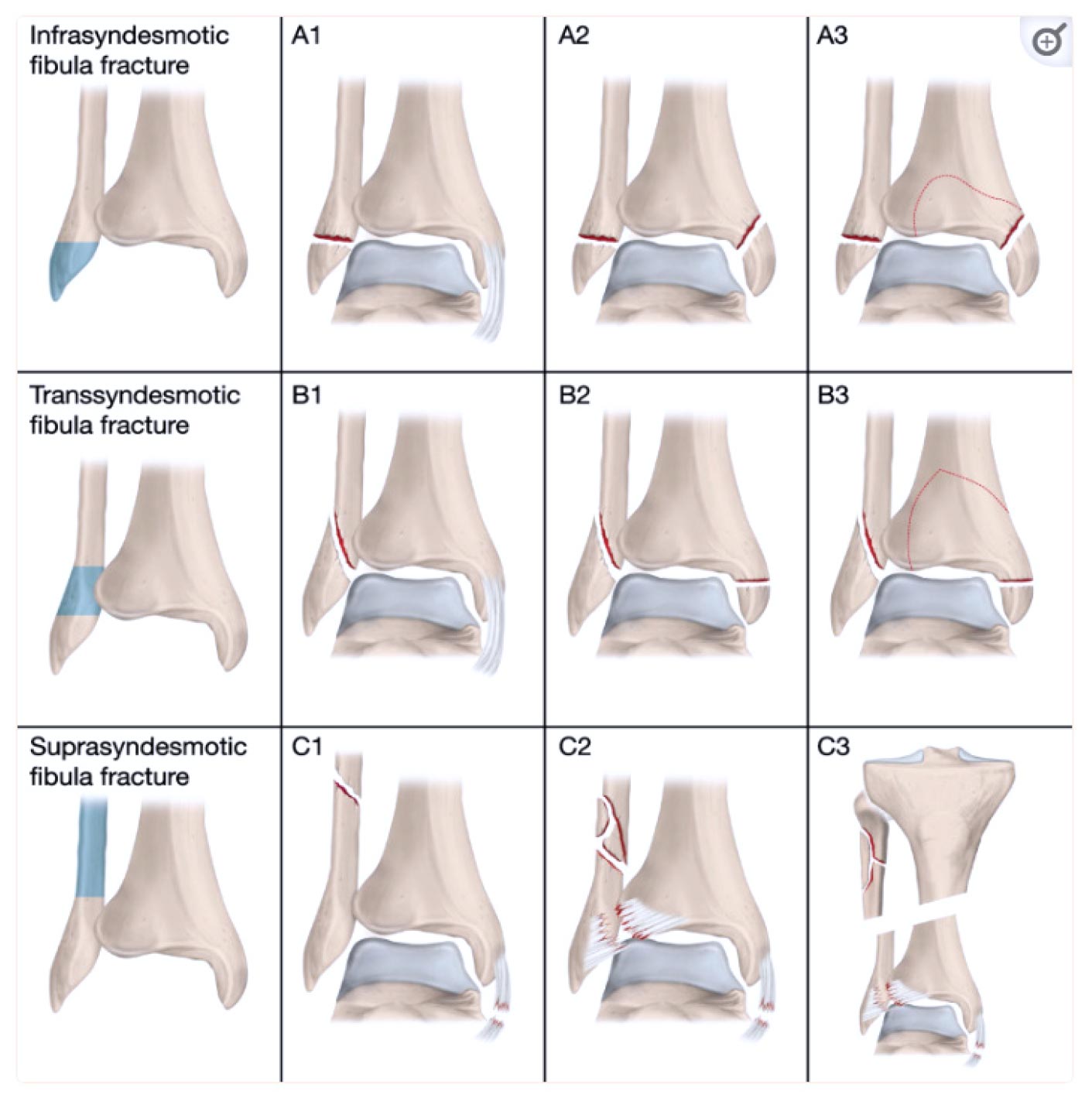
Figure 1. The AO/OTA classification of ankle fractures. Illustration by Pontus Andersson/Pontus Art Production
By Emilia Möller Rydberg, David Wennergren, Caroline Stigevall, Jan Ekelund, and Michael Möller
Large epidemiological studies are needed to elucidate the underlying injury mechanisms, the demographics of each fracture group, and the influence of sex and age on the sustained fracture.
Ankle fractures are the third most common type of fracture and range from simple avulsions that can be treated non-surgically to complex, open injuries that require multiple surgeries and long-term rehabilitation. An increasing incidence of ankle fractures, especially in the elderly, has been reported in several studies. Despite this, there is a lack of up-to-date, comprehensive epidemiological studies including all kinds of ankle fracture. Since 2012, the Swedish Fracture Register (SFR) has prospectively collected data on surgically and non-surgically treated ankle fractures, which have been classified according to the AO/OTA 2007 (Arbeitsgemeinschaft für Osteosynthesefragen/Orthopaedic Trauma Association) classification system. The aim of this study is to describe the epidemiology of ankle fractures between 2012–2022.
