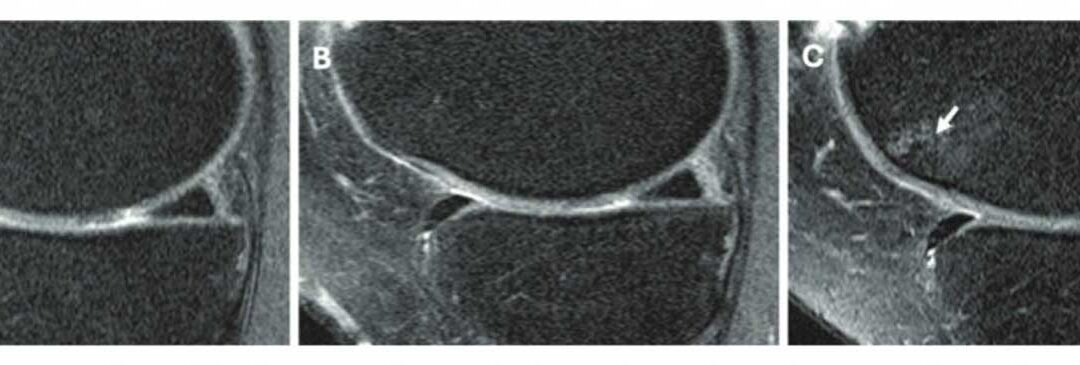
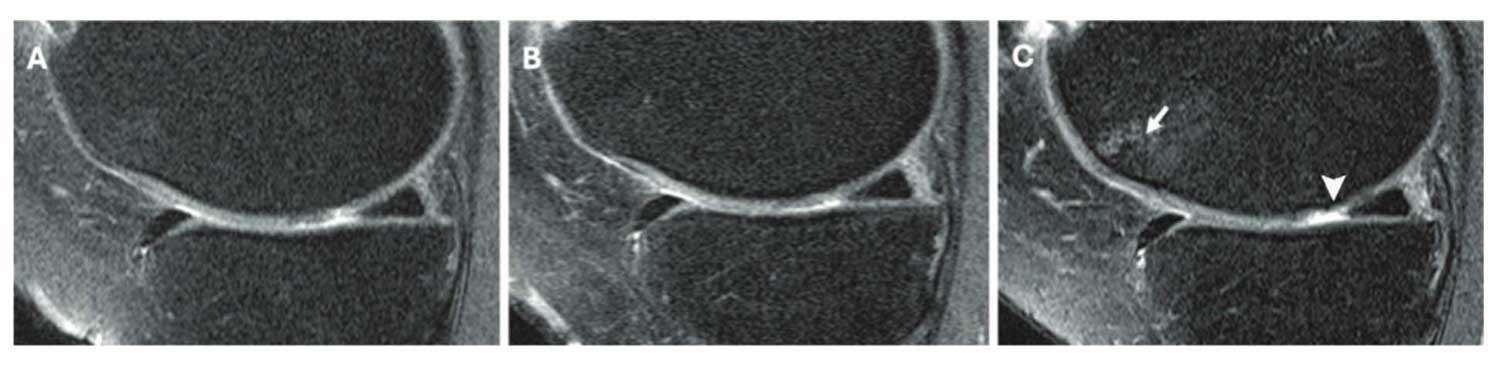
Figure. Knee MRI scans in a 58-year-old female participant in the Osteoarthritis Initiative who was administered a corticosteroid injection. Sagittal intermediate-weighted images obtained (A) 2 years before injection, (B) at the time of injection, and (C) 2 years after injection show a focus on the medial femoral cartilage and trochlea. (C) The postin-jection scan shows a new full-thickness cartilage lesion in the medial femoral cartilage (arrowhead), whereas images from the preinjection time points show a well-preserved medial femoral cartilage (A, B). The postinjection scan (C) also shows the development of a new full-thickness cartilage lesion in the medial femoral cartilage and a new bone marrow lesion in the trochlea (arrow), both of which were absent in the preinjection scans. These findings suggest structural deterioration following the corticosteroid injection.
At least 10% of all patients with knee osteoarthritis (OA) undergo treatment with injectable corticosteroids or hyaluronic acid (HA). Although both have been shown to help with symptomatic pain relief, their long-term effects on knee OA progression remain inconclusive. The overall aim of this study was to investigate the association between intra-articular knee injections, specifically with corticosteroids and HA, and the progression of knee OA using a detailed whole-joint semiquantitative MRI evaluation and clinical outcomes for a period of 2 years.
This secondary analysis uses data from the Osteoarthritis Initiative (OAI), a multicenter, longitudinal, prospective study (February 2004 to January 2015). Participants who received a reported injection of corticosteroid or HA and propensity-score–matched controls (on age, sex, body mass index, and clinical variables) were analyzed. Using the Whole-Organ MRI Score (WORMS) system for cartilage, bone marrow lesions, and meniscus, 3-T MRI performed at the time of injection, 2 years prior, and 2 years after were semiquantitatively graded. Postinjection progression was quantified using WORMS difference between time of injection and the 2-year follow-up. Associations with injection type were analyzed using repeated measures of analysis of covariance.
There were 210 participants analyzed (mean age, 64 years ± 7.9 years [SD]; 126 female). Corticosteroids were associated with greater WORMS progression compared with controls (mean difference, 0.39; 95% CI: 0.05, 0.75; P = .02) and HA (0.42; 95% CI: 0.01, 0.84; P = .04). HA was associated with decreased WORMS progression compared with the injection-concurrent time frame (mean difference, −0.42; 95% CI: −1.34, −0.28; P = .003). Both corticosteroids (mean difference in Western Ontario and McMaster Universities Osteoarthritis Index scores, −5.20; 95% CI: −6.91, −3.48; P = .001) and HA injections (−2.15; 95% CI: −4.42, −0.13; P = .04) were associated with reduced pain after injection.
Corticosteroid injections were associated with higher OA progression than HA injections and controls, whereas HA was associated with decreased progression at MRI for up to 2 years after injection.
Source: Bharadwaj UU, Lynch JA, Joseph GB, et al. Intra-articular knee injections and progression of knee osteoarthritis: data from the osteoarthritis initiative. Radiology. 2025;315(2):e233081. doi: 10.1148/radiol.233081.





