
By Christopher K. Wong, PT, PhD
With a focus on muscle activation, range of motion, and neuromotor training, this 60-year-old went from not being a runner to a half marathon in just a few months.

The author with his daughter after completing the half marathon. The author is a physical therapist, board certified as an orthopedic clinical specialist by the American Board of Physical Therapy Specialties, in practice for over 30 years and dedicated to academic scholarship and professional education currently at Columbia University.
I have never been a runner. The furthest I had ever run was the 7.5-mile Bay to Breakers race across San Francisco, 40 years ago while in college. A few years ago, I started running 1 mile per week to maintain my health for my family, my fitness, and for myself. As a physical therapist and professor, I also serve as a role model for my students and patients—some of whom are competitive runners. I am not competitive, however, and find running 2-3 miles/week has been sufficient to maintain my overall health. But when I was asked to run a half marathon by my daughter (who I had once pushed to run until she collapsed before we knew she had a rare disease called APS1 that made running difficult), I couldn’t say no.
Minimal Training
My main goal was to finish without injury and be able to walk the next day. I knew many running injuries are related to training,1 so I wanted to be smart about training. Cardiopulmonary endurance can reduce injury risk2 and mine would have to improve, though I anticipated having minimal training time since I work 2 jobs. A gradual increase in running distance fit my schedule, which was good since injuries occur most when habitual running distance or intensity increases by 15% or more.3 The result was that before the race, I had only run 13 total miles in a week’s time twice: once split over 3 days, once split over 2 days. Would that be enough? I received skeptical looks from family, runners, and colleagues alike.
Biomechanics
My plan was to optimize my movement potential as I do for my athlete patients so that my body could be as efficient as possible. The first of the 3-step plan was to ensure movements were not limited by fibrosis, often thought of as adhesions or scar tissue, that forms in response to injury but also immobility and affect passive structures such as nerve, joints, and myofascia—the fascia that surrounds all muscle.4 For example, when nerves exiting the spine are restricted, full innervation can be affected and the target muscles weakened; but nerves can be easily mobilized by maintaining spine range-of-motion.5 Joints can be kept healthy by maintaining full range-of-motion and myofascia maintained flexible with simple stretching (Figure 1).6 Joints and fascia can sometimes be addressed together, such as ankle joint dorsiflexion with soleus muscle stretch or knee joint flexion with ankle and midfoot joint plantarflexion and shin muscle stretch. As a physical therapist, I mobilized my joints and muscle fascia by maintaining firm pressure on stiff areas while moving the surrounding joints. Obtaining full joint range-of-motion and muscle flexibility can sometimes be difficult, which is a good reason to consult a skilled manual therapy focused physical therapist.
Optimizing full passive range-of-motion is important because the available motion determines the active motion and power that is produced in running. Power is the work performed in a specified time (P=W/t); and Work is the energy required to move a force through a particular distance (W=Fd) with a related formula for torque through a joint angle. When motion (the distance moved) is limited, the power that can be produced will always be limited when the force applied is the same. Ankle plantarflexion and knee extension enables power generation at push off to propel one forward, while ankle dorsiflexion and knee flexion absorb the shock of impact upon landing. So optimizing my range-of-motion would take advantage of both elements of the Work equation, in case my muscles couldn’t produce substantially more force in the few months I had to prepare knowing that for older people strengthening can take months.7
Active Training

Figure 1: Stretches to minimize passive restraints to movement from restricted nerve, joints, and myofascial. A) arm clock stretch to maintain spinal mobility and prevent myotomal weakness. B) what the author calls a tea ceremony stretch to maintain knee, ankle, and midfoot joint mobility while also stretching quadriceps and anterior shin muscles. C) ankle dorsiflexion with soleus stretch because limitation will also affect knee and hip function. D) lunge stretch for the hip flexors and calf muscles recommended by the author for life as the antidote to the sitting we all do.