Methods
All ankle fractures registered in the SFR (AO/OTA44; Figure 1) from April 1, 2012–March 31, 2022, in patients over 16 years were included in this observational register study. Epidemiological data on age, sex, injury date, injury mechanism, injury type (high- or low-energy trauma), fracture classification, and type of treatment (surgical or non-surgical) were retrieved from the SFR. Information regarding fracture classification included the fracture type and group according to the AO/OTA classification, as well as side and open or closed fracture. For injury mechanisms, the 6 categories (simple fall, fall from a height, unspecified fall, traffic, miscellaneous, and non-traumatic) were used.
Results
During the 10-year study period, 56,439 patients sustained 57,443 ankle fractures. Bilateral fractures on the same injury occasion were seen in 156 (0.3%) patients and 845 (1.5%) patients sustained more than 1 ankle fracture (on different injury occasions). Of the latter group, 364 patients sustained another fracture to the same ankle and 481 patients fractured the contralateral ankle.
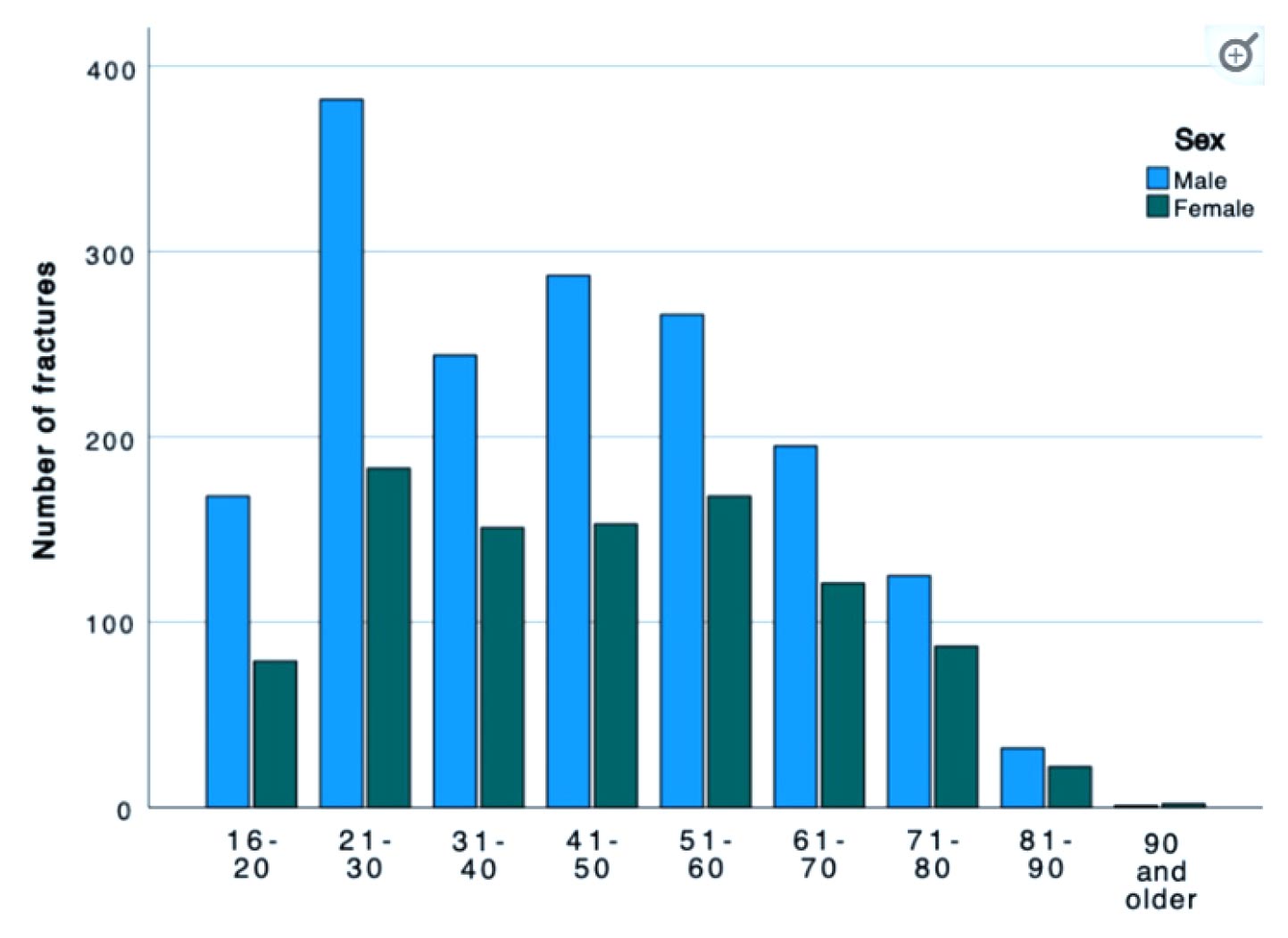
Figure 2. Age and sex distribution of ankle fractures sustained in high-energy trauma. Data shown for April 1, 2012–March 31, 2022.
