
 By Elias Schriwer, Robin Juthberg, Johanna Flodin, and Paul W. Ackermann
By Elias Schriwer, Robin Juthberg, Johanna Flodin, and Paul W. Ackermann
Mapping muscle motor points in the calf could improve electrode placement for neuromuscular electrical stimulation and thereby enhance outcomes.
Muscle contractions in the calf induced by neuromuscular electrical stimulation (NMES) may prevent venous thromboembolism, help rehabilitation, and optimize strength training, among other uses. However, compliance to NMES treatment is limited by the use of suboptimal stimulation points which may cause discomfort and less effectivity. Knowledge of where it is most likely to find muscle motor points (MP)—defined as the point on the skin that resulted in a small but clearly visible contraction of a muscle in the calf at the lowest possible level of stimulation by an NMES device—could improve NMES comfort and compliance. Toward that end, the aim of this study is to anatomically map the MPs of the calf as well as calculate the probability of finding an MP in different areas of the calf.
Methods
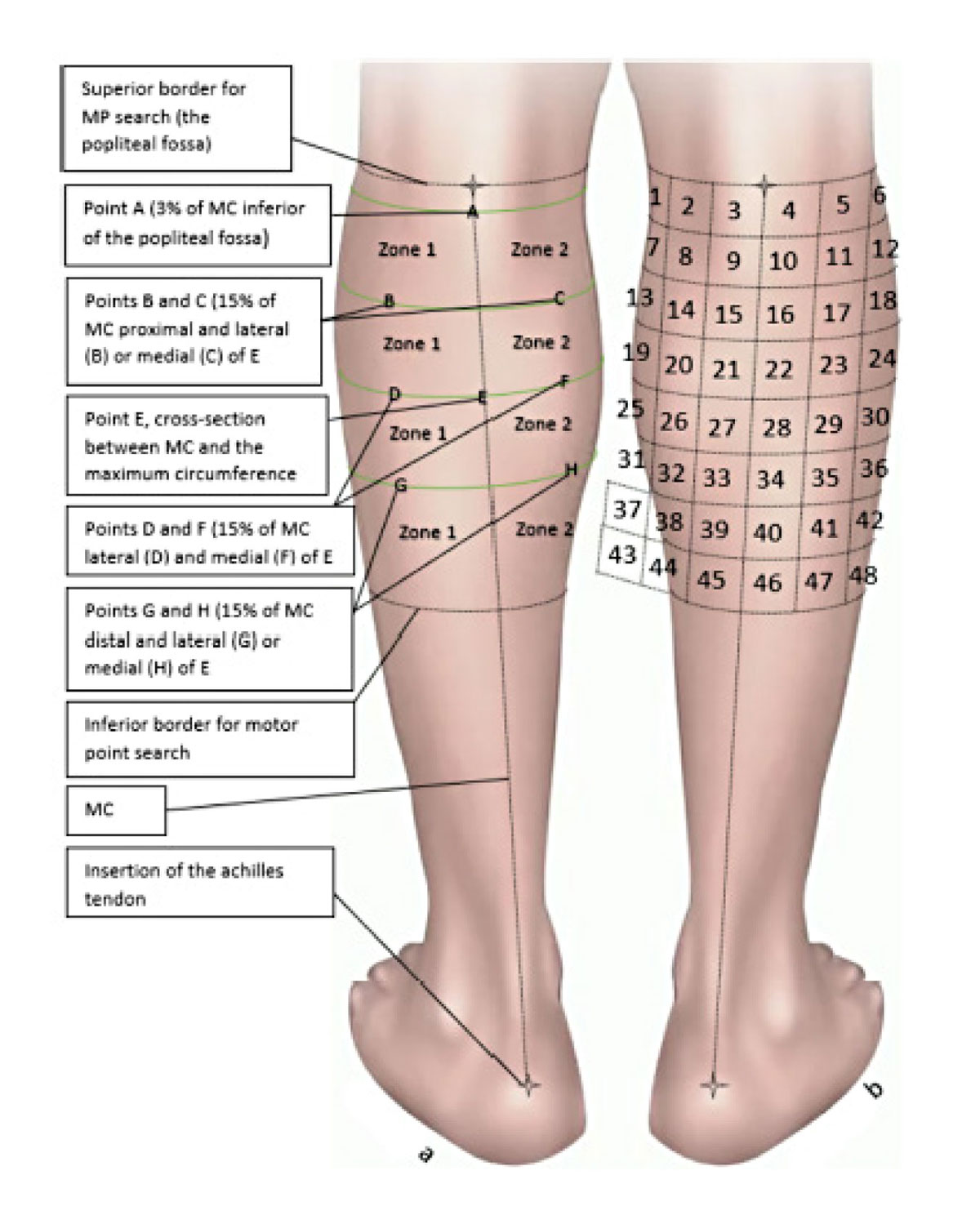
Figure 1: a) Zones and reference locations of the calf. b) Probability zones.
