
 A summarized talk by Joseph Park, DPM, FACFAS
A summarized talk by Joseph Park, DPM, FACFAS
Flatfoot, particularly flexible adult Stage 2 flatfoot, presents a complex challenge. This summary reviews proper patient evaluation for the condition and discusses the critical non-surgical and surgical considerations for managing stage 2 flatfoot, offering a deep dive into both soft tissue and osseous procedural options. By understanding the pathology’s nature, evaluating the demographic factors, and considering various surgical options, healthcare providers can tailor treatments that effectively address the specific needs of each patient.
Flexible adult stage 2 flatfoot, characterized by a deformity that remains correctable, highlights a progression from Stage 1 where no deformity exists, just isolated posterior tibial tendon issues. In stage 2 flatfoot, the deformity is evident but still flexible, allowing some alignment upon manipulation. This stage is crucial for intervention as the condition has not yet led to the rigid deformities found in later stages.
Following the Johnson and Strom system, stage 2A involves a visible but correctable deformity without significant abduction or additional plane deformities. Transitioning to stage 2B introduces a complexity where the deformity includes abduction, evident in the transverse plane component. These stages necessitate a tailored approach, focusing on preserving flexibility while addressing the deformity structurally and symptomatically.
Key Patient Considerations
Age: Age significantly impacts the approach to treating stage 2 flatfoot. Younger adults may have inherent flexibility aiding recovery, potentially requiring less invasive procedures. Conversely, older adults often present with additional complications such as diminished healing capacity and increased rigidity, leaning toward more aggressive interventions to ensure functionality and reduce discomfort.
Impact of BMI: The body mass index (BMI) of a patient plays a critical role in determining surgical options for stage 2 flatfoot. Higher BMI can increase the stress on the foot structure, often necessitating more robust surgical procedures to ensure adequate correction and reduce the risk of recurrence. This consideration impacts the choice of techniques, potentially leaning toward procedures that provide greater structural support to accommodate increased body weight.
 Comprehensive Preoperative Evaluation
Comprehensive Preoperative Evaluation
History Review: Before proceeding with surgical intervention for a flexible adult stage 2 flatfoot, it’s crucial to review the patient’s medical and social history thoroughly. This includes assessing the patient’s age, BMI, and underlying medical conditions such as diabetes or rheumatological diseases. Smoking status and previous foot conditions must also be evaluated since they can affect surgical outcomes and recovery. Understanding the patient’s level of physical