Empower athletes and work in partnership with them to reduce their risk and severity of overuse injury and keep them at the level of performance they want.
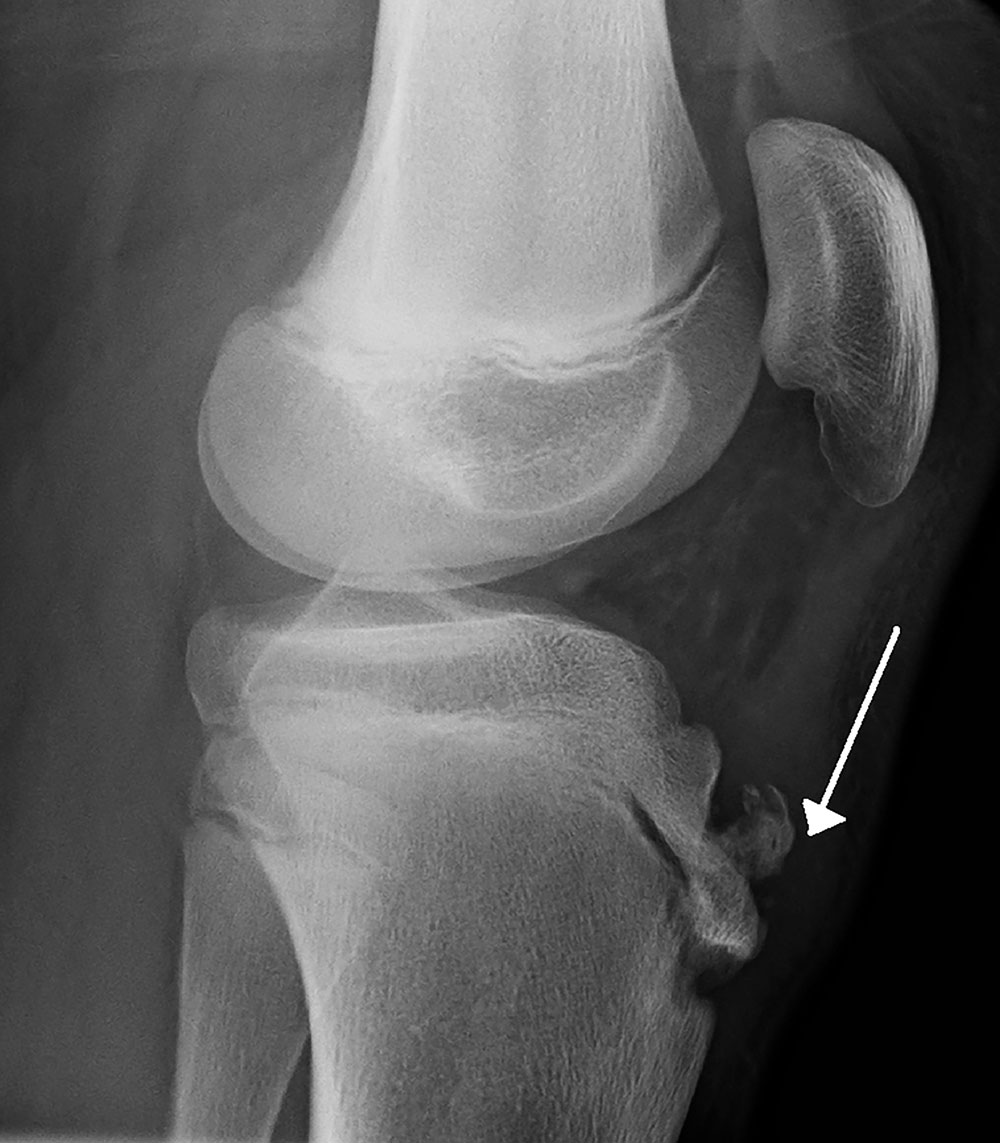
Photo credit: Image of Osgood Schlatter disease by James Heilman, MD. Use is per the Creative Commons Attribution-Share Alike 3.0 Unported license.
