1016/j.jvsv.2023.08.011.
This Part II of their guidelines focuses on evidence supporting the prevention and management of varicose veins with compression, drug therapies and nutritional supplements, evaluations of varicose tributaries and superficial venous aneurysms, and management of complications. - Singh A, Gattani R. A Narrative Review of Advancements in Understanding and Treating Varicose Veins. Cureus. 2023 Nov 1;15(11):e48093. doi: 10.7759/cureus.48093.
Varicose veins, marked by the presence of dilated and tortuous subcutaneous vessels, precipitate both physical discomfort and cosmetic concerns, frequently necessitating meticulous clinical evaluation coupled with ultrasound studies to secure a precise diagnosis. - Tan M, Campbell B, Parsi K, Davies AH; UIP. Management of bleeding varicose veins. Phlebology. 2024 May;39(4):273-275. doi: 10.1177/02683555231219548
Bleeding associated with varicose veins is not uncommon and can be a sudden cause of death. This article includes a 1 page algorithm for managing bleeding in these patients.
- Youn YJ, Lee J. Chronic venous insufficiency and varicose veins of the lower extremities. Korean J Intern Med. 2019;34: 269–283. doi.org/10.3904/kjim.2018.230.
- Ortega MA, Fraile-Martinez O, Garcia-Montero C, et.al. Understanding chronic venous disease: A critical overview of its pathophysiology and medical management. J Clin Med. 2021;10(15):3239. doi: 10.3390/jcm1015323.
- Raffetto JD, Khalil RA. Mechanisms of lower extremity vein dysfunction in chronic venous disease and implications in management of varicose veins. Vessel Plus. 2021;5:36. doi: 1020517/2574–1209.2021.16.
- Trayes KP, Studdiford, JS, Pickle S, Tully AS. Edema: diagnosis and management. Am Fam Phys. 2013;88:102–110.
- Raetz J, Wilson M, Collins K. Varicose veins: diagnosis and treatment. Am Fam Phys. 2019;99(11):682–688.
- Atkins E, Mughal NA, Place F, et al. Varicose veins in primary care. BMJ. 2020;370:m2509. doi.org/10.1136/bmj.m2509.
- Onida S, Lane TR, Davies AH. Improving the management of varicose veins. Practitioner. 2013 Nov-Dec;257(1766):21-4, 2–3.
- Pollack AA, Taylor BE, et al. The effect of exercise and body position on the venous pressure at the ankle in patients having venous valvular defects. J Clin Invest. 1949;28(3):559–63.
- Shadrina AS, Sharapov SZ, Shashkova TI, Tsepilov YA. Varicose veins of the lower extremities: Insights from the first large-scale genetic study. PLOS Genet. 2019;15(4): e1008110. PMID: 30998689. doi: 10.1371/journal.pgen.1008110.
- Davies AH. The seriousness of chronic venous disease: A review of real-world evidence. Adv Ther. 2019;36(Suppl 1):S5-S12. doi.org.10.1007s12325-019-0881-7.
- Raffetto JD, Ligi D, Maniscalco R, et al. Why venous leg ulcers have difficulty healing: Overview on pathophysiology, clinical consequences, and treatment. J Clin Med. 2021;10(1)29. doi.org/10.3390/jcm10010029.
- Lumley E, Phillips P, Aber A, et al. Experiences of living with varicose veins: A systematic review of qualitative research. J Clin Nurs. 201928(7-8):1085-1099. doi: 10.1111/jocn14720.
- Racette S, Sauvageau A. Unusual sudden death: two case reports of hemorrhage by rupture of varicose veins. Am J Forensic Med Pathol. 2005;26(3):294–296. doi: 10.1097/01.paf.0000176283.19127.0e.
- Sudoł-Szopi´nska I, Bogdan A, Szopinski T, Panorska AK, Kołodziejczak M. Prevalence of chronic venous disorders among employees working in prolonged sitting and standing postures. Int. J Occup Saf Ergon. 2011;17(2):165–173. doi: 10.1080/10803548.2011.11076887.
- Sharma S, Vashist M, Vashist MG. Family history as major predisposing factor in varicose veins disorder. Eur J Biomed Pharm Sci. 2017;4(12):392–396.
- Vlajinac HD, Radak DJ, Marinkovi´c JM, Maksimovi´c MŽ. Risk factors for chronic venous disease. Phlebology 2012,27, 416–422. doi.org/10.1258/phleb.2011.011091.
- Gloviczki P, Comerota AJ, Dalsing MC, et al. The care of patients with varicose veins and associated chronic venous diseases: clinical practice guidelines of the Society for Vascular Surgery and the American Venous Forum. J Vasc Surg. 2011;53(5 suppl):2S–48S. doi.org/10.1016/j.jvs.2011.01.079
- National Institute for Health and Care Excellence. Varicose veins: diagnosis and management. Clinical guideline 168. July 2013. https://www.nice.org.uk/guidance/cg168. Accessed Sept. 3, 2024.






I recently came across options for vein stripping near me while researching older treatments. It’s interesting to compare how newer, less invasive therapies have started to replace traditional procedures for many patients