
CAGA 101: The 12 Dirty Truths of Foot Mechanics

Figure 1: Joint subluxation with asymmetric narrowing.
By Jay Segel, DPM; Sally Crawford, MS
Our linear mechanical degradation equation, outlined in our last installment, highlighted the challenges to the kinetic chain during weightbearing and locomotion. It displays the all too real journey from imbalances and soft tissue disturbances with their causes and conditions to the more erosive destruction of cartilage and bony interaction that is the result of wear and tear, which is called, diagnostically, degenerative joint disease.
Like a gate, a lower limb musculoskeletal joint is made up of interactive parts, has an axis of rotation, an ideal position, a defined range, and a preferred plane of motion. It also needs a space to allow the desired function. As our problematic anatomy undergoes the burden/trauma of impact, weightbearing, and motion, joint integrity is compromised, alignment is lost, and the space needed between parts succumbs to wear and tear. This joint space narrowing and destruction of neutrality causes the bones to wear unevenly, leading to cartilage scarring and the formation of bone spurs, often referred to as osteophytic lipping. As this paradigm continues to play out, the interaction of bone spurs that have been created and occupy the joint space continues to occur. The joint continues to degrade until we are left with “bone on bone” and eventual debilitation. Simply put, loss of form leads to loss of function, but we can take steps to understand, communicate, and correct these issues that, left unchecked, lead to locomotion system failure.
 Timing and positioning are small details that explain big changes. They can be both predictive and diagnostic when seen through the illumination of a computer-aided gait analysis (CAGA).
