

By Paul Graham, B App Sc (Pod), FAAPSM
Natural forces affect every step we take. When the forces are too great for plantar tissues to handle, overloading occurs. Tissue overload can occur throughout the kinetic chain, wreaking havoc from end to end.
Over the past 15 to 20 years, research has focused on tissue overloading as the most common cause of overuse injury. Overload is caused by the forces of everyday life – push, pull, friction, gravity, and acceleration. These all generate forces on our bodies that can increase the risk of dysfunction and potential injury if the forces are higher than the tissues can withstand. These forces can be independent; but more commonly, they interact as we go through the movements of daily living.
Forces that affect us the moment we bear weight are the properties of gravity and the resultant ground reaction force (GRF) based on Newton’s third law: for every action, there’s an equal and opposite reaction.
It is important to understand how our body weight is transmitted onto the ground and how the GRF acts on our feet. Measures of plantar pressures allow us to see how those forces act on the foot. If the foot’s active and passive supportive mechanisms are overwhelmed or not stable enough to resist the GRF, we see compensation and dysfunction. These mechanisms are described in Kirby’s longitudinal arch load-sharing system1, combined with the recent studies of the role of the intrinsic muscle control by the central nervous system.2,3
Our body weight is primarily transmitted through our skeleton, which in turn is supported by connective tissues, allowing the forces to be dynamically shared during movement, particularly side-to-side movements.
Most humans have some asymmetry, which affects how the body functions and how body weight is transferred. Obvious asymmetries that affect function and plantar pressures include scoliosis, genu valgum or genu varum, internally or externally rotated lower legs, leg length differences, and high arch vs. low arch feet. As we age, asymmetry arises less from injuries, and more from adaptations and imbalances from everyday life.
Misalignments don’t necessarily mean that we’ll be injured, but they may contribute to injury by changing the pathways of force generation throughout the body. The red and yellow lines in Figure 1 represent the force placement. They are exactly equal in magnitude even though in the pictures it doesn’t show that.
While the foot’s default compensatory mechanism is pronation, depending on individual structure, compensation for a given condition may cause one person’s foot to roll outward, but it may cause another’s foot to roll inward.

Figure 1. Force Pathways & Asymmetry. In the patient with the knock knees (left), the weight bearing is more to the inside of the foot, making the foot roll in or pronate more. On the right, the patient’s weight will be placed depending on the level of compensation the body can offer.
Less obvious asymmetries that affect function are neuromuscular control and tone, neurological functions such as proprioception and information from other receptors, the origin and insertion of muscles creating joint movements, and the axis of joints, which also will influence joint movements.
Thanks to Kevin Kirby’s work describing it,4 a well-known axis of the foot is the subtalar joint (STJ) axis (Figure 2). If the axis is medially deviated, then GRF pressing under the foot will cause excessive pronation. If the axis is laterally deviated, then the same GRF pressing under the foot will cause excessive supination. And this is just one axis. When we talk about the midfoot joint axes, it gets more complicated with multiple axes, where each influences function.
Why the Body Compensates
Day-to-day activity creates forces that require compensation. Repeated dysfunctional patterns of movement create habits, which if continued, will create tissue adaptations that may positively or negatively affect function.
The busy-ness of life’s day-to-day activities often causes poor posture and function, and the repetitive nature leads to the risk of imbalance. While this commonly affects the trunk and head posture through changes in muscle balance and center of gravity (COG), it also can potentially alter gait and require compensation in the feet and legs. Based on all the gait styles you’ve seen in people walking by at the shopping center, it is clear the human body can compensate in several different ways.
Exercise, for example, is good for us, and to get stronger, we do need to push boundaries. Overtraining, however, is pushing the body beyond its limits. If we ignore the signs the body gives to not continue, this often results in injury or worse, a cycle of injury where the patient does what’s required to recover, then pushes themselves to get stronger as quickly as possible, resulting in reinjury. That cycle is real and pernicious, and all too common. Footwear heel height can also cause changes in the COG requiring postural shifts in the hips, knees, and extended torso to facilitate walking. Shoes should be worn as appropriate for the occasion and to provide appropriate support, as you wouldn’t wear high heels to run a marathon.
