
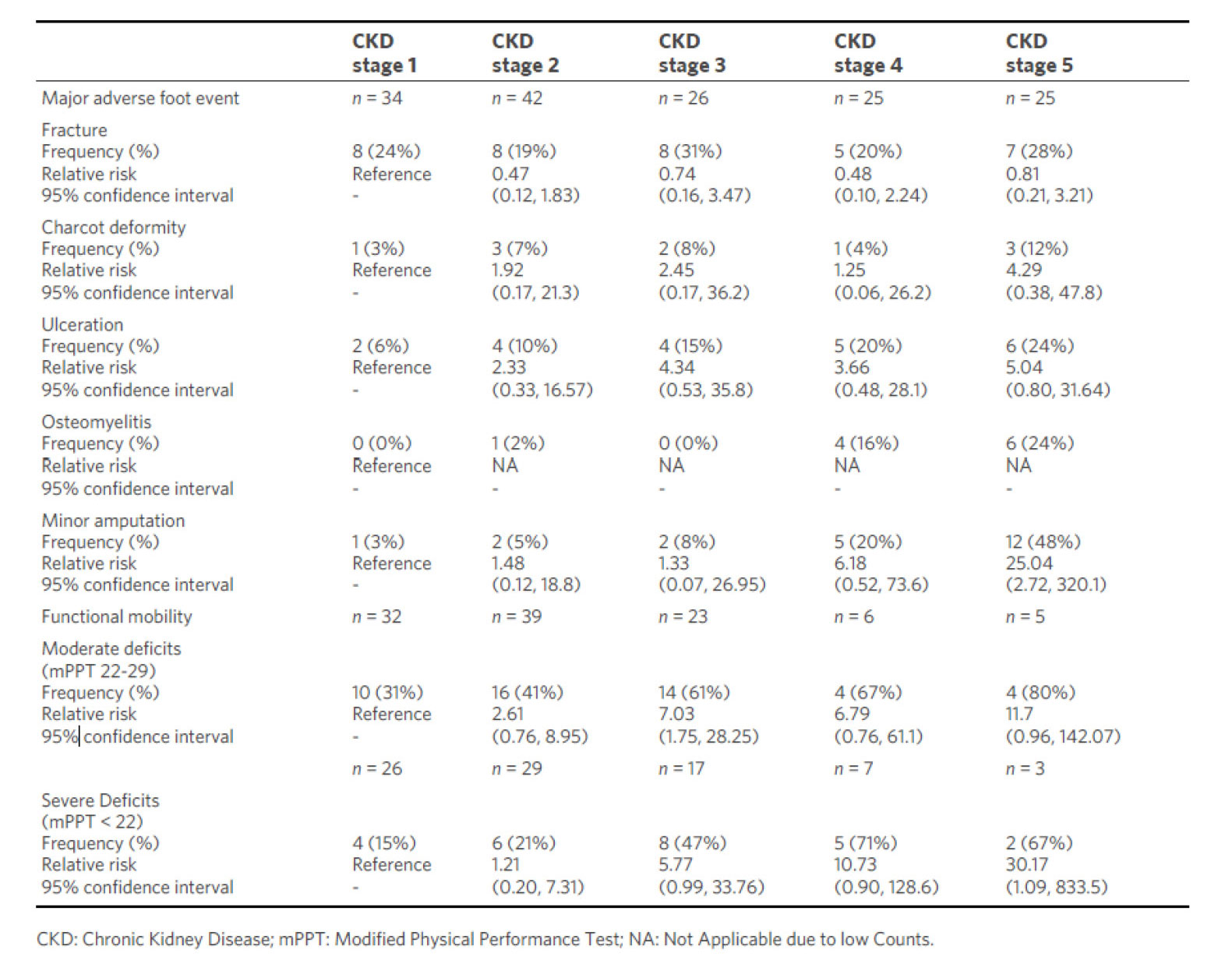
Table. Age-, body weight-, Hbalc-, and race-adjusted risk ratio of major adverse foot events and physical function by stage of chronic kidney
Peripheral neuropathy affects millions of individuals worldwide. The lifetime prevalence of peripheral neuropathy is estimated to be 50% among individuals with diabetes mellitus and this prevalence tends to increase with the duration of diabetes. Diabetic peripheral neuropathy (DPN) typically affects the distal extremities (feet and hands) and is, therefore, recognized as one of the incipient contributors to major adverse foot events (MAFEs) including foot fracture, ulcerations, Charcot neuropathic arthropathy (CN), osteomyelitis, and minor foot amputations or foot bone resections. MAFEs can singularly and collectively lead to major lower extremity amputation, which in turn can severely compromise an individual’s functional mobility and quality of life.
Diabetic nephropathy, a form of chronic kidney disease (CKD), is another major complication of diabetes mellitus, with a reported occurrence in 20%-50% of those with diabetes. Like DPN, diabetic kidney disease progresses in severity with diabetes duration.
DPN combined with diabetic kidney disease progression may be the root causes of both MAFEs and early functional mobility deficits in individuals with diabetes mellitus, though this has not heretofore been demonstrated. The purpose of this study is to describe the frequency and relative risk for major adverse foot events and functional mobility deficits in those with DPN across the stages of CKD.
These authors studied 284 participants with diabetes mellitus, peripheral neuropathy, and CKD. MAFEs including foot fracture, ulcerations, Charcot neuropathic arthropathy (CN), osteomyelitis, and minor foot amputations were collected from foot x-ray reports in the medical records of 152 participants; functional mobility deficits were assessed in 132 participants using the modified physical performance test (mPPT). Moderate mobility deficit was categorized as mPPT scores 22-29 and severe mobility deficit as < 22. Unadjusted and adjusted (age, body weight, race, HbA1c) risk ratios (RR) were calculated across each stage of CKD, with stage 1 CKD used as the reference group.
As noted in the table, the RR for neuropathic foot fracture, CN, and diabetic foot ulceration remained consistent across CKD stages. The RR of minor amputation is greater in CKD stages 4 and 5. The RR of moderate or severe mobility deficit is greater in CKD stages 3 and 5 and in CKD stages 3, 4, and 5, respectively. An inverse association was observed between MAFE prevalence and mPPT scores across CKD stages.
The authors concluded that major adverse foot events and functional mobility deficits are prevalent in individuals with DPN and diabetic kidney disease. The risks for minor foot amputation and functional mobility deficits increase as early as stage 3 CKD and increase further in stages 4 and 5.
Source: Sinacore DR, Jones MA, Kline PW. Major adverse foot events and functional mobility deficits associated with diabetic neuropathy and nephropathy. Metab Target Organ Damage. 2024;4:15. https://dx.doi.org/10.20517/mtod.2024.02. Use is per Creative Commons Attribution 4.0 International License.