By Nicole Wetsman
Getting better at any sport, at any level, takes practice, commitment—and repetition. Basketball players shoot jump shot after jump shot, soccer players drill footwork, and cross-country athletes log seemingly endless miles. The constant work to make each motion natural and instinctive is important but can also wear down the joints involved. For many athletes, repetition can, occasionally, lead to overuse injury. Unlike acute injury, which occurs after a single incident, overuse injury results from repeated small stresses.
“If you are playing a sport at a high level and using your body in that way, you’re subjecting it to potential breakdown due to exposure, to some degree,” said Chris Dodson, MD, sports medicine surgeon and associate professor of orthopedic surgery at Thomas Jefferson University in Philadelphia. “You really can’t stop it. If you could, every major league sport would be doing it. But every single one of them has athletes with overuse injuries.”
Athletes can sometimes continue to play through an overuse injury, but doing so can impair performance, reduce their enjoyment of the sport, and lead to long-term disability. Research on the specific causes of overuse injury and its treatment, however, can help physicians, physical therapists, and athletic trainers work with athletes to decrease their risk of sustaining overuse injuries that restrict play.
“You can’t stop them—but you can reduce them,” Dodson said.
A common problem
Overuse injury is a common problem for athletes at the college and high-school level, across all sports. Thousands of these injuries were recorded in the National Collegiate Athletic Association’s Injury Surveillance System, which tracks injuries in college athletes, and the High School Reporting Information Online, in a span of 4-year and 5-year periods, respectively, according to research published in the American Journal of Sports Medicine in 2015.1 Data produced by that study show that approximately 70% of overuse injuries occurred in the lower extremity. Furthermore, in a 2012 study of nearly 600 college athletes, nearly 30% of reported injuries were overuse injuries.2
Which overuse injuries an athlete is at risk of varies by age, gender, sport, and level of play. The 2015 study1 found that the rate of overuse injury in college athletes was more than 3 times the rate in high-school athletes. In addition, college athletes are far more likely to take more than 3 weeks to recover from such injury and return to play.
The highest rates of injury reported in the study,1 in both college and high school athletes, were in women’s and girl’s cross-country and men’s and boy’s cross-country, followed by women’s and girl’s track and field and men’s and boy’s track and field. In most sports, female athletes are more likely to suffer overuse injury than male athletes are.
Adolescent girls, for example, often develop knee injury as they grow and enter puberty, said John O’Kane, MD, associate professor in the Department of Family Medicine and team physician at the University of Washington. O’Kane and colleagues followed more than 350 female soccer players 12 to 15 years of age over a 4-year period.3 Parents of participants responded to a weekly email, over the course of each soccer season, to report whether their child had any type of overuse injury. Injured players were interviewed by telephone weekly until the injury resolved.
O’Kane identified 83 overuse injuries in the cohort during that period, most commonly to the knee. A common diagnosis was Osgood-Schlatter disease, characterized by inflammation of the patellar tendon causing knee pain.
“[Osgood Schlatter disease] most commonly occurs in the late stages of puberty, because of the inherent weak link in the growth plates at the time. They’re most susceptible just as they’re starting to fuse,” O’Kane said. The condition crops up just as adolescents are at the end of their growth: “Cells in the growth plates become more fragile as they’re starting to close.”
Other problems with the patellar tendon are also common in athletes of all ages who participate in sports that require explosive movement. Approximately 13% of male youth soccer players at an elite academy in Germany had some sort of patellar tendinopathy, according to one study (see Figure).4 Patellar tendinopathy is also common in volleyball players and in basketball players, both of whom jump on a hard surface during play.5 Research on basketball players shows that tendon abnormalities appear on ultrasonography scans even when athletes do not report clinical symptoms: In one study, > 20% of athletes who reported not having a problem in fact had an abnormality on a scan.6
 “[In] anyone who does an explosive sport, like soccer, or football in positions with explosive movement, hamstring injuries are common,” Dodson said. In cross-country runners, however, hamstring injuries rarely occur: “It’s very different in runners,” who, he said, are much more likely to sustain stress fracture. The surface on which a sport is played also contributes to the risk of stress fracture: For example, soccer players running on a soft grass field are less likely to suffer stress fracture than athletes running on a track, Dodson said.