The second step was to ensure that all muscles were active and strong throughout the full range-of-motion, which can be checked by simply holding for 10 seconds at all points, especially at the ends of the range-of-motion. I made sure to hold at whatever position I sensed weakness in the form of muscle ache, instability, or trembling. After all, if I couldn’t activate the muscle sufficiently when focused on trying, how could I expect the muscle to work automatically when I wasn’t specifically trying? Then I continued developing strength in the relevant muscles until the weakness went away by spending focused effort, yet minimal time, integrated into my daily life: holding at a certain angle of knee bending when I descended my stairs, reaching the highest point of the heel-raises I did at the kitchen sink when I made coffee, and getting to the lowest point of the split squats and side lunges I did while I brush my teeth.
The third step was integrating my range-of-motion and strength in running through neuromotor training so that all the muscles and joints worked together. Neuromotor training can be considered the coordination that enables efficient use of all the parts—as critical to success as the baton pass in a 4×4 relay. As I tell patients, just because your legs have normal motion and strength doesn’t mean you can dance. Since running steps are so fast, neuromotor training was easiest during walking. Four keys address important points of the gait cycle: 1) extending the trailing or back knee straight behind me ensured gluteus maximus activation, 2) feeling the trailing foot roll over the ball of the feet ensured muscle activation of the calf muscles, 3) engaging the abdominals as the swinging leg advances and generates momentum, and 4) allowing the front knee to bend upon contact to make sure the quadriceps play their role in absorbing impact. Extending the trailing leg allows longer step lengths without the jarring horizontal braking force that occurs with over striding. While some suggest shortening step length, gait speed is the simple product of step length and cadence, so reducing either will slow a runner down. And though my primary goal was to finish, I didn’t want to run slower. Training new neuromotor patterns into any activity takes time, but long runs provide the time.
Accounting for Real Life
I ran using these tips to optimize my running body mechanics but had to build up my endurance or cardiopulmonary capacity over the couple months before the race. Afterall, many can run to the corner, but few can run a marathon. I emphasized rest and recovery, which meant not running every day and attending to various aches and pains as they occurred with the self-stretches and joint mobilizations described above. With a goal of at least a couple long runs of 10 miles before the race, I stuck with a regimen of a couple short runs and a longer run each week. Since my goal was to finish without injury, I didn’t fret if I had to walk briskly during a long run—the same advice I have often given to patients as they recover and return to running. As the race approached, I tried not to walk but walked as fast as possible for as short a time as possible when I did.
Then to account for the course topography, I made sure my running environment included hills to account for the elevation changes on the race map. Inclines are an efficient way to force abdominal muscles and the gluteus maximus to work as well as necessary for cardiovascular conditioning; declines challenge the quadriceps.8 Counting for the adrenaline fueled psychological environment of a run with a crowd of people, I didn’t bother to run more than 10 miles in training ever, figuring that the crowd of eager motivated peers would pull me over the finish line. The process spelled out here of working through Passive restraints to movement, Activating muscles in their specific positions, Neuromotor training to integrate into the Activities of life, building sufficient cardiovascular Capacity to perform in real life Environments, all while harnessing an Attitude for success, I describe with the acronym PANACEA for rehabilitation9 (Figure 2).
