 By Robert Conenello, DPM, FACFAS
By Robert Conenello, DPM, FACFAS
We all know that several of the things we’ve been doing for years to treat plantar warts are just not that effective. It’s frustrating for the patients and it’s frustrating for us as clinicians. So we have to think outside the box.
And that’s what got me interested in learning more about microwave therapy for this everyday condition that we don’t have a successful treatment for…or at least we didn’t.
What Is Microwave Therapy?
Microwave therapy is a type of electromagnetic energy that induces a thermal response—both in food and in humans. When you compare the therapeutic microwave we’re using in the office, its energy output – 8GHz Power: 8W – is closer to a mobile phone (GSM 0.8 – 1.9GHz Power: 2W) than a kitchen microwave
(2.45GHz Power: 1000W). So, if you want to explain it to a patient, you could say it’s more like putting your foot next to your mobile phone than it is actually putting your foot in a microwave, which many people think we’re going to be doing when we first discuss this therapy with them.
 This is a rapid, in-office treatment that doesn’t use a lot of bandages or other supplies. It’s quick and easy to learn. Microwave therapy works by rapidly elevating tissue temperature into the hyperthermic range; it heats it up, but doesn’t destroy it like ablation. Microwaving these tissues leads to a cascade of immune system responses that create the heat shock protein [for details on heat shock protein, see Pediatric Cutaneous Warts and Verrucae: An Update on page 35]. That heat shock protein increases the release of interferon. So using the microwave basically allows the natural immune system to do what it’s supposed to do.
This is a rapid, in-office treatment that doesn’t use a lot of bandages or other supplies. It’s quick and easy to learn. Microwave therapy works by rapidly elevating tissue temperature into the hyperthermic range; it heats it up, but doesn’t destroy it like ablation. Microwaving these tissues leads to a cascade of immune system responses that create the heat shock protein [for details on heat shock protein, see Pediatric Cutaneous Warts and Verrucae: An Update on page 35]. That heat shock protein increases the release of interferon. So using the microwave basically allows the natural immune system to do what it’s supposed to do.
I did a small study with my own patients and found that on average, it took 2.4 treatments (typically, 1 treatment = 5 doses/2 seconds each delivered about a month apart) for the lesions to resolve. Some lesions were going away after 1 treatment, some were taking 3 or more. It didn’t seem to matter if the patients were treatment naïve or had failed several other therapies previously. What we did find was a link with the age of the lesions: The longer the lesion had been around, the longer it took to get rid of it.
My study included 59 patients, with an average age of 24 years, but we included kids and even some who were close to 80 years old. Again, there was no difference in terms of getting rid of the lesions. Same with sex of the patient, it was pretty much equal across the board.
Another interesting finding was that this group overall said they started feeling better after the very first treatment—and this was an active population, a lot of runners.
 Key finding from the study is that out of 59 patients, we saw 87.8% clearance rate with the microwave treatment. Compare that to 30% effectiveness of what we had been doing before.
Key finding from the study is that out of 59 patients, we saw 87.8% clearance rate with the microwave treatment. Compare that to 30% effectiveness of what we had been doing before.