activity and their social factors, such as the ability to take time off work (typically 4-6 months) for recovery, is essential. These factors help in planning the surgical approach and setting realistic postoperative expectations.
Physical Examination: The physical examination should include both non-weight bearing and weight-bearing assessments. Checking the ankle range of motion, subtalar joint motion, and the alignment of the foot are crucial. The physical examination should focus on identifying any pain during motion, the stability of the medial column, and palpation of the posterior tibial tendon to assess for tenderness or thickening. Evaluating the heel position, medial longitudinal arch height, and forefoot positioning during single and double heel raises provides additional information on the functionality of the foot and the extent of the deformity.
Radiographic and Diagnostic Assessment
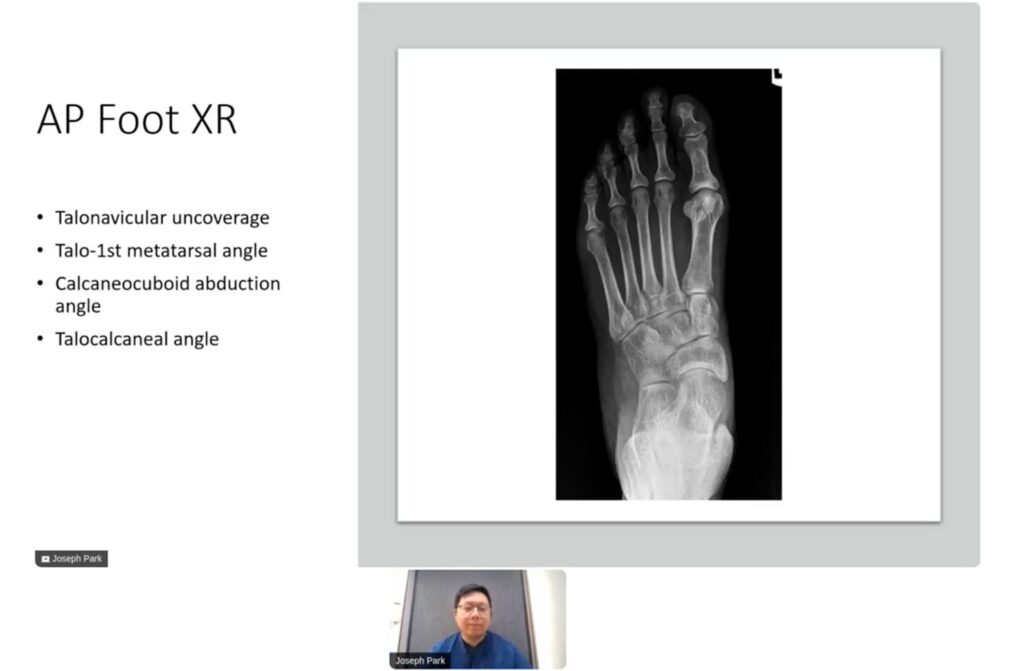
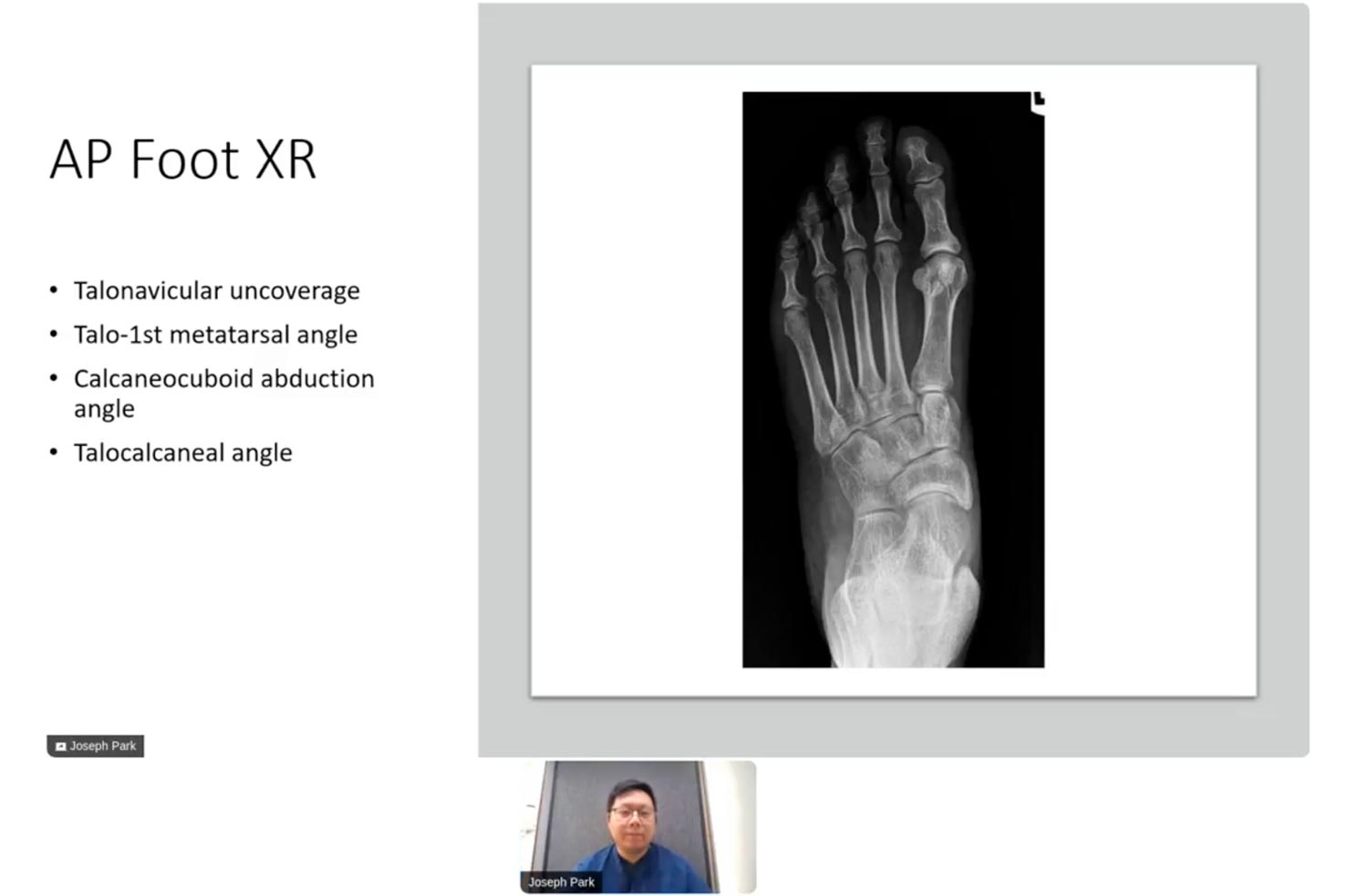
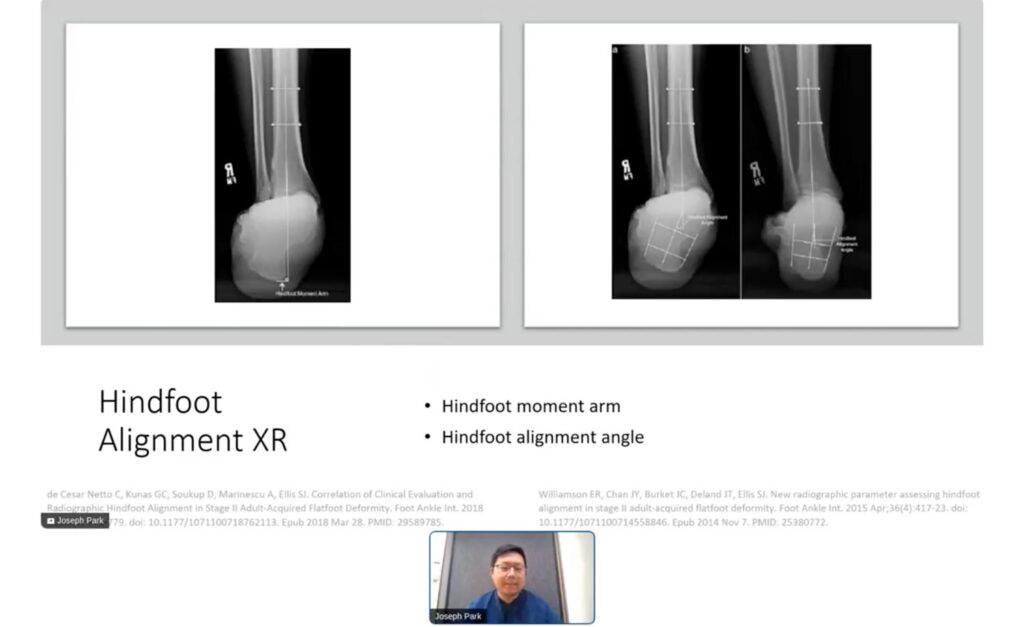
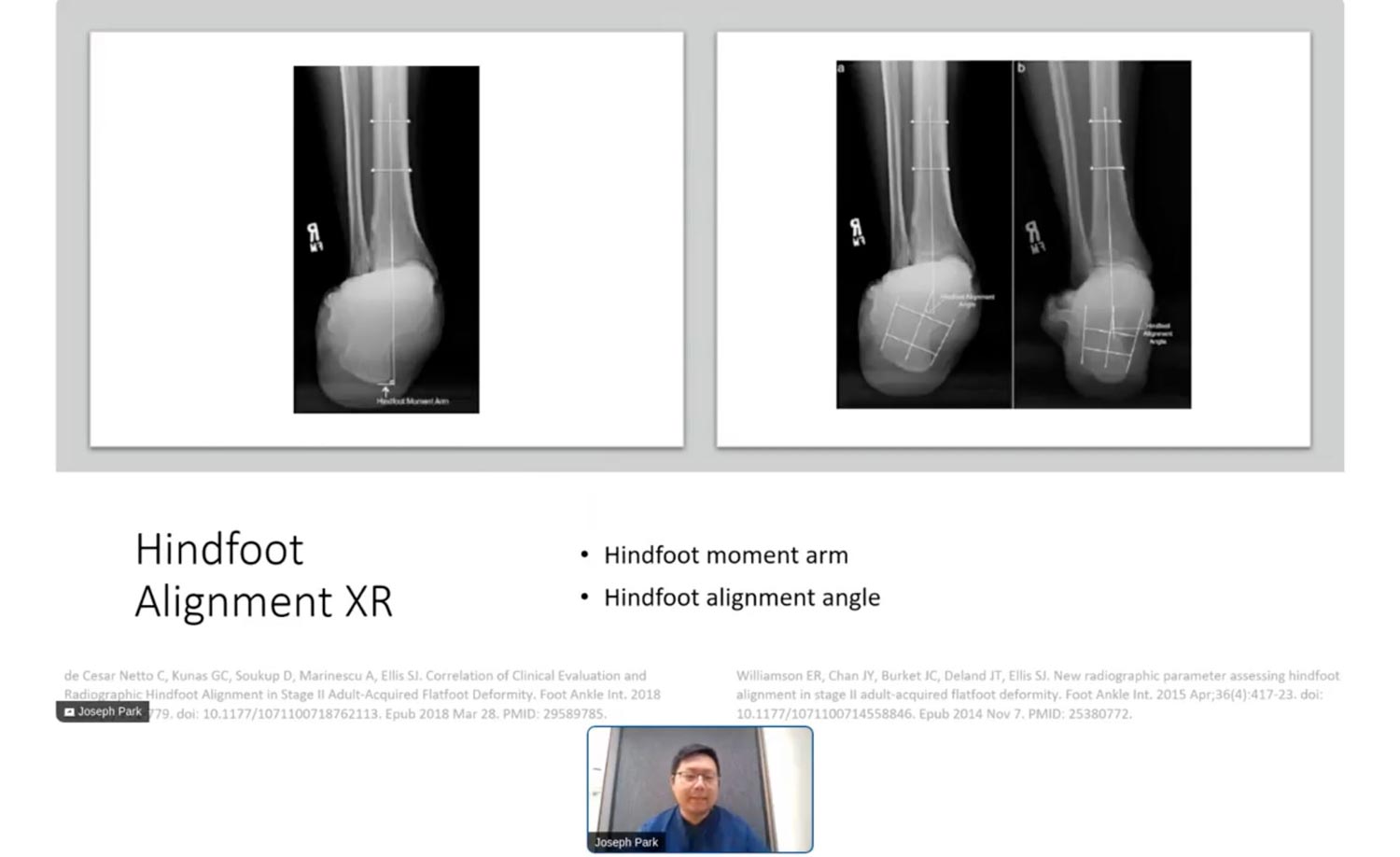
Radiographic evaluation is key in planning the surgical correction of stage 2 flatfoot. Weight-bearing radiographs of the foot and ankle, including anteroposterior (AP), lateral, and oblique views, are standard. These images allow the surgeon to assess the alignment and structural changes in the foot. In some cases, advanced imaging techniques such as weight-bearing computed tomography (CT) scans may be