Attitude
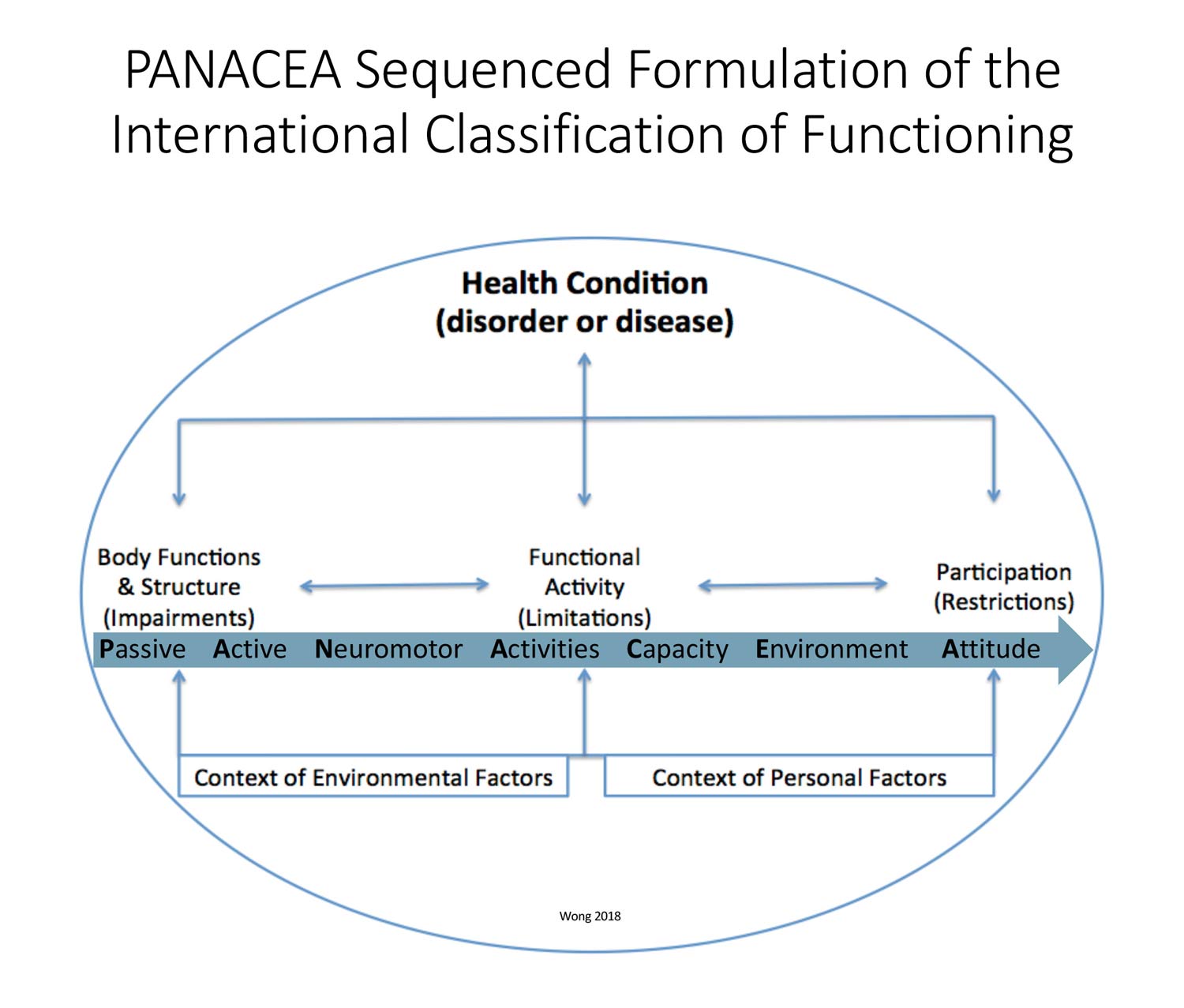
Figure 2: The International Classification of Functioning (ICF) model describes an individual’s health condition considering personal and environmental factors that affect them in the context of their body’s impairments, that lead to functional limitations, and can ultimately restrict full participation in life. The PANACEA sequence optimizes a person’s participation by addressing all ICF elements in logical order from impairments to functional activities to requirements for life participation. Minimizing passive restraints to movement, activating musculature, and neuromotor coordination enables active participation in building the cardiopulmonary capacity needed for real life social and physical environments. Attitude is a personal factor that must be always addressed. This figure is the author’s adaptation from his prior work, Graham E, Johnson M, Wong CK. Return to running after rehabilitation for chronic 16-year cremaster strain: a case study. J Orthop Sports Phys The Cases. 2024;4(3):146-152. https://doi.org/10.2519/josptcases.2024.0007.
Biomechanical and physiological factors don’t completely explain the success of people engaging in endurance sports.10 Psychological traits, including motivation and attitude, are also critical aspects. Some need external motivation such as an impending goal, in my case just finishing the race. Some are intrinsically motivated by maintaining psychological and physical health.11 I am always inspired by my many patients who have struggled through rehabilitation to return to running and also my friends who have overcome leg amputations to walk, run, and excel at world class paralympic levels.
