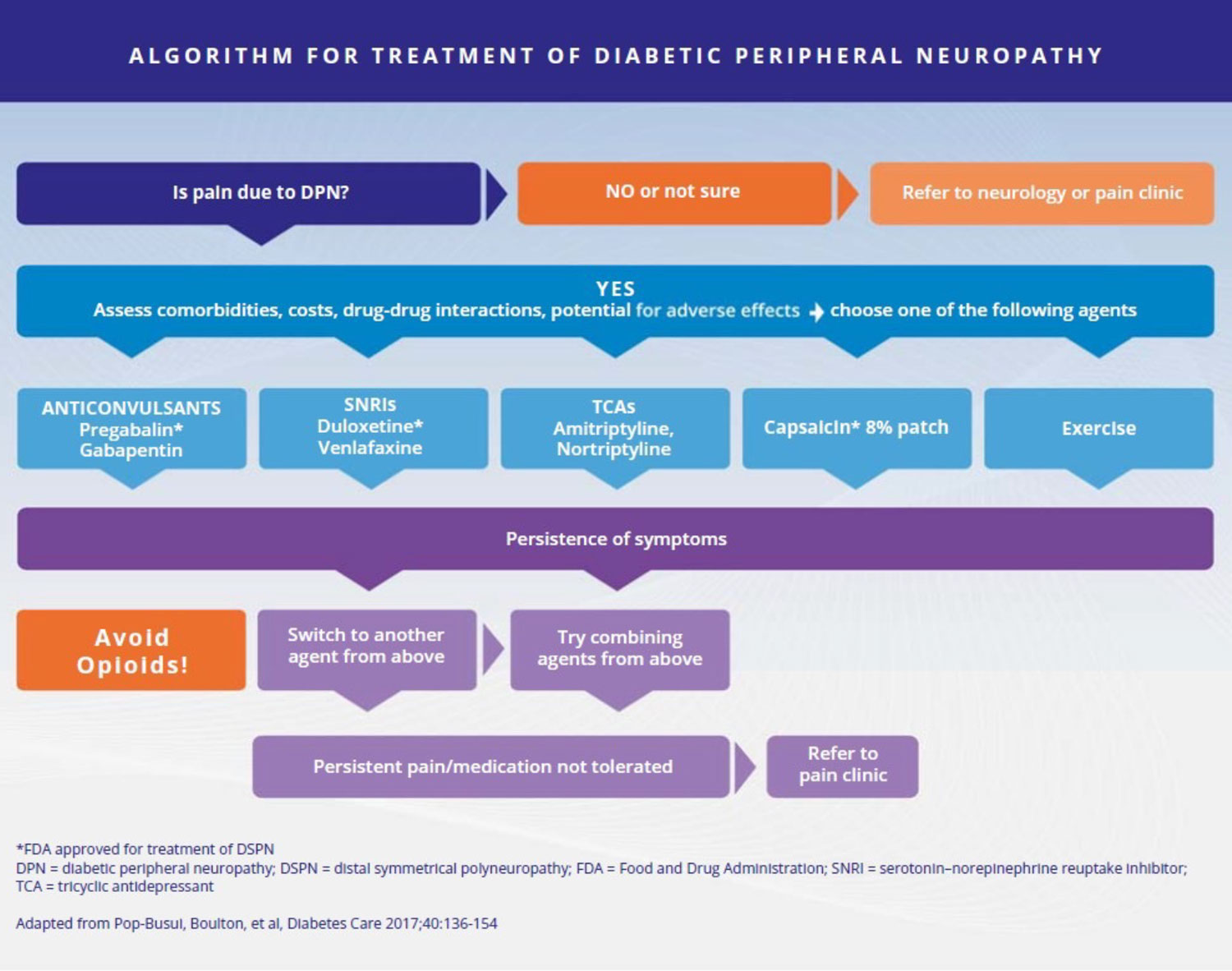
 Despite major advances in elucidating the pathogenesis of diabetic peripheral neuropathy (DPN), there remains a lack of disease-modifying treatment options in individuals with diabetes. Currently, there is no convincing evidence supporting glucose control or lifestyle management as therapies for neuropathic pain in diabetes or prediabetes. At present, among pharmacological options, pregabalin and duloxetine are oral agents that have received regulatory approval from FDA for the treatment of neuropathic pain associated with DPN and are effective for DPN pain reduction when using patient-reported outcomes. In addition, based on evidence from 2 large 12-week randomized multicenter trials in 2020, the FDA approved the cutaneous concentrated capsaicin 8% patch that works by desensitizing and interfering with the function of the transient receptor potential vanilloid 1 receptor, a protein involved in pain signaling. However, the patch needs to be applied for ~30 minutes and can be done only in the office with a physician present. The opioid, tapentadol, has received regulatory approval in the United States and Canada, but evidence for its use is, at best, inconclusive, and the American Diabetes Association and other organizations strongly recommend against using any opioids for management of DPN pain. Reviewing evidence for the variety of agents that can modify DPN pain, one should use a stepwise approach and consider an individual’s comorbidities, socioeconomic status, and potential drug interactions. Nonsteroidal anti-inflammatory agents should be avoided for chronic pain management in persons with diabetes due to adverse kidney effects. Given the high risk of addiction, abuse, sedation, and other complications and psychosocial issues, even with short-term opioid use, opioids are not recommended in the treatment of painful DPN. High frequency (eg, 10 kHz) spinal cord stimulation is a nonpharmacological approach that may be effective in persons with painful DPN that failed at least 1 medication, as suggested by a recent large RCT, leading to FDA approval in 2021 (See algorithm, page 13).
Despite major advances in elucidating the pathogenesis of diabetic peripheral neuropathy (DPN), there remains a lack of disease-modifying treatment options in individuals with diabetes. Currently, there is no convincing evidence supporting glucose control or lifestyle management as therapies for neuropathic pain in diabetes or prediabetes. At present, among pharmacological options, pregabalin and duloxetine are oral agents that have received regulatory approval from FDA for the treatment of neuropathic pain associated with DPN and are effective for DPN pain reduction when using patient-reported outcomes. In addition, based on evidence from 2 