useful. These scans provide a more detailed view of joint alignment, particularly in complex cases, and help in identifying conditions like sinus tarsi impingement or subtalar joint subluxation, which are harder to detect with traditional radiographs.
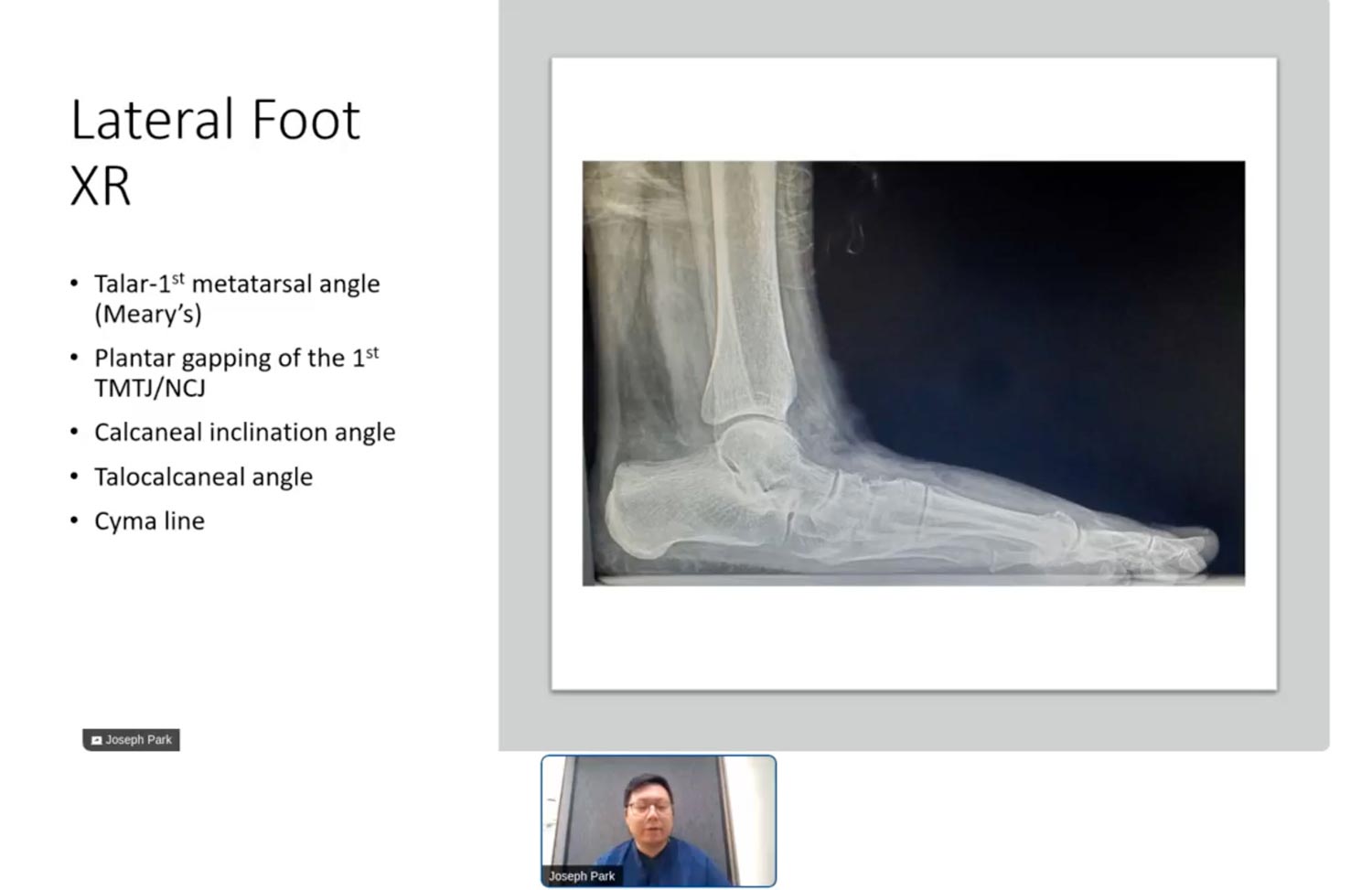 Analyzing radiographic indices such as the talonavicular coverage angle, calcaneocuboid abduction angle, and the talo-first metatarsal angle on AP and lateral foot views is crucial. These indices help determine the severity of the deformity and guide the surgical planning. For instance, a talonavicular coverage angle greater than 40% typically indicates pathology. The calcaneal inclination angle and talocalcaneal angle are also evaluated to assess the heel alignment and the flatfoot severity. Accurately interpreting these indices ensures appropriate surgical intervention, maximizing the chances of restoring normal foot function and reducing postoperative complications.
Analyzing radiographic indices such as the talonavicular coverage angle, calcaneocuboid abduction angle, and the talo-first metatarsal angle on AP and lateral foot views is crucial. These indices help determine the severity of the deformity and guide the surgical planning. For instance, a talonavicular coverage angle greater than 40% typically indicates pathology. The calcaneal inclination angle and talocalcaneal angle are also evaluated to assess the heel alignment and the flatfoot severity. Accurately interpreting these indices ensures appropriate surgical intervention, maximizing the chances of restoring normal foot function and reducing postoperative complications.
Decision Making: Non-Operative vs. Operative Treatment
Non-surgical management of flexible adult stage 2 flatfoot, such as orthosis use and physical therapy, has shown mixed outcomes in the long term. Studies suggest that while non-operative measures can be effective for some, a significant percentage of patients eventually require surgical intervention. O’Connor et al1 found that despite conservative treatment measures, roughly 24.6% of patients progressed to surgery within 5 years. Lin et al2 reported that 70% of the patients were brace-free at follow-up, highlighting successful non-surgical management. However, 30% did not fully succeed with non-operative treatments, demonstrating need for a more definitive solution like surgery.
Surgical intervention is considered when non-operative treatments fail or when the patient’s activity level and quality of life are significantly impacted. Research by Coster et al3 showed substantial benefits, including pain reduction and functional improvements post-surgery for adult stage 2 flatfoot. Surgical treatments focus on realigning the foot structure, reducing pain, and restoring function, aiming for long-term patient satisfaction and mobility. Surgeons decisions weigh factors like patient age, activity desires, and the severity of the foot deformity.
