
 Stemming the Rising Tide of Senior Falls
Stemming the Rising Tide of Senior Falls
By Jason Kraus, BS
As we celebrate Older Americans Month, it’s essential that we ask ourselves what we can do to help stem the deeply troubling and seemingly intractable issue of senior falls. As it turns out, there’s a great deal we can do.
The human toll of falls among seniors is substantial, resulting in numerous injuries, disabilities, hospitalizations, and deaths each year, significantly impacting quality of life and independence. According to the Centers for Disease Control and Prevention (CDC), about 36 million older Americans experience a fall each year.1 One in 4 older adults falls each year in the United States. One out of 5 of these falls causes a serious injury such as broken bones or a head injury. As a result, falls are the leading cause of injury and injury death among adults age 65 and older. Many older adults who fall become less active and independent, requiring more long-term care and support services. This places strain on family members and other caregivers and increases the likelihood of nursing home admission. Additionally, fear of falling can cause some seniors to limit their activities, leading to social isolation, depression, and further physical decline.2
The financial toll of senior falls is no less staggering. Falls cost the U.S. healthcare system $50 billion annually,3 with three-quarters of those costs borne by Medicare and Medicaid. Beyond the direct medical expenses, falls can lead to a cascade of other hidden costs including patient monitoring, lost wages, and lost productivity in the work force.
Virtually every medical practice whose patient population regularly includes seniors see patients at risk for falls on a near daily basis. Typically, however, fall risk is not part of the conversation as these patients are appointed for myriad other issues and fall risk is simply not top of mind. Even patients who struggle as they move from reception room to treatment room or who require assistive devices are likely to leave their appointment without any mention of fall risk management.
Ironically, the recent implementation of Merit-based Incentive Payment System (MIPS) measure 318 – in which patients are assessed for fall risk and asked about falls – has done little to move the needle. First, there is no required, or even preferred, method of assessment. Only a list of options is provided. Nor is there any guidance for clinical recommendation beyond that a referral may be necessary. Refer to whom? Based on what criteria?
The science is clear regarding the single greatest fall risk factor that seniors face: a history of previous falls.4 Despite this commonly accepted reality, there continue to be missed opportunities between patients who have suffered a fall – and are at a high risk to fall again – and those who treat the consequences of those falls. Consider the more than 300,000 seniors who fall and break a hip each year in the U.S:1 They’re rushed to an emergency room, x-rayed, the fracture repaired or the hip replaced, followed by weeks or months of physical therapy. Patients are then discharged and the falls cycle often continues. What would seem to be more appropriate is a referral rather than a discharge, and lower extremity specialists should establish themselves as the destination for these patients.
What we know is that to move the needle, a holistic, multidisciplinary approach is necessary.5 Every specialty has a role to play whether as an active participant in a patient’s fall risk care, or as an informed and proactive referral source. In a sense, the rest of team is presently on the field, but the quarterback is missing.
Arguably, the logical specialty to suit up as quarterback is podiatry. In its exhaustive, systematic review of literature on lower-limb factors associated with balance and falls, Neville et al (writing for the National Council on Fall Risk Awareness and Prevention) found 6 highly correlated direct links to lower-limb-related influences on fall-risk in older adults.6 These included:
- range of motion
- orthoses
- strength
- footwear
- pain
- deformity
They found 2 additional links that they determined to be indirect. These included plantar skin/soft-tissue and sensory-loss. In another ground-breaking study, Wylie et al also established a definitive link between podiatric care and falls management.7 Logically, and according to the science, Podiatry is best positioned to lead a revolution in senior falls awareness and prevention.
So where to begin? By changing the way you think. Instead of narrowly defining a patient by their chief complaints, broaden the view to include the whole person and their long-term wellbeing. Be open to identifying the unseen or unsaid. (At least half of seniors who have fallen never reveal it to their friends, family or physician.) Be willing to discover more substantial ways in which you can be of service to your patients. If you redefine your role from fixing foot pain to ensuring that patients move comfortably throughout their lives, you can unlock multiple opportunities for preventing life changing injuries.