“[In] anyone who does an explosive sport, like soccer, or football in positions with explosive movement, hamstring injuries are common,” Dodson said. In cross-country runners, however, hamstring injuries rarely occur: “It’s very different in runners,” who, he said, are much more likely to sustain stress fracture. The surface on which a sport is played also contributes to the risk of stress fracture: For example, soccer players running on a soft grass field are less likely to suffer stress fracture than athletes running on a track, Dodson said.
However, identifying the rate of overuse injury in any sport, at any level, is challenging: The term is defined inconsistently by researchers and in databases that track them at various institutions.7 “It would be helpful for larger databases to be more standardized,” O’Kane said. The collegiate Pac-12 Conference is working to develop uniform injury reporting to improve that process, he said.
Because overuse injuries don’t occur after a specific event but build over time, there is also inconsistency in when they are reported by athletes to trainers, physicians, and coaches—making it more challenging to identify their specific impact on athletes and athletic performance. For example, a study published in the Journal of Athletic Training in 2018 found that, between 2005 and 2008, the National Collegiate Athletic Association Injury Surveillance System data on men’s and women’s soccer included only approximately two-thirds of overuse injuries that caused time away from the sport.8
Risk reduction and treatment: A checklist
Does the athlete have the necessary strength to perform? Reducing an athlete’s risk of an overuse injury starts with identifying places where they are not strong enough to handle the work that they are asking their body to do, said sports medicine specialist Rob Conenello, DPM.
“Many times, individuals you see are just not strong enough to do the things they want to do. People who want to go running have to be prepared,” Conenello said. “So when I talk about strength, it’s not just weights—it’s good mobility, core strength, flexibility, and those things. If you start with an athlete who has deficiencies, they’re going to get injured. We start seeing overuse problems because they are doing the same thing over and over incorrectly.”