Being overweight increases the loading on all tissues and can exponentially increase loading on already overloaded tissues. Excessive weight can also cause an abducted gait, often with a transverse plane sway or waddling type of gait. If the compensation in the frontal and sagittal planes is insufficient for full compensation, other structural misalignments may occur.
 Surgery to address major injury, such as through sports, a car crash, workplace injury, or an arthritic joint, can make a world of difference to a patient’s quality of life. But we need to ensure that the outcome is the best possible and does not alter force transmission negatively.
Surgery to address major injury, such as through sports, a car crash, workplace injury, or an arthritic joint, can make a world of difference to a patient’s quality of life. But we need to ensure that the outcome is the best possible and does not alter force transmission negatively.
How the Body Compensates
To reduce the risk of injury, our body compensates by redistributing forces across several tissues by using the input from the neural sensors and then distributing the forces generated through muscle strength, connective tissue elasticity, and joint mobility.
The postural inputs include visual acuity from the eyes, balance from the vestibular canal system in the inner ear, tempo-mandibular-joint proprioception for head position, proprioception from the foot to provide a plane of reference for the rest of the body, and joint and soft tissue function feedback from mechanoreceptors and Golgi tendon organelles. With all this input, the brain uses muscles as a key part of the compensatory mechanism.
Muscles initiate movement and power and provide a significant stabilization force. As we age and our muscles atrophy, prolonged normal movements and activities can become painful as muscles fatigue. We need to consider low tone or high tone muscle issues, trigger points, neuromuscular disorders, et cetera, in how patients’ muscles will react with all this compensation.

While transmission of forces is primarily through the skeletal structure, the web of connective tissues such as fascia, ligaments, periosteum, and tendons provide stability and energy return making repetitive movement very energy efficient. This helps the passive supportive mechanisms of the body, such as in the foot.
Joint mobility, usually classified as joint stiffness in biomechanical terms, should be seen as describing not only the joint range of motion (ROM), but the characteristics of the capsular apparatus and associated soft tissues. People with stiff joints are less able to compensate, so the joint above and below are loaded more.
People with a greater ROM usually have greater capacity to compensate and redirect forces and often are not as symptomatic, even though their feet may look worse.

Figure 2. Significant Subtalar Joint Axis Displacement. When a foot that functions normally is in relaxed bipedal stance, resting slightly pronated from neutral position, the STJ axis passes through the posterior-lateral calcaneus posteriorly and above the first intermetatarsal space anteriorly (center, B). As the STJ undergoes pronation motion, the talus internally rotates and medially translates in relation to the plantar foot, causing the STJ axis to internally rotate and medially translate (left, A). As the STJ undergoes supination motion, the talus and STJ axis externally rotate and laterally translate in relation to the plantar foot (right, C). Reprinted from reference 1 with permission from the American Podiatric Medicine Association; all rights reserved.
Clinical Signs of Lack of Compensation
If there is not enough compensation to allow fluid gait due to significant structural asymmetry, functional imbalance or lack of muscle function or joint ROM, we will see various changes. For example, if a person complains of being clumsy, check their tibial torsion: Commonly, it will be internally rotated. Or maybe the foot and ankle joints are too stiff to allow compensation to occur. Or they may have a neuromuscular disorder that makes them less aware of spatial arrangements. If the body can’t compensate enough, the patient will indeed trip more easily than other people.
The abductory twist as the heel lifts off the ground when a person is walking is another example where the joints in the midfoot and the STJ don’t have enough ROM to compensate, and the dysfunction of the soft tissues restrict movement. So as the heel lifts, the torque that is being developed by the structure is shown by the twisting of the heel.
A side-to-side gait can occur if there are joint blockages or other features that reduce compensation in the frontal plane, which is the first plane to compensate, and in the sagittal plane, which is the second. So the body is only able to compensate through the transverse plane. That’s just one of many reasons why someone would have a side-to-side gait. But if you rule out all the other reasons, then you should consider the body’s ability or inability to compensate properly.