For me, my biggest motivator was to run the half marathon with my daughter who I had once had to carry home after we tried to run too far before knowing that her health was compromised by APS1. Autoimmune polyglandular syndrome type 1 (APS1) affects multiple organs due to mutations of the autoimmune regulator AIRE gene.12 While the various organs affected can be medically managed, there is no cure. So in the grand scheme of things, the ability to run the half marathon was just one health issue for my daughter to conquer, and a way for me to relieve my lingering unnecessary parental guilt.
Conclusion
Ultimately, we did complete the half marathon. I ran without causing injury, walked down my stairs the next morning, and went to work without pain. My daughter beat me to the finish line by 10 minutes and was happy and inspired to run more. Honestly, my best-case scenario. My only problem is that now she wants us to run another!
Christopher K. Wong, PT, PhD, is a Certified Orthopedic Clinical Specialist and Professor of Rehabilitation & Regenerative Medicine at Columbia University Irving Medical Center and Curriculum Director of the Clinical Residency in Orthopedic Physical Therapy at Columbia University Vagelos College of Physicians and Surgeons in New York City. He is also Co-Chief Editor, Journal of Clinical Education in Physical Therapy, which can be found at https://journals.library.columbia.edu/index.php/jcept
- Burke A, Dillon S, O’Connor S et al. Aetiological factors of running-related injuries: a 12 month prospective “Running Injury Surveillance Centre” (RISC) study. Sports Med Open. 2023;9(1):46. https://doi.org/10.1186/s40798-023-00589-1
- Lisman PJ, de la Motte SJ, Gribbin TC, et al. A systematic review of the association between physical fitness and musculoskeletal injury risk: Part 1-Cardiorespiratory endurance. J Strength Cond Res. 2017;31(6):1744-57.
- Gabbett TJ. The training–injury prevention paradox: should athletes be training smarter and harder? Br J Sports Med. 2016;50(5):273-80.
- Ando A, Suda H, Hagiwara Y, et al. Remobilization does not restore immobilization – induced adhesion of capsule and restricted joint motion in rat knee joints. Tohoku J Exp Med. 2012;227(1):13-22.
- Basson A, Olivier B, Ellis R, et al. The effectiveness of neural mobilization for neuromusculoskeletal conditions: a systematic review and meta-analysis. J Orthop Sports Phys Ther. 2017;47(9):593-615.
- Konrad A, Alizadeh S, Daneshjoo A, et al. Chronic effects of stretching on range of motion with consideration of potential moderating variables: a systematic review with meta-analysis. J Sport Health Sci. 2024;13(2):186-94.
- Csapo R, Alegre LM. Effects of resistance training with moderate vs heavy loads on muscle mass and strength in the elderly: a meta-analysis. Scand J Med Sci Sports. 2016;26(9):995-1006.
- Pickle NT, Grabowski AM, Auyang AG, Silverman AK. The functional roles of muscles during sloped walking. J Biomech. 2016;49(14):3244-51.
- Wong CK, Sheppard JK, Williams KL. Improving balance and walking ability in community-dwelling people with lower limb loss: a narrative review with clinical suggestions. Phys Ther Rvw. 2018;23(2):124-32.
- Konopka MJ, Zeegers MP, Solberg PA, et al. Factors associated with high-level endurance performance: An expert consensus derived via the Delphi technique. PLoS One. 2022;17(12):e0279492.
- Tjelta LI, Kavale PE, Shalfawi S. The half-marathon participants, who are they and what motivates them for training and competition? Acta Kinesiologiae. 2017;23: https://doi.org/10.12697/akut.2017.23.04
- National Organization for Rare Disorders (NORD). Autoimmune Polyglandular Syndrome Type 1. Available at https://rarediseases.org/rare-diseases/autoimmune-polyglandular-syndrome-type-1/. Accessed May 1, 2025.






At Strokess, we deeply resonate with the idea that biomechanics and belief can work together to unlock new possibilities—this story is proof that age and past limitations are no match for smart training and strong motivation.