
By Sofia Ryman Augustsson and Erik Sjöstedt
Chronic ankle instability—a recurring “giving way” of the lateral (outer) side of the ankle causing instability—results from repeated ankle sprains. These authors aimed to find a test battery that could be used easily and could discern true injury in this special population.
 In sports, the ankle has been shown to be one of the most common injured body sites after the knee. Lateral ankle sprain is one of the most common traumatic musculoskeletal injuries and up to 40% develop CAI after this injury. Typically, severe sprains are followed by additional sprains and a feeling of instability, which can then affect range of motion (ROM), muscle strength, and functional performance. ROM is often reduced, perhaps mainly in the acute phase, but it can also be a long-term problem. Both initial and a long-termed reduced muscle strength have been noted, and balance and postural control may be impaired as a result of ankle sprains. Overall, this often affects gait, running, and the ability to land when jumping, and if not managed appropriately, a cascade of negative alterations to both the joint structure and a person’s movement patterns continue to stress the injured ligaments.
In sports, the ankle has been shown to be one of the most common injured body sites after the knee. Lateral ankle sprain is one of the most common traumatic musculoskeletal injuries and up to 40% develop CAI after this injury. Typically, severe sprains are followed by additional sprains and a feeling of instability, which can then affect range of motion (ROM), muscle strength, and functional performance. ROM is often reduced, perhaps mainly in the acute phase, but it can also be a long-term problem. Both initial and a long-termed reduced muscle strength have been noted, and balance and postural control may be impaired as a result of ankle sprains. Overall, this often affects gait, running, and the ability to land when jumping, and if not managed appropriately, a cascade of negative alterations to both the joint structure and a person’s movement patterns continue to stress the injured ligaments.