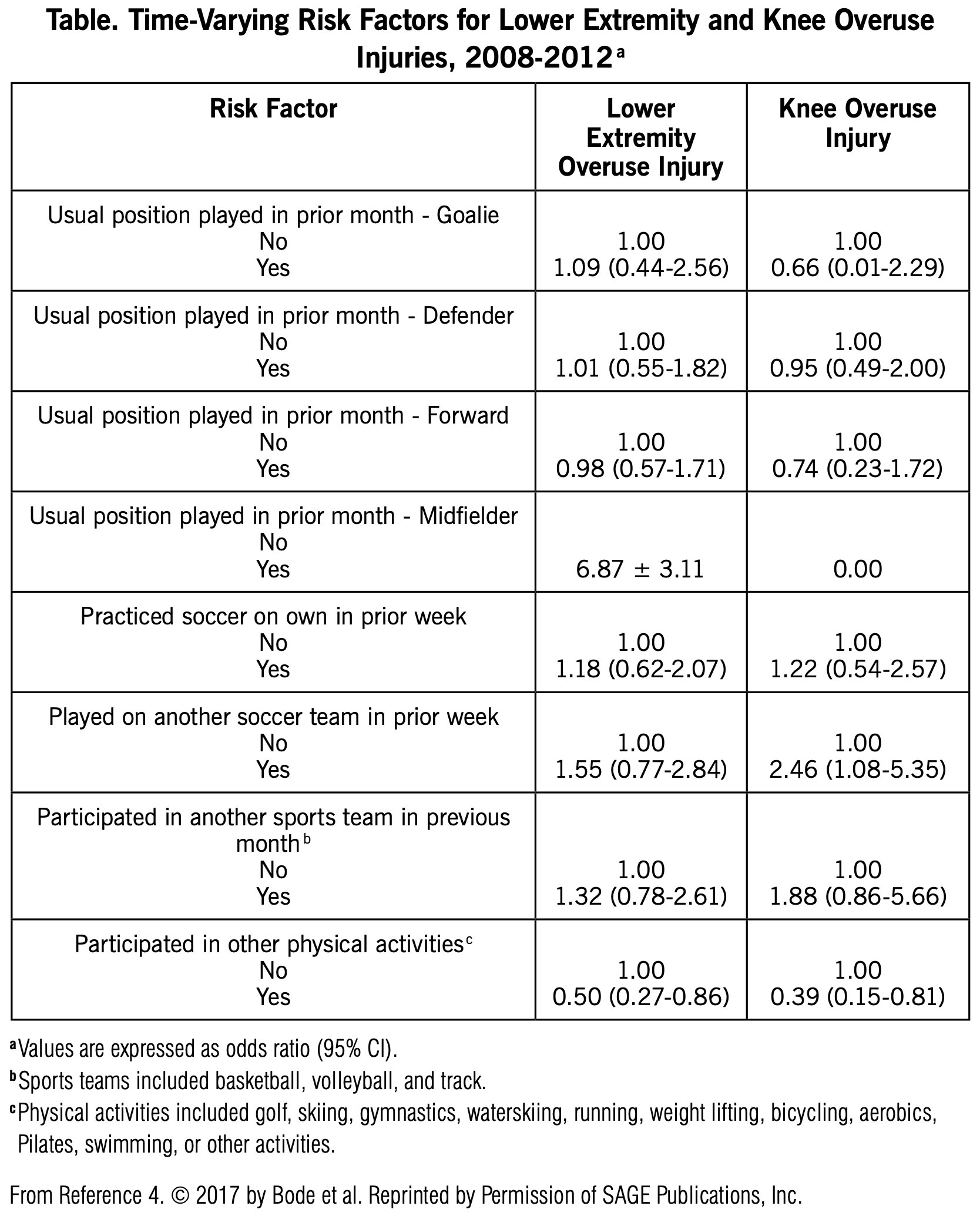
The O’Kane study3 on youth female soccer players also examined variables that put athletes at risk of overuse injury (see Table ). A low normalized knee separation on landing from a jump was associated with a higher risk of knee overuse injury. Greater strength in the hamstring, quadriceps, and hip flexors lowered the risk of knee overuse injury. Identify athletes who have risk factors and take steps to correct them—such as by increasing strength, Conenello said.


Figure. Bode et al found that 64% of youth elite soccer players showed signs of neovascularization of grade I-IV. Image shows sonographical findings of a U-17 player with acute patellar tendon syndrome in the right knee. Structural changes like hypo-echogenic areas, neovascularizations, and tendon thickening were all detectable. Image use is per Creative Commons Attribution License 4.0
Are you screening the athlete regularly for problems? Physical therapists and trainers can screen for those risk factors, Dodson said . “We look at how you move, and see if, for example, you have tight muscles, or more limited rotation in your spine. Those are mechanical and baseline changes that would predispose you to having more overuse injuries. Those are things you can address.”
Is the athlete properly acclimating to practice and play? Rapidly ramping up activity can also increase the risk of overuse injury. “People used to think if you loaded too much, you increased your risk. What’s more clear now is that it’s not so much the total load but the change in load,” O’Kane said. “It’s what you’ve done in the past 2 weeks, and if that’s significantly more than in the prior 2 weeks, the risk goes way up. You want more acclimation.”
Research on stress fractures in college runners demonstrates the way changes increase risk. “The two biggest risk factors for a stress fracture were being a freshman…and having a new coach,” O’Kane said—both situations where an athlete would have a significant change to their running program. Athletes might also be at risk when they return to practice after the offseason: “You might want to return the next season and get after it, but it’s important that the buildup is more gradual.”
