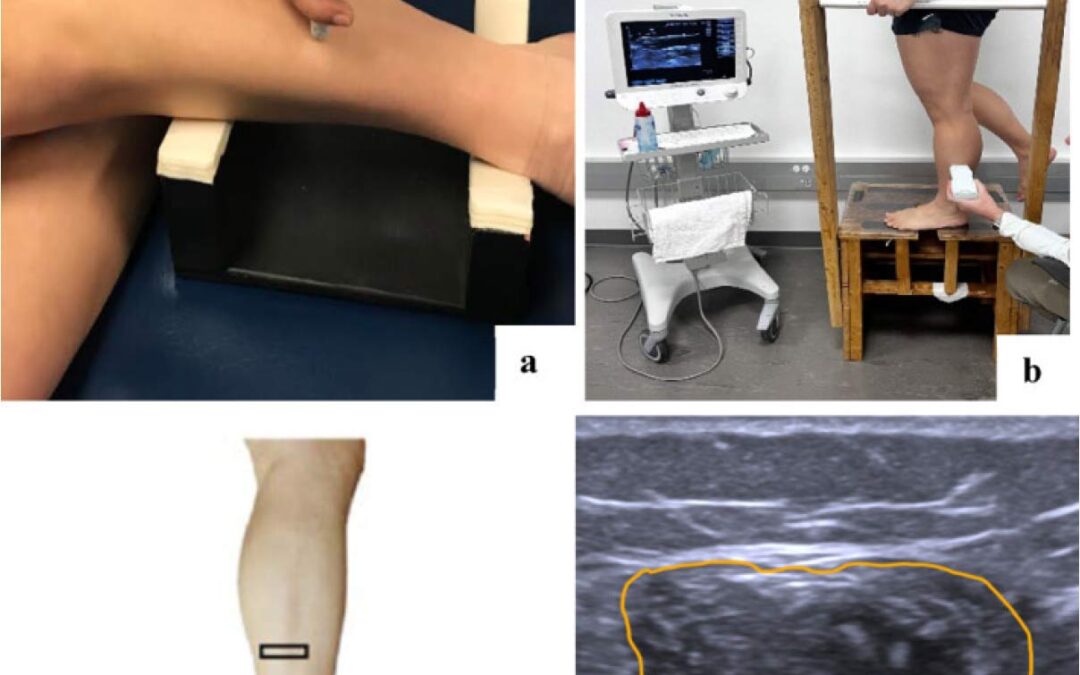

Ultrasound imaging was conducted in side-lying, bilateral standing, and single leg standing positions. (a) Side lying position: This setup shows the peroneal muscles imaged in a non-weight bearing state in side-lying position. (b) Single-leg standing: This image captures the peroneal muscles during weight bearing in single leg standing. Similar position was use for bilateral standing with both feet planted with an equal distribution of weight on both limbs. (c) Probe placement: The ultrasound linear transducer is positioned at 50% of the fibular length, measured from the midpoint between the fibular head and the lateral malleolus. (d) Cross-sectional area measurement: The cross-sectional area (CSA) of the peroneal muscles is measured along the fascial borders indicated by a yellow line.
Lateral ankle sprains (LAS) result in chronic ankle instability (CAI), causing ongoing instability. Although peroneal muscle weakness is documented in CAI, surface electromyography shows similar activation patterns between CAI and healthy individuals, suggesting structural rather than neural deficits. Ultrasound imaging (USI) uniquely enables noninvasive assessment of muscle morphology and quality through cross-sectional area and echogenicity measurements. However, previous USI studies examined peroneals only in non weight-bearing positions, potentially missing functional deficits. This study examines peroneal muscle characteristics in CAI versus healthy individuals specifically during weight-bearing functional positions using USI.
A case-control study was conducted with 58 participants (29 CAI and 29 healthy controls), aged 18-30 years. Cross-sectional area (CSA), echogenicity (grayscale analysis where higher values indicate fatty infiltration/fibrosis), and functional activation ratio (FAR) of the peroneal muscles were assessed using USI in non weight-bearing (side lying) and weight-bearing positions. CSA images were averaged from 3 measurements for each position. The CAI group had significantly smaller CSA in BLS (P < 0.01) and SLS (P < 0.01) but not lying (P = 0.06), higher echogenicity indicating poorer muscle quality (69.7 ± 10.3 vs. 61.3 ± 7.0, P < 0.01), and lower FAR in both BLS (0.99 ± 0.13 vs. 1.13 ± 0.16, P < 0.01) and SLS (1.01 ± 0.17 vs. 1.12 ± 0.22, P = 0.03) compared to healthy controls. Individuals with CAI showed reduced peroneal muscle CSA, lower activation, and poorer muscle quality specifically in weight-bearing positions compared to healthy controls. These findings suggest altered muscle function in CAI especially in functional weight-bearing positions. This demonstrates the need to assess peroneals in functional weight-bearing position compared to resting.
Source: Jaffri A. Functional assessment of peroneal muscles using ultrasound imaging in chronic ankle instability. J Foot Ankle Res. 2025;18(4):e70088. doi: 10.1002/jfa2.70088.