The fundamental approach to a falls management protocol follows this basic workflow:
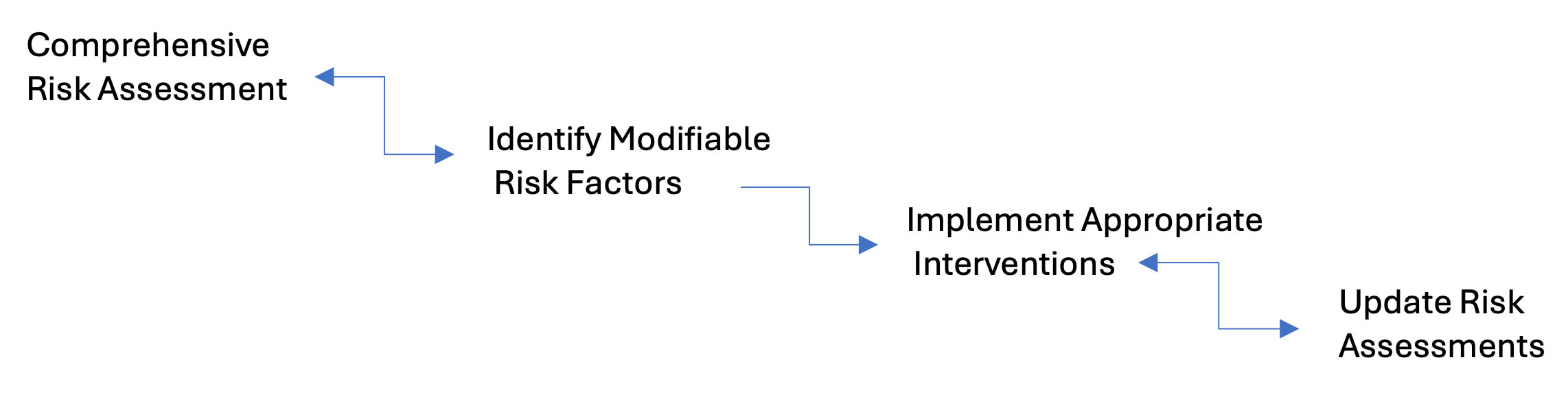
There are exciting new tools available to practitioners to easily implement this protocol. Following both CDC and CMS guidelines, Orthotica recently launched its Life in Balance fall risk management program. Anchored by an evidence-based and reimbursable assessment, this straightforward tool helps providers evaluate all primary fall risk factors, establishes a baseline fall risk score, and generates a risk reduction framework exclusive to each patient. Additionally, specially designed AFOs have been shown to be a highly effective intervention for elderly patients who present with muscle weakness or unsteady gait.8
The leadership vacuum around senior falls prevention is so colossal that the opportunity for practitioners interested in filling that void is equally vast. Simply raise your hand, and your practice can easily become the destination for preventing and lowering the risk of falls in your community. Much as our cholesterol is regularly checked, all senior patients should be assessed for falls at least annually, and more often for those at high risk. Alert primary care physicians and other potential referrers in your area of your new focus. Reach out to local journalists who write about health and let them know that falls in our senior population are not inevitable and that you have the expertise and commitment to help stem the tide of senior falls in your community. Even if you do nothing more than train your staff to be aware of fall risk and establish a falls protocol for your existing patient population, you will be making a meaningful contribution to the health and wellbeing of hundreds, if not thousands, of older Americans.
Jason Kraus, BS, has held executive management positions in the healthcare industry for more than 40 years. Prior to co-founding Orthotica Labs in 2022, Jason served as Chief Revenue and Strategy Officer and Director of OHI, was a Partner in the practice consulting firm S.O.S. Healthcare Management Solutions, LLC, and Co-founder of Benefoot Orthotic Laboratory. In addition to serving on numerous professional boards, Jason is a frequent lecturer at medical conferences world-wide on a wide range of marketing and management topics, and has authored numerous practice management articles that have appeared in professional journals and trade publications.

- Kakara R, Bergen G, Burns E, Stevens M. Nonfatal and Fatal Falls Among Adults Aged ≥65 Years — United States, 2020–2021. MMWR Morb Mortal Wkly Rep 2023;72:938–943. DOI: http://dx.doi.org/10.15585/mmwr.mm7235a1
- Get the Facts on Falls Prevention. Published March 13, 2023. Available at https://www.ncoa.org/article/get-the-facts-on-falls-prevention. Accessed May 10, 2024.
- Florence CS, Bergen G, Atherly A, Burns E, Stevens J, Drake C. Medical Costs of Fatal and Nonfatal Falls in Older Adults. J Am Geriatr Soc. 2018;66(4):693-698. doi: 10.1111/jgs.15304.
- Wapp C, Mittaz Hager AG, Hilfiker R, Zysset P. History of falls and fear of falling are predictive of future falls: Outcome of a fall rate model applied to the Swiss CHEF Trial cohort. Front Aging. 2022;3:1056779. doi: 10.3389/fragi.2022.1056779. Erratum in: Front Aging. 2023 Jul 06;4:1235431.
- Leggett C, Jess J, McNamara R. A multi-disciplinary approach to falls prevention in the elderly. Intern J Integ Care. 2017;17(5): A202, pp. 1-8, DOI: dx.doi.org/10.5334/ijic.3512
- Neville C, Nguyen H, Ross K, et al. Lower-Limb Factors Associated with Balance and Falls in Older Adults: A Systematic Review and Clinical Synthesis. J Am Podiatr Med Assoc. 2020 Sep 1;110(5):Article_4. doi: 10.7547/19-143.
- Wylie G, Torrens C, Campbell P, et al. Podiatry interventions to prevent falls in older people: a systematic review and meta-analysis. Age Ageing. 2019;48(3):327-336. doi: 10.1093/ageing/afy189.
- Wang C, Goel R, Zhang Q, Lepow B, Najafi B. Daily Use of Bilateral Custom-Made Ankle-Foot Orthoses for Fall Prevention in Older Adults: A Randomized Controlled Trial. J Am Geriatr Soc. 2019;67(8):1656-1661. doi: 10.1111/jgs.15929.





