 First law of motion: objects in motion stay in motion. Sir Isaac Newton
First law of motion: objects in motion stay in motion. Sir Isaac Newton
By Dylan Morrissey, Matthew Cotchett, Ahmed Said J’Bari, Trevor Prior, Ian B Griffiths, Michael Skovdal Rathleff, Halime Gulle, Bill Vicenzino, Christian J Barton
Plantar heel pain (PHP) is common and can have a negative impact on physical and mental health. Despite this prevalence, existing guidelines lack clear, high-quality recommendations for treating people with this condition. The question then is, how should clinicians treat pain and improve function in people with PHP? The authors set out to answer this question by developing a best practice guide (BPG) for the management of PHP.
Methods & Results
The authors synthesized high-quality randomized controlled trials (RCTs), elicited expert clinical reasoning, and surveyed patients to produce this BPG.
Of the 51 trials included in the review, 8 RCTs of 9 interventions could be considered for primary proof of efficacy. The 9 interventions included radial extracorporeal shockwave therapy (ESWT), focused ESWT, custom foot orthoses, prefabricated foot orthoses, dry needling, magnetized insoles, calf stretching, foot taping, and wheatgrass cream.
Forty people with PHP completed the online survey and 14 experts were interviewed resulting in 7 themes and 38 subthemes. There was good agreement between the systematic review findings and interview data about taping and plantar fascia stretching for first step pain in the short term. Clinical reasoning advocated combining these interventions with education and footwear advice as the core self-management approach. There was good expert agreement with systematic review findings recommending stepped care management with focused shockwave for first step pain in the short term, medium term, and long term and radial shockwave for first step pain in the short term and long term. Good agreement was also found to ‘step care’ using custom foot orthoses for general pain in the short term and medium term.
The synthesis of this quantitative (review) and qualitative (expert interviews and patient survey) data led to the development of a core approach for people with PHP. The core approach consists of the best evidence-based interventions of plantar fascia stretching and low dye taping complemented by an individualized education approach. All recommended core approach components should be used simultaneously for about 4–6 weeks before consideration of adjunctive interventions such as ESWT or orthoses. Expert interviews strongly emphasized the need to implement this education and self-management approach prior to applying the interventions identified to have strong evidence when pain remains unchanged from baseline. The timelines were derived from the qualitative components and reflect the time required for someone to respond to the core approach, but recognize a need to adjust these timelines based on individual circumstances.
Discussion
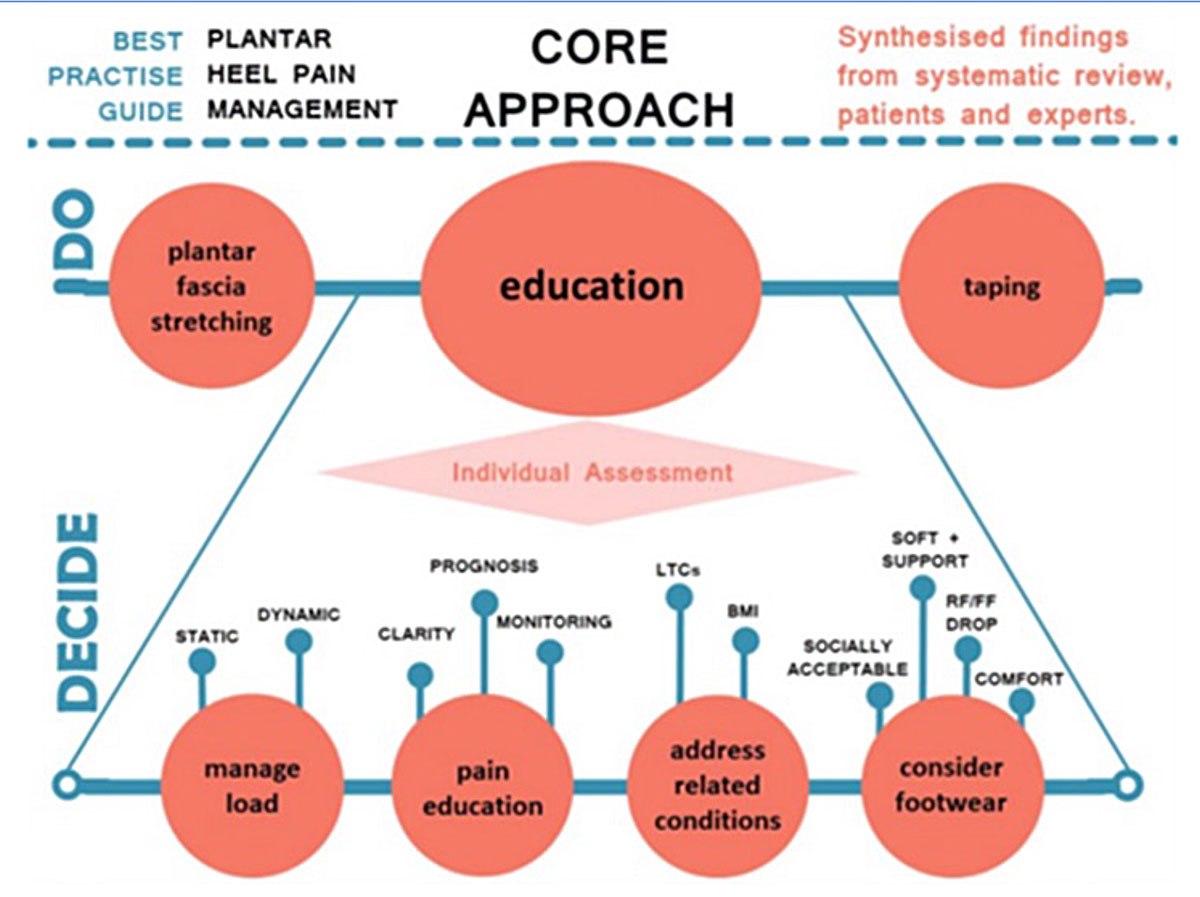
Figure. Core approach to the management of plantar heel pain based on the best available evidence, expert opinion and the patient voice. The top layer (“DO”) of tapin, stretching and education are required initial interventions with each patient. The individual assessment (“DECIDE”) is of which specific educational aspects are needed. BMI, body mass index; FF, forefoot; LTC, long-term conditions; RF, rearfoot.