Of all the fractures in this study, 13,685 (24.3%) were classified as AO/OTA type A, 35,892 (63.6%) as AO/OTA type B, and 6,837 (12.1%) as AO/OTA type C. Within the 3 AO/OTA types, fractures in group 1 (A1, B1, C1) dominated in all 3 types. The A1 group accounted for 69% of fractures, whereas A3 only accounted for 6% of fractures. The B1 group accounted for 52% of fractures (25% B2 and 23% B3). The C1 group accounted for 45% of fractures (27% C2 and 29% C3 (Figure 1). Another 953 fractures were unable to be classified, and 76 were pediatric fractures.
Women (61%) were affected more than men (39%). Only in the age groups below 40 do men have a higher frequency of ankle fractures than women. The mean age at the time of sustaining the fracture was 55 years. Men were found to be younger at the time of injury (mean age, 50 years) compared with the women who had a higher mean age of 58 years. The age and sex distribution for all ankle fractures peaked in total numbers between the ages of 50–70 years.
In total, 1.8% of all ankle fractures were open and were most frequent in the C2 group (5.4%, n = 9). The A1 group had the fewest open fractures (0.3%, n = 29). Open fractures were most common between the ages of 50–80 years. In those over 60 years, open fractures were more common in women than men, whereas men in the 21–50 years age group were more commonly affected. Open fractures of Gustilo–Andersson type II (wound > 1cm) were most common and 2/3 of this group were women. For patients older than 65 years, women dominated in all Gustilo–Andersson injury types. For patients under the age of 65 years, Gustilo–Andersson injuries types I and II were dominated by women, whereas men dominated the Type III injuries.
High-energy trauma was the underlying cause (4.7%, n = 2674) of all the ankle fractures in the study. The AO/OTA-A2 group had the highest proportion of high-energy trauma cases, whereas the AO/OTA-B1 group had the fewest high-energy trauma cases (2.5%, n = 460). High-energy trauma was most common in those age 21–30 years. In all age groups, men were more frequently injured by high-energy trauma than women (Figure 2).
The most common mechanism of injury for all ankle fractures and for each AO/OTA fracture group was a simple fall. Traffic injuries comprised a higher proportion of high-energy trauma (29.2%) and resulted more frequently in open fractures (4.7%) than other injury mechanisms. Fractures with a mechanism of injury that did not fit the other categories, such as sports injuries and fractures sustained in fights, and traffic injuries were associated with male sex and a lower mean age.
The number of ankle fractures peaked during the Swedish winter months (November to March), and was found to be driven by fractures sustained by simple falls. When analyzed by fracture type, the same seasonal variation was seen in B-type fractures but not for the other fracture types.
Discussion
The SFR offers a unique opportunity to conduct large epidemiological studies. The classification of ankle fractures, as well as other types of fracture, in the SFR has been validated and shown to have substantial accuracy. Compared with data from the Swedish National Patient Register (NPR), the SFR has been shown to constitute a complete and accurate source of information for epidemiological studies. One of the strengths of this study is that it is a multicenter study that includes ankle fractures of all kinds, treated both surgically and non-surgically and hospitalized and non-hospitalized. Another strength of this study is the length of the time period studied—10 years—which reduces the risk of variations in single years affecting the results.
Conclusions
This study presents the epidemiology of all AO/OTA types of ankle fractures in Sweden over a 10-year period. The study authors have shown that most ankle fractures are caused by a simple fall, affect women more than men, and occur during wintertime. These findings indicate that age-related skeletal fragility, as well as an increasing risk of simple falls in the elderly, may be risk factors. The study also demonstrates that men sustain their ankle fractures at a younger age and are more frequently injured by a high-energy trauma. As further shown, open ankle fractures are most common in women over the age of 60, but the severe open injuries more frequently affect men. This study will contribute to the planning of primary prevention for ankle fractures.
This article has been excerpted from “How to Measure Children’s Feet: 3D Foot Scanning Compared with Established 2D Manual or Digital Methods,” J Foot Ankle Res 16, 21 (2023). https://doi.org/10.1186/s13047-023-00618-y. Editing has occurred, including the renumbering or removal of tables, and references have been removed for brevity. Use is per CC BY 4.0 International License.