Similarly, if a person has muscle weakness or ankle, subtalar or midfoot joint restrictions, we’ll see some odd types of gait, particularly in running, as the body is forced to use every compensatory trick it can to help allow normal movement to occur. But if it is commonly occurring at the end of or toward the end of a sporting activity, it’s usually because the muscles are fatigued; they’ve shortened, and therefore are not providing their stabilization role and the level of compensation is not enough.
Pronation Is Not All Bad
In the past, pronation of the foot was seen as a bad thing. If you look at your bare foot while seated and it is non-weight bearing, most will see an arch. This describes the structure of your foot, which may have a higher arch profile or a lower arch profile. We need to be careful when describing any low arch profile as excessively pronated and thus pathological.
Now, if you stand up and look at the same foot, the chances are that it will be pronated or rolled in. The medial column of the forefoot will dorsiflex, the arch will elongate, and the whole arch will flatten. This describes the function of your foot as it compensates for what could be several reasons. It could be a structural factor – genu valgum, excessive external tibial torsion, ligament laxity. It could be from muscle contracture, posterior leg musculature, weak intrinsic or extrinsic musculature, or muscle dysfunction due to growth. It could be pain avoidance, leg length difference, painful corn, et cetera. All this is to say, a pronated foot simply tells us that the foot is compensating for something. Our challenge as clinicians is to discover what the body is compensating for.
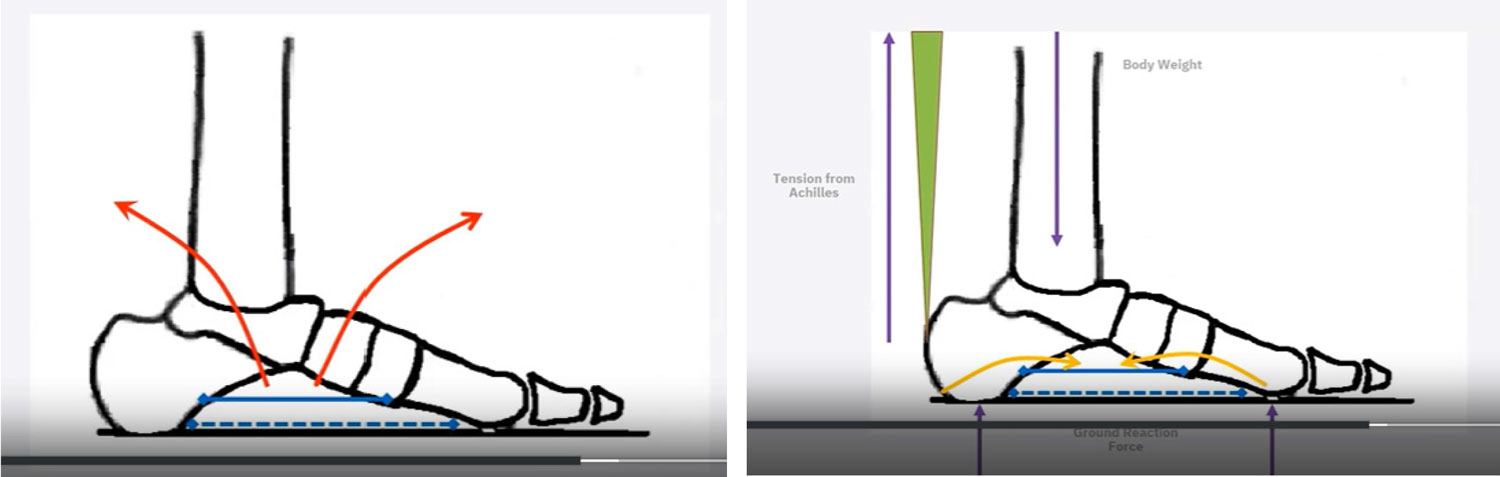
Figure 3. How the Foot Manages Force. A) The blue lines show how the foot and the medial and lateral longitudinal arch are stabilized by the intrinsic musculature and soft tissues. This dorsiflexes the rear foot and plantarflexes the forefoot, leading to the development and the maintenance of the arch structure shown by the red arrows. B) The gray line depicts the forces of body weight, the maroon line shows the tension from the Achilles, and the purple lines show the GRF applied underneath the foot. These tend to create the opposite rotation, lowering the arch of the foot and elongating the arch, as shown by the yellow arrows. Author’s drawing based on works by Kevin Kirby.5
Figure 3 shows how the foot manages the forces applied to it in normal activity. In cases where the auto-supportive mechanisms are substantial enough to resist the deforming forces, the foot will function normally. In cases where the active and passive-supportive mechanisms are just enough to resist the deforming forces, the person is at risk of injury. If they apply a greater level of force through the foot, they will overwhelm these mechanisms and can develop injury. This can occur with a major event such as a sporting injury, or more commonly over time, with aging and lifestyle choices (weight gain, loss of strength and mobility), so even a small increase in force may cause an injury.