Common tests to identify possible impaired functions are balance test, strength test, and various forms of jump test. However, studies investigating ankle condition in subjects with CAI using an on-the-field test battery are scarce. Understanding which tests that are most challenging for these subjects has the potential to set realistic goals in rehabilitation and return-to-sports criteria. Thus, the primary aim of this study was to investigate CAI subjects regarding strength, balance, and functional performance with an easily used test battery that required minimal equipment. A second aim was to evaluate which of these tests has the highest ability to discriminate impaired function between the injured and non-injured ankle in CAI subjects.
Methods
This study was conducted with a cross-sectional design. Twenty CAI subjects, engaged in sports, and 15 healthy subjects serving as a control group, were tested for assessment of strength, balance, and functional performance. A test battery was developed accordingly: isometric strength in inversion and eversion, the single leg stance test (SLS), single leg hop for distance (SLHD), and side hop test. The limb symmetry index was calculated to determine whether a side-to-side lower limb difference could be classified as normal or abnormal. The sensitivity of the test battery was also calculated.
Inclusion criteria for the study were men and women with recurrent unilateral ankle problems due to previous sprains, aged 15–40 years, sought treatment on at least 1 occasion for ankle injury and have had a minimum of 3 recurrent sprains in the past year.
Results
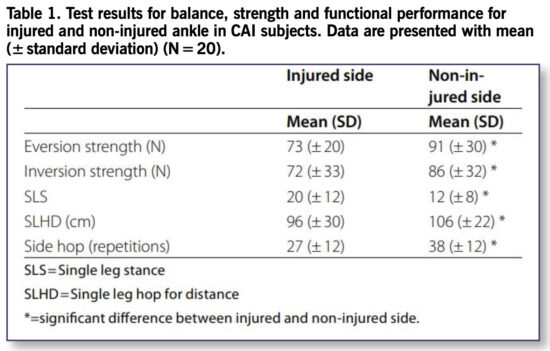
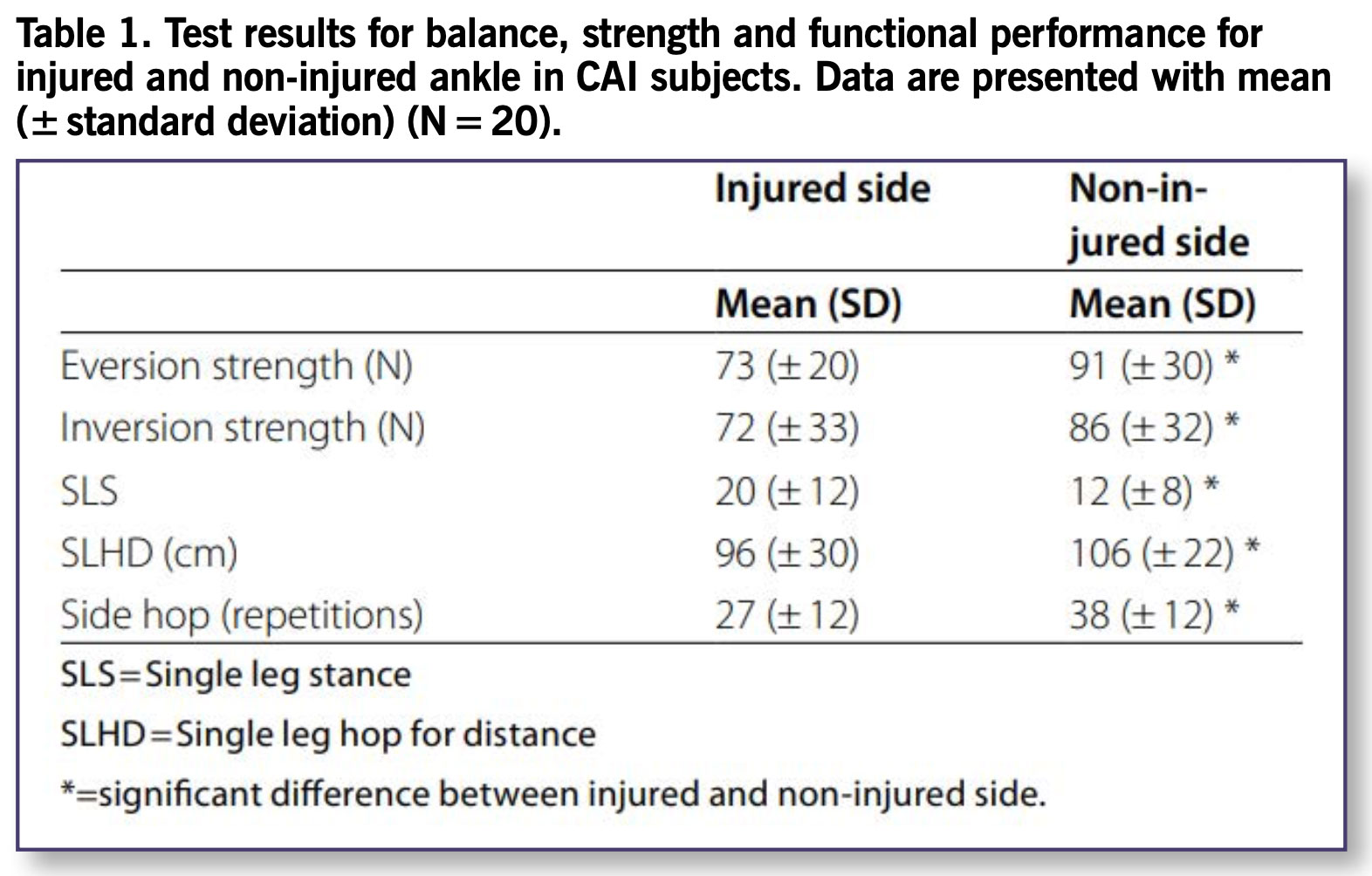
Of the 20 CAI subjects, 10 had right ankle and 10 had left ankle instability. The test battery total score was significantly better for the non-injured compared to the injured ankle (P < 0.01). The subjects were 20% (18 N) weaker on the injured side compared with the non-injured side in eversion (P < 0.01) and 16% (14 N) weaker in inversion (P < 0.01). For the SLS test, the mean score of the injured side was 8 points (67%) higher (more foot lifts) compared to the non-injured side (P < 0.01). The mean distance of the SLHD was 10cm (9%) shorter for the injured side compare to the non-injured side (P = 0.03). The mean number of side hop was 11 repetitions (29%) fewer for the injured side compare to the non-injured side (P < 0.01). (See Table 1.)