The BPG defines a core approach (Figure) to management, which consists of supported self-management interventions of plantar fascia stretching and taping (labelled ‘DO’ in the figure) to support the plantar fascia, alongside less well-defined educational interventions (labelled ‘DECIDE’ in the figure). The expert interviews indicated that education should adopt a realistic tone as recovery may take several weeks or months but stress the positive prognosis, and gave clear direction that this education should encourage: individual assessment; footwear advice to ensure comfort in shoes that allow a small rearfoot to forefoot drop while also considering social acceptability to improve adherence; load management to break up long periods of static loading or problematically rapid training changes in more athletic populations; support to address comorbidities such as type 2 diabetes; teaching patients the parameters required to self-monitor the pain response to activity and how to interpret pain with respect to tissue damage in order to allay fears of long-term consequences.
The systematic review showed ESWT had the best evidence of any adjunctive treatments, demonstrating positive efficacy in the short-, medium-, and long-term. It is typically used for people with non-resolving, persistent symptoms. As ESWT is inferior to stretching for acute symptoms, it is recommended when patients are failing to recover optimally using the core approach. Focused shock wave is applied so that the peak intensity is deep to the skin thus being targeted directly at the lesion and RCTs showed moderate positive short-term findings on pain of large effect. Radial ESWT results in peak intensity at the surface and showed moderate positive effects, again of large effect at all time points for patient-reported outcomes.
Other options are available for those patients who do not respond to core treatment or ESWT. Custom orthoses can be considered based on positive evidence of moderate strength and lower effect size than ESWT for short-term outcomes. This progression is extrapolated from expert interviews and systematic review findings. Prefabricated or custom orthoses are often prescribed for PHP. However, none of the trials included in this review used the same orthosis. All differed in the prescription process, casting technique, shell material, top-covers, and modifications, thus limiting trial comparison. The prescription of foot orthoses in clinical practice, whether customized or prefabricated, commonly involves a process of both education and orthosis modification to optimize the dose and biomechanics. No included RCTs followed this process, possibly limiting efficacy of orthoses. Furthermore, prefabricated orthoses, as used in the included trials, were shown to be ineffective. Therefore, it can be recommended that a single orthosis prescription is not used for all presenting patients, an assertion supported by expert opinion in this study. Given the contrast with custom orthoses, it may be that having a range of prefabricated orthoses may be a suitable strategy so that prescription can be individualized. This approach would be a priority for future cost-effectiveness trials, given the lower cost compared with casting or scanning.
Dry needling had a positive effect on pain and function in the short term. One study showed that dry needling can be considered to have neutral evidence of effect but could be considered as an adjunct intervention to the core approach, with lower priority than orthoses. Trigger point dry needling is also associated with minor adverse events such as needle site pain and to a lesser extent minor bruising. Findings from the interviews indicated that dry needling is not a first-line treatment but may be considered to influence pain and muscle tension when combined with other interventions.
Corticosteroid and platelet-rich plasma injection therapy was carefully assessed, both in the trials and the semi-structured interviews as this is a commonly used intervention. However, no such RCTs have been performed. This is an intervention for which placebo control is readily achievable and represents a priority for future research—perhaps in patients where ESWT has failed to yield optimal results.
Resistance exercises of the affected area and limb are often effective as part of first-line care for chronic musculoskeletal problems such as osteoarthritis of the hip or knee and common tendinopathies. While there is moderate evidence for stretching the plantar fascia, the authors’ systematic review could not identify evidence in favor of more comprehensive exercise approaches. Furthermore, the expert interviews did not provide a theme on hidden efficacy and was divided on whether such resistance exercises are useful or not.
Information obtained from the 3 methods used to formulate the BPG was generally consistent. For example, the need for positivity when discussing prognosis was expressed by experts and mirrored in the patient survey responses. Furthermore, there was strong agreement between the patient survey findings and the content of the core intervention while expert interviews and the systematic literature review were in agreement about the efficacy of the various interventions. The agreement was also good where the published evidence was unclear. For example, there is an absence of high-quality trials of progressive strengthening while the expert interviews showed very divergent views on likely efficacy.