The active and passive supportive mechanisms work through:
- stabilizing the calcaneocuboid joint, which facilitates peroneus longus weight transfer to the medial column from low gear to high gear,
- the windlass functions stabilizing the medial column on the midfoot,
- proper function of the first metatarsophalangeal joint into pre-swing phase, and
- contracture of the plantar connective tissues, pushing our toes into the ground and catapulting us over the planted foot.
McPoil and Hunt, in their 1995 research paper, “Evaluation and management of foot and ankle disorders, present problems and future directions”, proposed the use of a new model: the tissue stress model.6 They presented this as an effective alternative to the traditional Root et al7 biomechanics paradigm for evaluating and treating foot disorders. Since then, this theory has been validated by several other research studies as we have moved from a kinematic explanation of foot function to a more kinetic focus on the forces and the ability of the tissues to manage the load placed on them. When everyday forces are applied to tissues at high risk, such as in the patient with neuropathy, bony prominences, or poor circulation, they can also affect the ability of tissues to withstand high tissue loading and direct injury can occur. The breakdown of tissue, delayed healing rates, and possible requirement of amputation can be the dramatic result.
Directly Redistributing Forces

Figure 4. Presentation of a Patient with a Firm Forefoot Supinatus Condition Resulting in Bursitis. Above is a pressure map of a patient, captured using XSENSOR’s Intelligent Insoles | Clinical, with a firm forefoot supinatus, L/foot > R/foot. The XSENSOR Foot & Gait Clinical software provides data on the placement and intensity of loading and other vital statistics. It can also provide insight into the dysfunction through the midfoot joint complex based on the abnormal trajectory of loading. From this information we can institute a treatment strategy and then at an appropriate future progress review, assess if this strategy has made the desired changes in function as well as improvement of symptoms.
In our aim to prevent such tissue damage and ulceration or to heal those present, we need to address any circulatory issues as well as manage neuropathy, but we should never lose sight of the importance of assisting the body to manage the direct loading of those tissues.
In 2014, Waaijman et al showed that in-shoe peak pressure of less than 200 kPa and high adherence (> 80%) of wearing custom offloading insoles and footwear can reduce the risk of foot re-ulceration by over 50%, and that is significant.8
Foot dysfunction does not necessarily mean injury, but it may mean an increased risk of injury. For example, running places higher stress on tissues and when combined with uneven surfaces, injuries can occur.
How can we know the outcome of these forces?
Just as research has changed the way we understand how forces impact the foot and the outcomes, it also has questioned much of current practice. There are many studies that question the validity of non-weight bearing tests and weight bearing tests as well as recent studies that question the long-held foundations of our understanding of function and dysfunction. The most recent that comes to mind is Anja-Verena Behling et al 2023 paper, “Chasing footprints in time – reframing our understanding of human foot function in the context of current evidence and emerging insights”.9
The constantly changing landscape of theories regarding foot function, can make it difficult to be completely confident in exactly how to measure dysfunction and to know if what we are measuring is the root cause of the symptoms and concern the patient presents with.
“To measure is to know” -Lord Kelvin
We can measure the outcome of loading objectively, quickly, and easily by using plantar pressure mapping. Using this data, we can understand the loading characteristics of the tissues and whether the tissue loading occurs too fast. We can understand if it is poorly distributed or if the intensity is too much. We can analyze if the foot is pronating or supinating with validated techniques and the function of the rearfoot, midfoot, and forefoot joint complexes, all in dynamic weight bearing gait. With some equipment we can analyze this in running and with others, analyze these factors in the patient’s day-to-day life, removing any artificial barriers seen in clinical examination. We can also test balance and so much more.