Surgical Treatment Options for Stage 2 Flatfoot
Soft Tissue Procedures: Soft tissue procedures in the surgical treatment of stage 2 flatfoot often include gastrocnemius recession or tendon transfers to correct muscular imbalances and improve foot alignment. These surgeries aid in reducing the stress on tendons and correcting minor deformities without the need for bone alteration. Techniques such as a posterior lengthening, are recommended only when the patient’s activity levels are considered, as they might affect muscle functionality. Ligament reconstructions, including spring ligament and deltoid ligament repairs, may also be pursued to restore stability and prevent further deformation.
Osseous Procedures: Osseous procedures involve modifications to the bone structure to correct the foot alignment more definitively. Medial displacement calcaneal osteotomy (MDCO) is a popular method used to shift the heel bone inward and restore the foot’s arch. This procedure often is complemented with lateral column lengthening when there is significant forefoot abduction, which helps in realigning the foot more comprehensively. These procedures are crucial for achieving a stable, functional foot that can support the patient’s weight and activity without pain. Additional procedures like arthrodesis (joint fusion) may be considered in more severe or rigid cases, providing a permanent correction by fusing the affected joints into the correct position.
 Postoperative Care and Rehabilitation
Postoperative Care and Rehabilitation
Immediate: Postoperative care following stage 2 flatfoot surgery is crucial for ensuring a successful recovery. Initially, this involves managing post-surgical pain, reducing swelling, and preventing infection. Patients are typically advised to avoid weight-bearing activities, and the use of crutches or a walker may be necessary. It is important to keep the surgical site clean and dry, and dressing changes should be performed as directed by the surgeon to avoid complications.
Long-term & Follow-up: Long-term management of stage 2 flatfoot surgery includes physical therapy focused on restoring strength and mobility. Follow-up appointments are essential for monitoring the healing process and for making necessary adjustments in the treatment plan. Patients may undergo periodic X-rays to ensure proper alignment and healing of bones. Rehabilitation exercises gradually increase in intensity based on individual recovery progress. Additionally, patients might need orthotic devices to support proper foot alignment and distribution of pressure during activities. Regular consultations help to address any ongoing issues or concerns, ensuring the best possible outcome.
Conclusion
In summary, addressing flexible adult stage 2 flatfoot surgically requires a comprehensive understandig of the patient’s unique foot anatomy, lifestyle, and expectations. The decision to pursue surgery must balance the risks and benefits while considering non-operative alternatives that might be effective. When surgery is indicated, it’s essential to choose the appropriate procedures aimed at correcting the specific deformity and restoring function, considering both osseous and soft tissue interventions.
The ultimate goal of surgical intervention is to reduce pain, improve foot alignment, and enhance the patient’s quality of life. With careful surgical planning and execution, combined with appropriate post-operative care, patients can achieve significant improvements in foot function and overall satisfaction with their surgical outcomes. As research evolves, so do the techniques and recommendations for treating stage 2 flatfoot, affording patients better and more tailored treatment options.

Joseph Park, DPM, FACFAS, is Assistant Professor at the Western University College of Podiatric Medicine and Attending Physician at Riverside University Health System, both in Southern California.
This article is a summary of Dr. Park’s presentation from the 2024 No-Nonsense Seminar, March 8, 2024, moderated by LER Publisher & CEO Rich Dubin. To view this lerEXPO event, visit https://nononsense2025.lerexpo.com. Continuing education credits are available for many of our programs.
- O’Connor K, Baumhauer J, Houck JR. Patient factors in the selection of operative versus nonoperative treatment for posterior tibial tendon dysfunction. Foot Ankle Int. 2010;31(3):197-202. Doi: 10.3113/FAI.2010.0197.
- Lin JL, Balbas J, Richardson EG. Results of non-surgical treatment of stage II posterior tibial tendon dysfunction: a 7- to 10-year followup. Foot Ankle Int. 2008;29(8):781-6. Doi: 10.3113/FAI.2008.0781.
- Coster MC, Rosengren BE, Bremander Ak, Karlsson MK. Surgery for adult acquired flatfoot due to posterior tibial tendon dysfunction reduces pain, improves function and health related quality of life. Foot Ankle Surg. 2015;21(4):286-9. Doi 10.1016/j.fas.2015.04.003.