Timing and positioning are small details that explain big changes. They can be both predictive and diagnostic when seen through the illumination of a computer-aided gait analysis (CAGA).
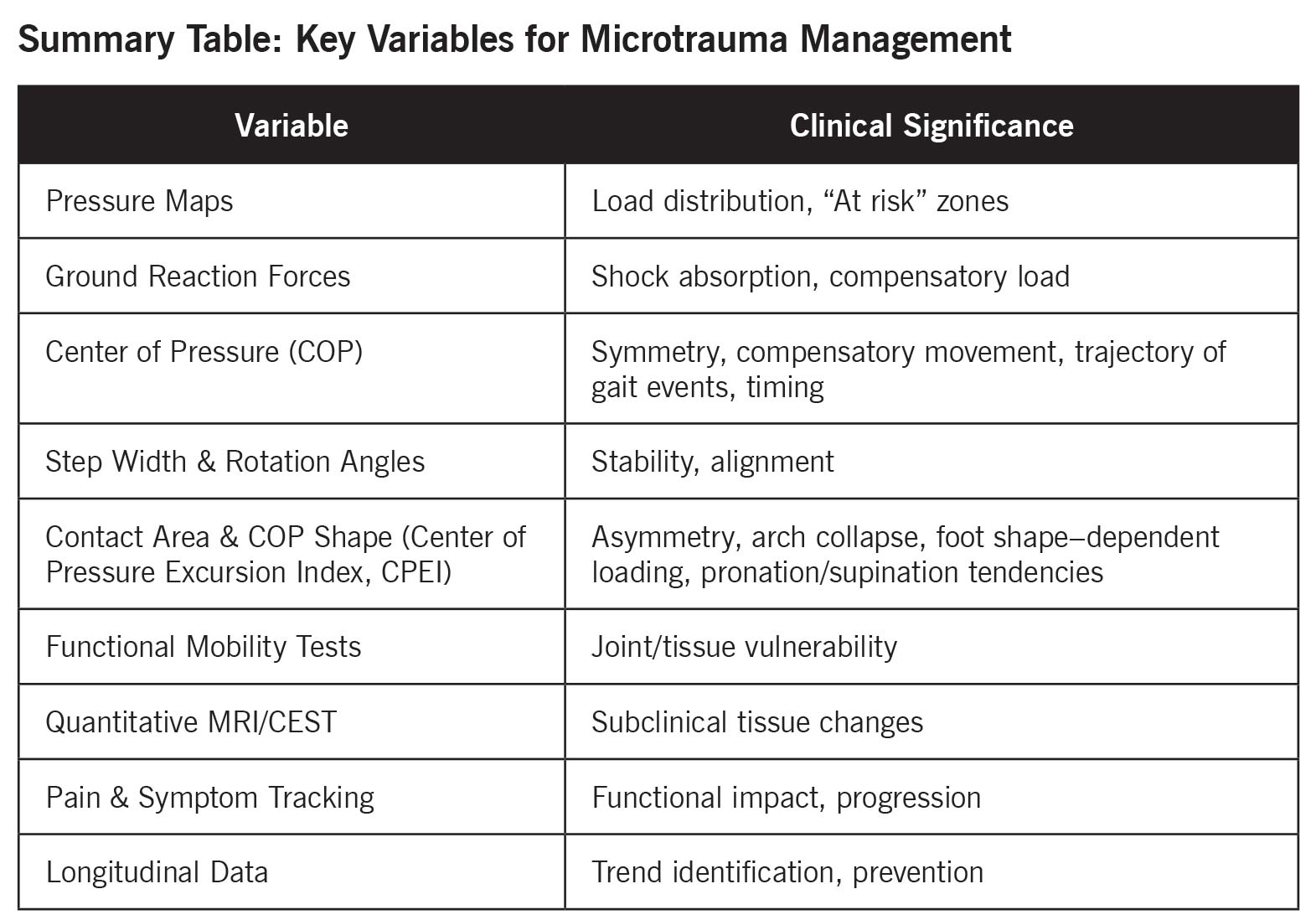
Walking and running are repetitive collisions of 2 dissimilar structures of differing mass, the foot and the support surface. These actions produce propagating shock waves, which, in turn, create repetitive microtrauma that has a net negative effect on the entire musculoskeletal system, as stated in our aforementioned chain of destruction. The prime movers of the kinetic chain, pointedly the foot, ankle, knees, hips, and lower back, pay the highest costs. Given this trauma, it is advantageous to consider the surface interactions, including forces, shock management, positioning, and timing parameters, along with postural kinematic data. Those comprise the center of the wheelhouse for a well-outfitted CAGA system, such as the ones we use in research and patient care.
CAGA allows us to quantitatively spot trouble early and make smart changes.
Microtrauma may not be possible to pinpoint to a single parameter alone. Still, with the cohesive and coordinated comprehensive analysis of measures and changes, both spatial and temporal, we can better explain and validate a subject’s concerns. At the same time, we can design a personalized care plan to include treatment of present issues and prevention. So, yes, degenerative microtrauma is a normal part of moving through life, but with the right CAGA tools and training, we can measure it, understand it, and manage it. A “see this in the data, do this” approach to health care, which can be easily monitored by follow-up CAGA testing.