Anatomical landmarks on the lower limbs were defined on 30 healthy participants (mean age 37 years). The test protocol included measurements of the calf and MP scans. The midline of the calf (MC) was defined as the line connecting the center of the fossa poplitea to the calcaneal insertion of the Achilles tendon (Figure 1). The location of the 4 most responsive MPs on the medial and lateral head of the gastrocnemius were determined in relation to these anatomical landmarks using an MP search pen and a pre-set MP search program. The anatomy of the calves was normalized and subdivided into a matrix of 48 (6 × 8) smaller areas (3 × 3cm), from upper medial to lower lateral, in order to calculate the probability of finding an MP in 1 of these areas. The probability of finding an MP was then calculated for each area and presented with a 95% confidence interval.
Results
The MP heatmap displayed a higher concentration of MPs proximally and centrally on the calf. However, there were wide inter-individual differences in the location of the MPs (Figure 2). The highest probability of finding an MP was in area 4, located centrally and medially, and in area 29, located centrolaterally and around the maximum circumference, both with 50% probability (95% CI: 0.31–0.69). The second highest probability of finding MPs was in areas 9, 10, and 16, proximally and medially, all with 47% probability (95% CI: 0.28–0.66). Areas 4, 9, 10, 16, and 29 exhibited a significantly higher probability of finding MPs than all areas with a mean probability of 27% and lower (P < 0.05). The lateral and distal outskirts exhibited almost zero probability of finding MPs.
Discussion
This study demonstrated a pronounced inter-individual variation in the localization of calf muscle MPs. The 2 areas with the highest concentrations of MPs were localized in the midline close to the fossa poplitea and in the proximity of the transverse plane at the maximum circumference of the calf. A computed MP heatmap displayed the probabilities of finding MPs on an anatomical chart, which may guide and help the clinician in daily NMES application.
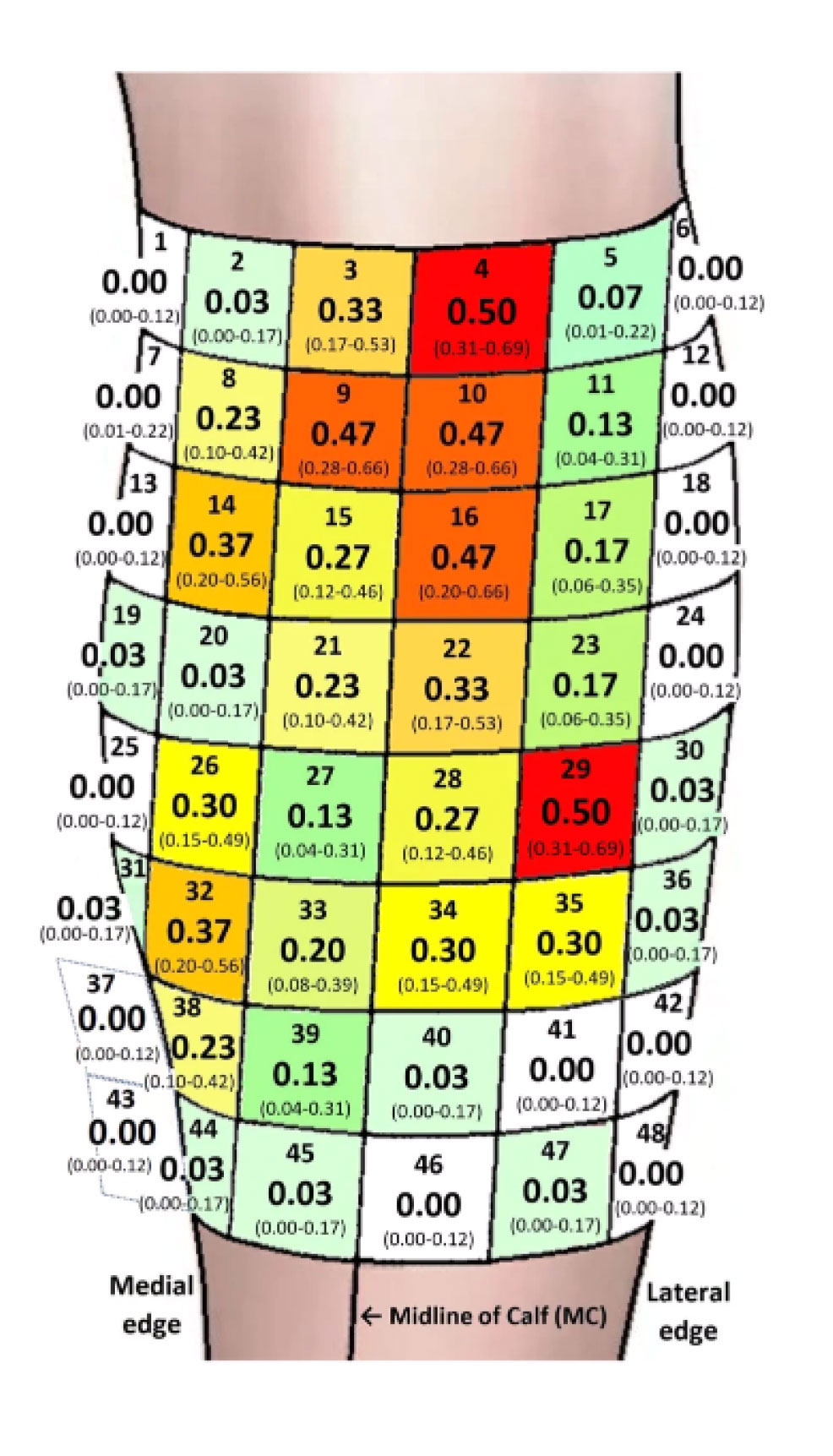
Figure 2: The probability of finding MPs plotted in the areas (1–48), presented with a 95% CI. The dark red areas (4,9,10,16,29) display a statistically significant higher probability of finding MPs compared to the shades of yellow, green and gray/white areas. The orange areas (14,32) display a statistically significant difference compared to the green and grey/white areas. The grey/white areas did not display a MP. MP Motor Point, CI Confidence Interval. Area 1 = medial, proximal. Area 48 = distal, lateral
The prominent inter-individual variability in the anatomical localization of MPs on the calf muscle was the main finding of this study, which suggests that each patient, when possible, should undergo an MP scan before NMES electrodes are applied. The MP heatmap will give suggestions on where to start an MP scan in order to reduce the time of scanning. If an MP scanning device is not available, the heatmap suggests areas to place the electrodes.