Case Studies
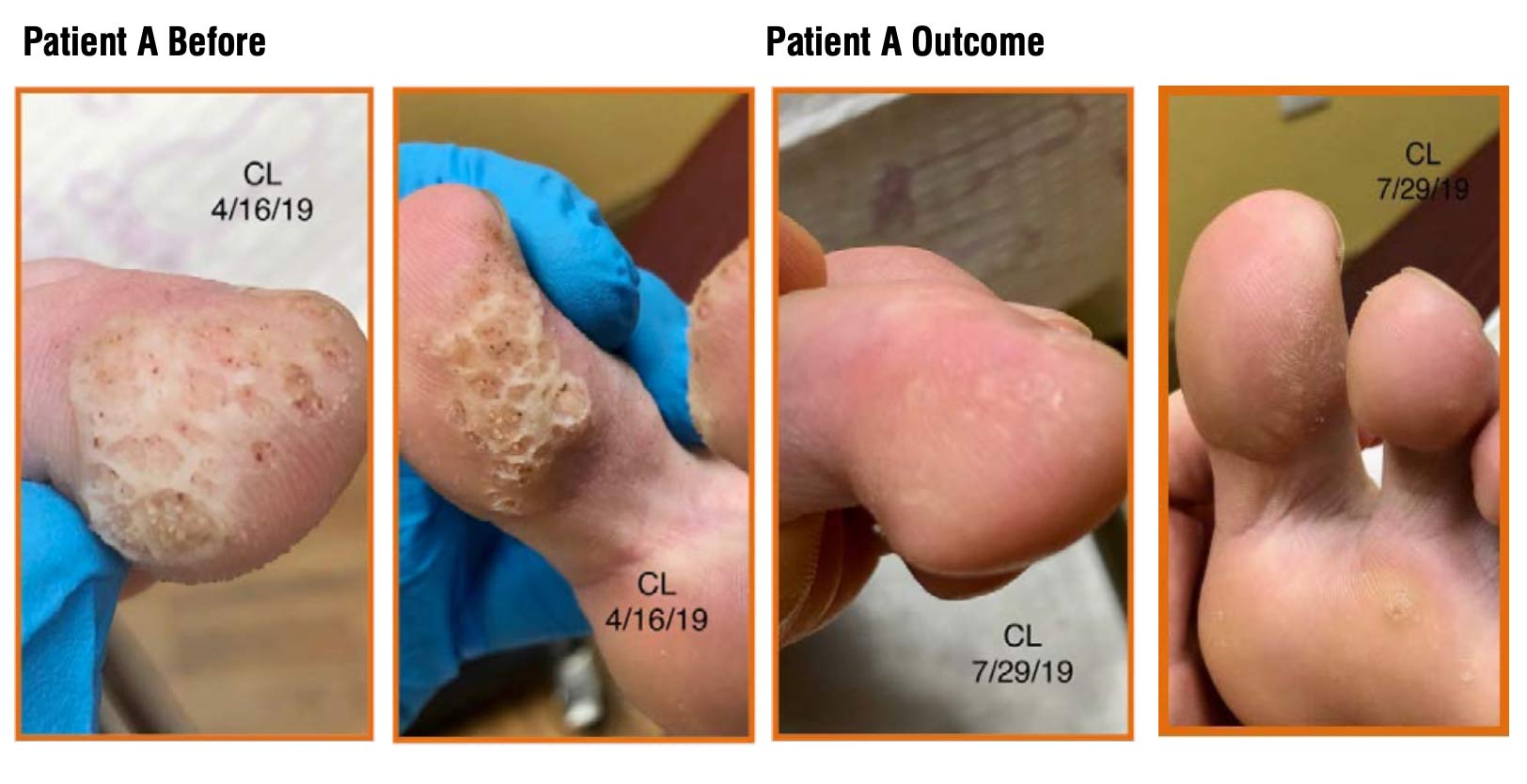
Patient A was a 14-year-old male with a 3-year history of mosaic lesions on both feet. We saw him every 2/3 weeks for 1 year and tried salicylic acid (SA), cryotherapy, and imiquimod. His reported pain level was 1/10.
We did 2 microwave treatments and he reported resolution at 12 weeks.
Patient B was a 46-year-old male with a 4-week history of lesion to left second digit. He’s a physical therapist in general good health and an avid runner. Previous treatments included SA and home cryotherapy. His pain level was 5/10.
We did 1 treatment with a Microwave Dose: 6 watts for 2 seconds x 5. He reported no pain 1 week after the treatment.
Patient C was an 8-year-old healthy female, level 5 gymnast. She had a 3-month history of 15 lesions (8 on the left, 7 on the right). She reported a pain level of 6/10 while on the balance beam and tumbling. Previous treatment had been Compound W.