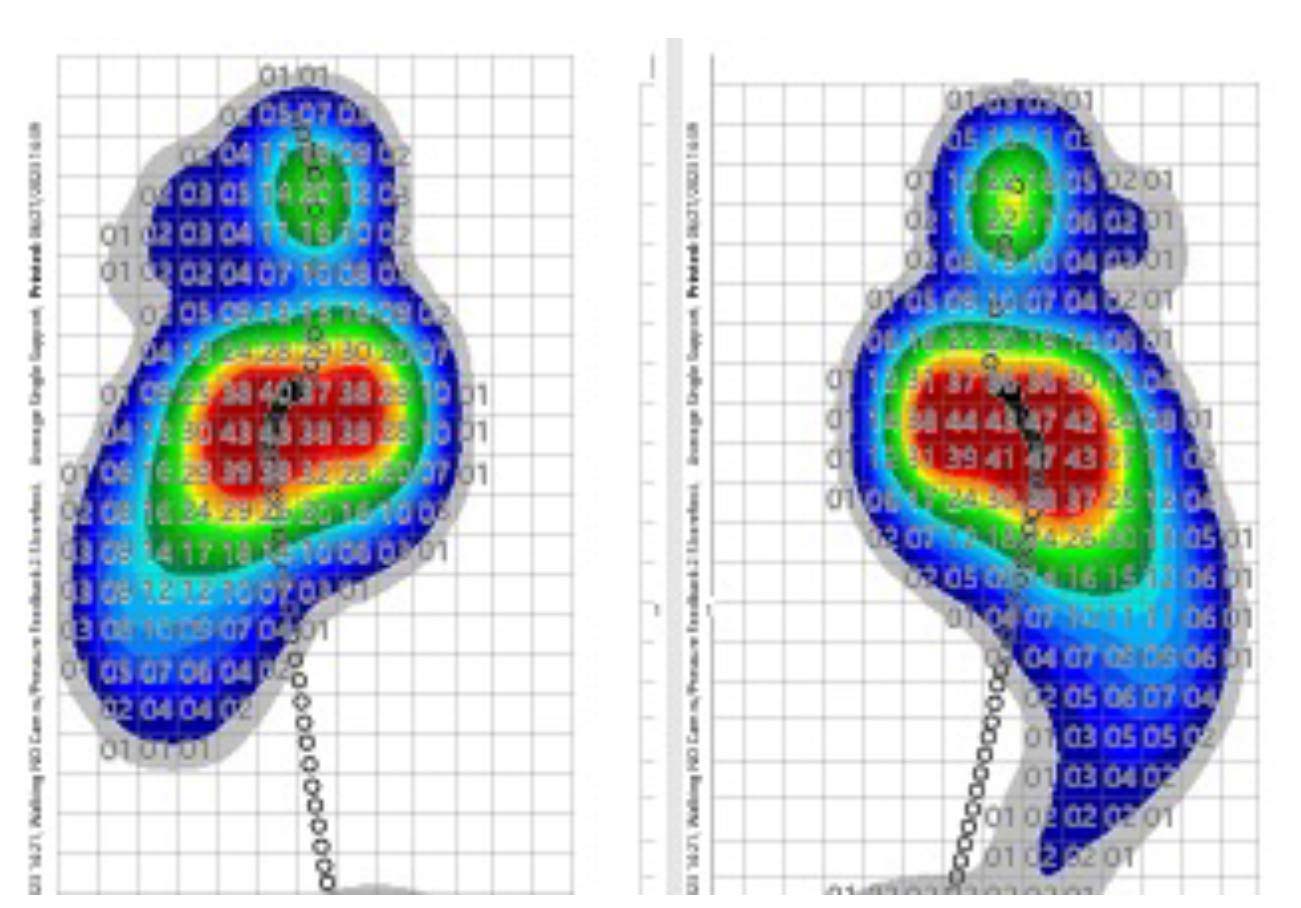
Figure 2: 1 to 1 pressure plots where, when, and also how loading occurs. COP excursion and shape, step width, and rotation angles provide insight into stabilization efforts and potential joint strain.
So, yes, degenerative microtrauma is a normal consequence of moving through life, but, with the right CAGA tools and training, we can measure it, understand it, and manage it. A “see this in the data, do this” approach to health care in general, and orthotic/therapeutic treatment evaluation, in particular, can be easily monitored by follow-up CAGA testing, allowing us to stay on top of these ever-occurring insults to our pedal structures. When considering possible outcomes from our care plans and the conveyance of prognosis, we take this in a step-by-step approach, explaining that there are 3 measurable levels of success: slowing down the progression of musculoskeletal degradation, arresting it, and reversing it, but that the elements of systemic structural deformation and fatigue exist in normalcy. These are demonstrable issues that don’t get better with time but are manageable with keen understanding, clear diagnosis, and a treatment plan aimed at our structural reality, our functional reality, and simple wear and tear over time.