The observation of the most distal MP being localized at around 50% length of the calf suggests that clinicians do not have to scan for MPs below the mid of the calf when applying calf NMES. The study authors’ identification of the most medial and lateral MPs both being localized at around 6cm (18%) from the MC implies a further restriction of the search area for the clinician performing the MP scan.
The second main finding of this study was the localization of the 2 areas on the calf that exhibited the highest concentrations of MPs.
Based on the study authors’ main findings, they established a novel MP heatmap displaying the probabilities of finding MPs in 48 predefined, 3 × 3cm areas of the calf. The heatmap displayed that central and proximal areas of the calf showed a much greater probability of containing an MP than the most medial, lateral, and distal areas. The graphical display of the heatmap suggests an anatomical chart, which can be used to search for MPs in a subsequent, logical order.
The observation of areas 4 and 29 demonstrating the highest probability of containing an MP, at 50%, suggests that these areas may be good starting points for the clinician to locate MPs. Area 4, located 0–3cm below the fossa poplitea and just lateral of the midline, and area 29, located 12–15cm below the fossa poplitea at the largest circumference of the calf and 3–6cm lateral of the midline, may be easily identified by the clinician. The finding that areas 4 and 29 exhibited a significantly higher probability of identifying an MP than in 39 of the 48 areas examined on the calf strengthen the observation that these areas are good starting points to look for MPs.
The discovery that areas 9, 10, and 16, which demonstrated the second highest probability of finding an MP (47%), share borders with each other and with area 4 implies how a manual search with MP pens on the calf could be performed. After the search in area 4, the study authors suggest that the search of MPs should continue in a distal and medial direction to area 9, followed by searching laterally toward area 10, subsequently in a distal direction to area 16, then continuing the search distally toward area 29, passing areas 22 and 28 on the way.
Conclusions
This study demonstrated a distinct inter-individual variation in the localization of MPs on the calf muscle. However, certain anatomical patterns of likelihood of where to find MPs seem to repeat among subjects. This MP heatmap of the calf could be used to expedite electrode placement and to improve compliance in order to receive consistent and enhanced results of NMES treatments.
This article has been excerpted from “Motor Point Heatmap of the Calf,” published in the Journal of NeuroEngineering and Rehabilitation. 2023;20:28. https://doi.org/10.1186/s12984-023-01152-5. Editing has occurred, including the renumbering or removal of tables, and references have been removed for brevity. Use is per CC 4.0 International License.