Taking into consideration each patient’s past treatment history and experience, the BPG can guide patients and clinicians. It can also inform future research. Patients having access to summary resources such as figure 2 should reduce some of the inconsistency they report when seeking guidance from internet and other resources.
Home-Based Stretching Effective for Plantar Fasciitis
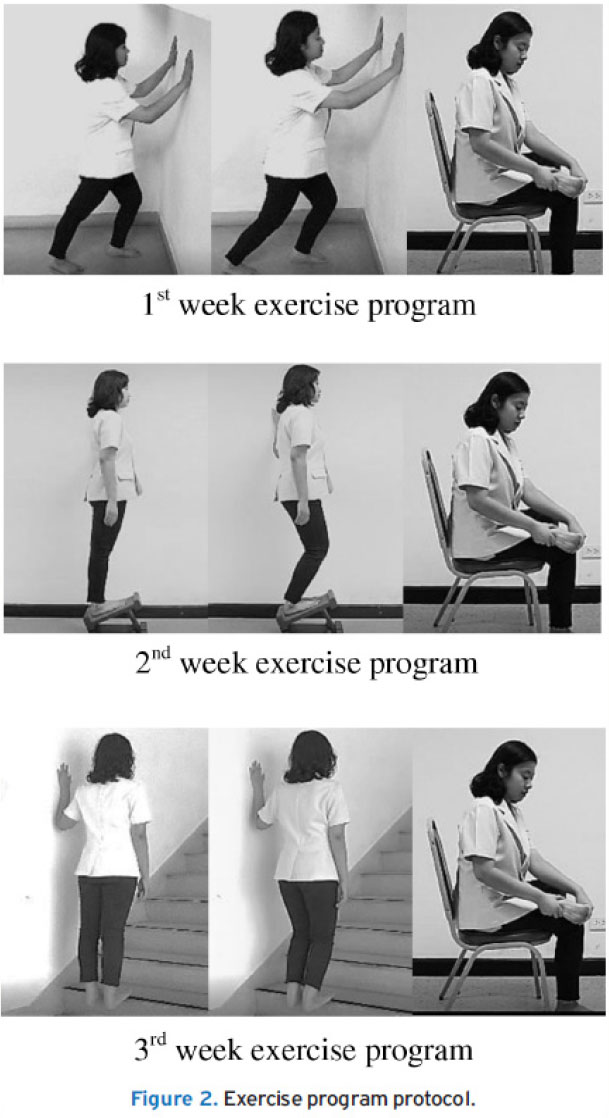 A 2020 study from Thailand found a 3-week home-based stretching program was effective for patients with plantar fasciitis. The exercise program was a home-based stretching exercise for calf and plantar fascia that patients could perform by themselves; it was progressed by week (Figure). To ensure the patients were able to follow the program properly, a physiotherapist taught the exercise program until they remembered and were able to exercise on their own accurately. Patients also received both handbook and video clips of the exercises for use via smartphone. In addition, the researcher reminded them to follow the exercise twice a week by Line chat or telephone. Participants were re-checked and were assigned more progressively of exercise after the 5th day and 10th day of the intervention program.
A 2020 study from Thailand found a 3-week home-based stretching program was effective for patients with plantar fasciitis. The exercise program was a home-based stretching exercise for calf and plantar fascia that patients could perform by themselves; it was progressed by week (Figure). To ensure the patients were able to follow the program properly, a physiotherapist taught the exercise program until they remembered and were able to exercise on their own accurately. Patients also received both handbook and video clips of the exercises for use via smartphone. In addition, the researcher reminded them to follow the exercise twice a week by Line chat or telephone. Participants were re-checked and were assigned more progressively of exercise after the 5th day and 10th day of the intervention program.
The exercises consisted of gastrocnemius, soleus, and plantar fascia stretching. Duration for each stretching exercise was 20-30 sec, resting between exercises for 10 sec, and doing each exercise for 10 sets. Patients spent a total time for the exercise around 20 minutes per day, 5 days per week over the duration of 3 weeks.
The authors concluded that this program was effective for reducing pain, enhancing function and muscle strengths of the ankle plantarflexors, invertors, evertors, great toe flexors, and less toe flexors in patients with plantar fasciitis.
Source: Boonchum H, Bovonsunthonchai S, Sinsurin K, Kunanusornchai W. Effect of a home-based stretching exercise on multi-segmental foot motion and clinical outcomes in patients with plantar fasciitis. J Musculoskelet Neuronal Interact. 2020;20(3):411-420.
This article has been excerpted from “Management of plantar heel pain: a best practice guide informed by a systematic review, expert clinical reasoning and patient values” by the authors noted above, which was published in the British Journal of Sports Medicine. 2021;55:1106–1118. doi: 10.1136/bjsports-2019-101970. Editing has occurred, including the renumbering of tables, and references have been removed for brevity. Use is per CC BY 4.0.