If we use an in-shoe sensor, such as the XSENSOR Technology’s Intelligent Insole Clinical system, we can not only see this with our patient walking barefoot, but also in their shoes, replicating activities in their activities of daily living (ADL), sport, or work duties. This data presents a picture of the actual forces being placed on the foot during these activities and gives us the best window into why the patient is experiencing the concerns that they’ve come to see us with.
The XSENSOR Clinical Foot & Gait software provides further information such as where the loading is and the symmetry during the swing phase as well as the relationship between footsteps, distances, and timings. Everything you need to know to start understanding the complexities and components of the presenting condition so you can start to address them.
The information we gain from this equipment tells us what is happening, but it doesn’t tell us why. But by understanding what is happening, we can develop a hypothesis and then test it using dynamic plantar pressure to see in real time whether our hypothesis is supported by the relevant changes. While the examinations, our understanding of the complexities of foot function and the interaction of the rest of the body in all the various activities we do each day and their related forces loading the foot may not be perfect, plantar pressure analysis provides a reliable, objective, and repeatable window that we can depend on to gain the diagnostic insight and develop the most efficacious treatment strategy possible.
Paul Graham is an Australian podiatrist with a special interest in musculoskeletal conditions. He was awarded a Fellow of the Australasian Academy of Podiatric Sports Medicine in 1999. He offers training in plantar pressure analysis through his company Step Force. He has provided plantar pressure training in universities in Australia and is a Faculty of Manipal University in India. He has used plantar pressure analysis in his clinical practice for over 25 years for the diagnosis and treatment of gait and foot dysfunctions.
This is an excerpted transcript from a 4-part webinar series titled “Clinical Gait Assessment Using Plantar Pressure Analysis,” sponsored by XSENSOR Technology Corporation. A second excerpted transcript from the same series focused on Developing Treatment Strategies & Predicting Outcomes Using Plantar Pressure Analysis will appear in a future issue. To hear the entire webinar, visit https://learn.xsensor.com/clinical-gait-assessment-using-plantar-pressure-analysis-part-2.
- Kirby KA. Foot and lower extremity biomechanics IV: precision intricast newsletters, 2009-2013. Payson, AZ: Precision Intricast, Inc.; 2014. p. 31-4.
- Kelly LA, Cresswell AG, Racinais S, Whiteley R, Lickwark G. Intrinsic foot muscles have the capacity to control deformation of the longitudinal arch. J R Soc Interface. 2014;11:20131188.
- Kelly LA, Lichtwark G, Cresswell AG. Active regulation of longitudinal arch compression and recoil during walking and running. J R Soc Interface. 2015;12:20141076.
- Kirby KA. STJ axis location and rotational equilibrium theory of foot function. J Am Podiatr Med Assoc. 2001 Oct;91(9):465-87. doi: 10.7547/87507315-91-9-465.
- Kirby KA. Understanding Ten Key Biomechanical Functions Of The Plantar Fascia. Podiatry Today July 2016. Available at https://www.hmpgloballearningnetwork.com/site/podiatry/understanding-ten-key-biomechanical-functions-plantar-fascia. Accessed Jan. 19,2024.
- McPoil TG, Hunt GC. Evaluation and management of foot and ankle disorders: present problems and future directions. J Orthop Sports Phys Ther. 1995;21(6):381-8. doi: 10.2519/jospt.1995.21.6.381.
- Root ML, Orien WP, Weed JH. Normal and abnormal function of the foot. 1977, Clinical Biomechanics Corp: Los Angeles.
- Waaijman R, de Haart M, Arts MLJ, Wever D, Verlouw AJWE, Nollet F, Bus SA. Risk factors for plantar foot ulcer recurrence in neuropathic diabetic patients. Diabetes Care. 2014;37(6):1697-705. doi: 10.2337/dc13-2470
- Behling AV, Rainbow MJ, Welte L, Kelly L. Chasing footprints in time – reframing our understanding of human foot function in the context of current evidence and emerging insights. Biol Rev Camb Philos Soc. 2023;98(6):2136-2151. doi: 10.1111/brv.12999.