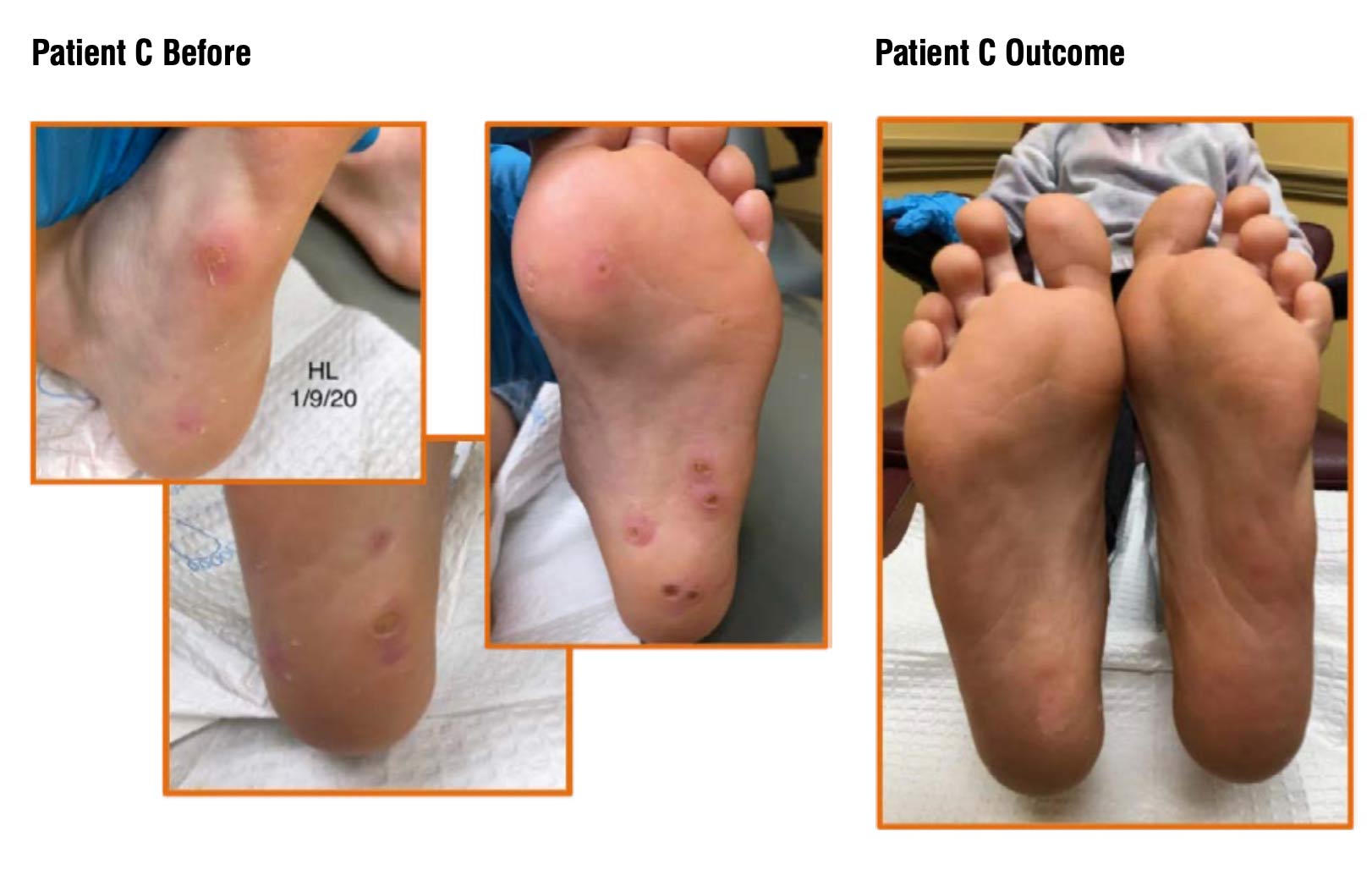 Her microwave dose was 8 watts at 2 seconds x 5. She reported complete resolution at 8 weeks.
Her microwave dose was 8 watts at 2 seconds x 5. She reported complete resolution at 8 weeks.
Robert Conenello, DPM, FACFAS, is the owner of Orangetown Podiatry in xxxx New York, where he’s been a practicing podiatrist for more than 20 years. He is also a member of the Lower Extremity Review Editorial Advisory Board. He discloses that he is a compensated clinical consultant for Saorsa, Inc., maker of the Swift product discussed here.
To Learn More… Visit lerEXPO.com
This article is excerpted from an lerEXPO.com event. To hear Dr. Conenello discuss his study in further detail and provide other case studies, visit lerEXPO.com: go to Events; click on past events and scroll down to New Frontiers in Dermatology: Warts, IPKs & Microwave Therapy, sponsored by Swift. There you’ll find not only Dr. Conenello’s talk, but also “Warts: Condition Profile,” by Tracy Vlahovic, DPM, FFPM, FCPS (Glasg), in which she explores the condition profile for warts and what makes HPV such a challenging virus to treat effectively and with consistency. This program, including a detailed discussion by Ivan Bristow, PhD, FFPM, RCPS (Glasg), on his study using microwave therapy in pediatric cutaneous warts and verrucae, is approved for 2.0 CME.