Does the athlete know to “listen” to her (his) body? Athletes should not push through if they feel off or sore on a particular day. “The whole idea of no pain, no gain goes out the window,” O’Kane said. “When an athlete tells you that they’re starting to get sore, that’s your best opportunity to try and intervene and prevent an injury. You can lower the load, and get them on a more gradual increase forward.”
If an athlete starts to feel an injury, it’s important to work with a trainer or physician to evaluate whether continued activity will make matters worse: “Things can get worse if athletes continue to ramp things up,” Conenello said. “Something simple can become a stress fracture or a tear,”
A rule of thumb for Conenello is that, if an athlete is limping, they should not be involved in their usual activity. “It’ll cause other problems. Listen to your body, talk to your doctor. If it just hurts when you start exercising and it gets better, that might be fine, but if you’re in the middle of activity and it gets worse, that’s a sign it could be something worse.”
But an athlete isn’t a medical expert, which makes it hard to know when continuing to work through pain will make an injury worse, O’Kane pointed out. “I don’t think an athlete can know if the pain on the inside of their foot is a tweak, and not a big deal, or an impending stress fracture—one is a season ender, and the other just needs an orthotic.”
Have you instructed the athlete to report any injury promptly? Reporting injury early can help an athlete recover and return to regular play and activity more quickly. “I often tell athletes that sometimes the amount of time you’re in pain is the amount of time it will take to get better,” O’Kane said. “If your ankle is sore for a few days, you can make modifications, and be back quickly. If something is nagging you for 4 to 6 weeks before you get it looked at, it may take even longer to get better.”
Final recommendation: Encourage teamwork
Working in partnership with athletes can help reduce the risk and severity of overuse injury and ensure that they can perform at the level they want to. “If you can empower athletes by teaching them what they need to do, you keep them healthy,” Conenello said. “Most athletes are good patients. They’re invested in getting better.”
Nicole Wetsman is a freelance writer in New York City.

- Roos KG, Marshall SW, Kerr ZY, et al. Epidemiology of overuse injuries in collegiate and high school athletics in the United States. Am J Sports Med. 2015;43(7):1790-1797.
- Yang J, Tibbetts S, Covassin T, Cheng G, Nayar S, Heiden E. Epidemiology of overuse and acute injuries among competitive collegiate athletes. J Athl Train. 2012;47(2):198-204.
- O’Kane JW, Neradilek M, Polissar N, Sabado L, Tencer A, Schiff MA. Risk factors for lower extremity overuse injuries in female youth soccer players. Orthop J Sports Med. 2017;5(10):2325967117733963.
- Bode G, Hammer T, Karvouniaris N, et al. Patellar tendinopathy in young elite soccer – clinical and sonographical analysis of a German elite soccer academy. BMC Musculoskelet Disord. 2017;18(1):344.
- Gisslén K, Alfredson H. Neovascularisation and pain in jumper’s knee: a prospective clinical and sonographic study in elite junior volleyball players. Br J Sports Med. 2005;39(7):423-428.
- Cook JL, Khan KM, Kiss ZS, Griffiths L. Patellar tendinopathy in junior basketball players: a controlled clinical and ultrasonographic study of 268 patellar tendons in players aged 14-18 years. Scand J Med Sci Sports. 2000;10(4):216-220.
- Neil ER, Winkelmann ZK, Edler JR. Defining the term “overuse”: an evidence-based review of sports epidemiology literature. J Athl Train. 2018;53(3):279-281.
- Roos K, Kucera KL, Golightly Y, Myers JB, Rosamond W, Marshall SW. Capture of time-loss overuse soccer injuries in the National Collegiate Athletic Association’s injury surveillance system, 2005-2006 through 2007-2008. J Athl Train. 2018;53(3):271-278.






Very interesting and informative