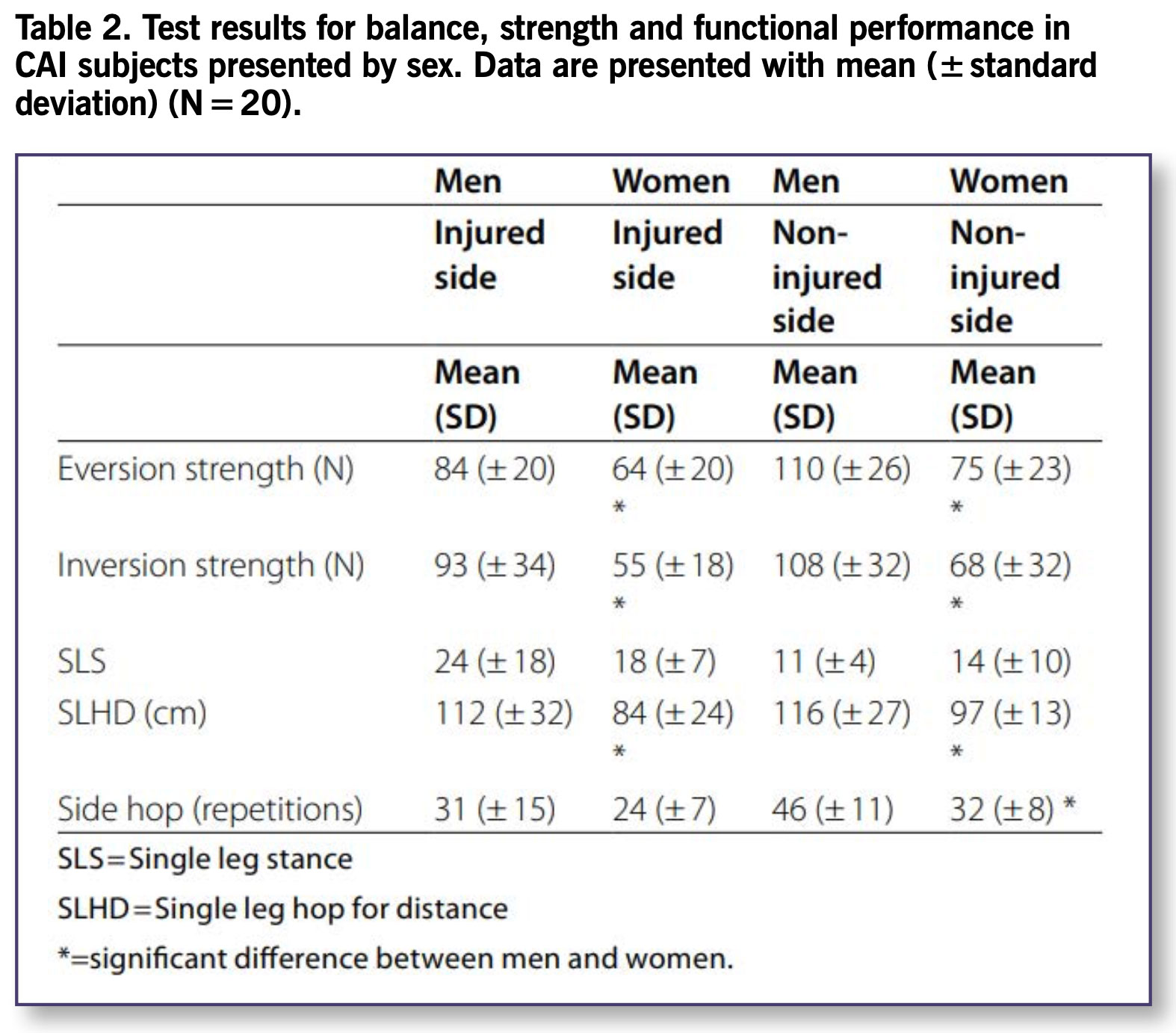
Differences were found between men and women, in favor for the male subjects, in the strength tests and the SLHD (P ≥ 0.04). Men also performed better at the side hop test on the non-injured side (P < 0.0) but not on the injured side (P = 0.22). No differences were found between men and women in the SLS test for either side (P ≥ 0.26). Differences were found between injured and healthy subject in SLS (P = 0.01), SLHD (P < 0.01), and the side hop test (P < 0.01) whereas no differences were found for the strength tests (P ≥ 0.25). (See Table 2)
 Discussion
Discussion
The main observation in this study was that impairments in strength, balance, and functional performance seem to be quite common in CAI subjects. The total score for the test battery was significantly better for the non-injured compared to the injured ankle (P = 0.01). The sensitivity was high for the SLS (100) and the side hop test (85), and thus provides a high ability to discriminate impaired performance between injured and non-injured ankle in CAI subjects. When the 5 tests were combined to produce 1 test battery, a sensitivity of 100% was found.