large 12-week randomized multicenter trials in 2020, the FDA approved the cutaneous concentrated capsaicin 8% patch that works by desensitizing and interfering with the function of the transient receptor potential vanilloid 1 receptor, a protein involved in pain signaling. However, the patch needs to be applied for ~30 minutes and can be done only in the office with a physician present. The opioid, tapentadol, has received regulatory approval in the United States and Canada, but evidence for its use is, at best, inconclusive, and the American Diabetes Association and other organizations strongly recommend against using any opioids for management of DPN pain. Reviewing evidence for the variety of agents that can modify DPN pain, one should use a stepwise approach and consider an individual’s comorbidities, socioeconomic status, and potential drug interactions. Nonsteroidal anti-inflammatory agents should be avoided for chronic pain management in persons with diabetes due to adverse kidney effects. Given the high risk of addiction, abuse, sedation, and other complications and psychosocial issues, even with short-term opioid use, opioids are not recommended in the treatment of painful DPN. High frequency (eg, 10 kHz) spinal cord stimulation is a nonpharmacological approach that may be effective in persons with painful DPN that failed at least 1 medication, as suggested by a recent large RCT, leading to FDA approval in 2021 (See algorithm, page 13).
Regular aerobic, strengthening, and balance exercise, alone or in combination; reduction of sedentary behavior; and dietary modification aimed at reducing calorie intake and increasing plant-based foods and polyunsaturated fats have all demonstrated positive outcomes for individuals with DPN, including for neuropathic pain reduction. Small-fiber neuropathies should be managed with foot protection (eg, padded socks); supportive shoes with orthotics, if necessary; regular foot and shoe inspection; prevention of heat injury; and use of emollient creams. Regular foot and nail care by a trained professional is recommended. Advanced stages of large-fiber neuropathies may require a multidisciplinary approach to include strategies to enhance muscle strength, gait, and balance training; titrate any pain or other medications that could promote dizziness and other side effects affecting gait and balance; orthotics to treat and prevent foot deformities; tendon lengthening for pes equinus from Achilles tendon shortening; and/or surgical reconstruction in case of deformities.
Source: Blonde L, Umpierrez GE, Reddy SS, et al. American Association of Clinical Endocrinology Clinical Practice Guideline: Developing a Diabetes Mellitus Comprehensive Care Plan-2022 Update. Endocr Pract. 2022;28(10):923-1049. doi: 10.1016/j.eprac.2022.08.002.