The CAI subjects in the present study had reduced strength with a 20% difference in eversion and 16% in inversion between injured and non-injured ankle, but strength values did not differ compared to healthy subjects. One plausible explanation for the non-existent difference between CAI and healthy subjects might be the difference in disparity between men and women in the 2 groups. In the group of CAI subjects, 11 (55%) were women whereas there were only 5 women (33%) in the group of healthy subjects. The male subjects were found to be stronger in the strength tests, and these dissimilarities most likely exist in healthy subjects as well.
The sensitivity of the eversion strength test was 65%, with 13 CAI subjects classified as abnormal, whereas the sensitivity of the inversion strength test was 60%. The reduced strength in inversion noted in this study is in accordance with the outcome from an earlier study. Thus, reduced strength seems to be present in CAI subjects, suggesting that continued strength training after rehabilitation is probably important to reduce the risk of re-injury. In addition, the result from this study suggests that isometric testing can detect strength deficits in CAI subjects and should be recommended for clinical use.
 In this study, CAI subjects performed significantly worse at the balance test on the injured side. The differences of 67% in the SLS and the test sensitivity of 100% noted in this study between the injured and non-injured ankle suggests that evaluation of balance is of utter importance in this group of subjects and that rehabilitation should aim to improve balance ability.
In this study, CAI subjects performed significantly worse at the balance test on the injured side. The differences of 67% in the SLS and the test sensitivity of 100% noted in this study between the injured and non-injured ankle suggests that evaluation of balance is of utter importance in this group of subjects and that rehabilitation should aim to improve balance ability.
Impairments in functional performance were also noted for the CAI subjects in the present study. There was a 29% difference, with 11 repetitions fewer in the side hop test on the injured side. Seventeen of the 20 CAI subjects were classified as abnormal giving the test a sensitivity of 85%. The mean distance of the SLHD was 10cm (9%) shorter for the injured side compared to the non-injured side (P = 0.050). However, the sensitivity of the SLHD in this study was only 45% and only 9 of the 20 CAI subjects were classified as abnormal. Thus, the deficits in SLHD performance could be considered as minor compared to the side hop performance and strength impairments. This study confirms that a SLHD does not appear to be as challenging as other functional tests such as the side hop test.
Not surprisingly, there was a relatively strong correlation between the 2 strength tests (rs=0.73) and a moderate correlation between the 2 hop tests (SLHD and side hop) (rs=0.49). Moderate correlations were also noted between the strength tests and the side hop test (eversion, rs=0.59, R2 = 0.35 and inversion rs=0.56, R2 = 0.31) and the SLHD (eversion, rs=0.51, R2 = 0.26, inversion, rs=0.45, R2 = 0.20) suggesting that maximum muscle strength has an impact on functional performance in this group of subjects.
Correlations could not be found between the balance test and any of the other parameters in this study (P ≥ 0.48). However, the absence of a correlation between ankle strength and balance has previous been demonstrated in healthy individuals. Assessment of muscle strength was carried out isometrically, which may not provide necessary information regarding the nature of a balance test. One previous study revealed that strength training increased strength in subjects with functional ankle instability but did not improve proprioception. Thus, other factors than muscle strength may be of more importance for balance performance in CAI subjects. However, this does not explain the absence of correlations between the balance test and the tests of functional performance.
Conclusion
Deficits in muscle strength, balance, and functional performance appear to be present in CAI subjects with the largest impairments in balance, side hop performance, and eversion strength, which stresses the need for better return-to-sport criteria for this group of subjects. The findings also indicate that the SLHD test does not seem to be sufficiently challenging when it comes to evaluating functional performance in CAI subjects, whereas the more challenging method of the side hop test used in this study could be recommended. The SLS, inversion and eversion strength tests, and the side hop test had high ability to discriminate performance between the injured and the non-injured ankle in CAI subjects.
This article has been excerpted from “A Test Battery for Evaluation of Muscle Strength, Balance and Functional Performance in Subjects with Chronic Ankle Instability: A Cross-Sectional Study,” BMC Sports Science, Medicine and Rehabilitation. 2023;15(1):55. (2023). Doi: 10.1186/s13102-023-00669-5. Editing has occurred, including the renumbering or removal of tables, and references have been removed for brevity. Use is per CC BY 4.0 International License.





