

iStockphoto.com #1200116165
Foam rolling and roller massage, instrument-assisted soft tissue mobilization, and percussion massage are all the rage amongst consumers all along today’s fitness continuum. But what is the evidence base for the countless claims proponents offer? These authors provide a review of the peer-reviewed literature.
By Linden A. Lechner, BSc; Michael A. Rosenblat, PT, PhD(c), CEP; and Leanne M. Ramer, PhD
Over the last two decades, our understanding of fascia has shifted dramatically. Once assumed to be a passive connective tissue, fascia is now appreciated as a mechanically active, innervated, and dynamic system, interacting intimately with muscles to crucially influence their function.1 While an anatomical consensus and categorization of fascia remains elusive, the anatomical and functional association between fascia and skeletal muscle is commonly described as the myofascia (Figure 1).
In parallel with our increasing understanding of how fascia modifies movement, treatments targeting the myofascia have emerged as a popularized approach to rehabilitation. A subset of this pervasive practice is widely referred to as “self-myofascial release,” a collection of treatments that aim to address dysfunctions of skeletal muscle and connective tissue by the consumer at home. These are marketed to mimic the results of manual therapy, with an ever-increasing array of commercially available tools enticing and empowering consumers by creating the feeling that they have a therapist in the palm of their hand.
The term “self-myofascial release” emerged from the suggestion that these manipulations target clinically relevant and painful myofascial trigger points, caused by focal fibrous adhesions or constrictions. Despite the ubiquity of the term in training and rehabilitation, there is little (if any) evidence to support this hypothesis: while many interventions can alter myofascial tone, the mechanism likely has little to do with adhesion “release.”2 We therefore use the more general term myofascial manipulation to describe a growing collection of these techniques.
Of the available options targeting the myofascia, the most popular recent modalities include myofascial rolling, instrument-assisted soft tissue mobilization (IASTM), and percussion massage. These are abundantly and haphazardly used, but the data to support their benefits or best practice for use are only beginning to emerge. With most clients intrigued by or already performing at-home treatments targeting the myofascia, it is critical to understand what literature exists surrounding their efficacy in improving function and promoting recovery. In this article, we discuss the current literature surrounding the efficacy of these techniques, and further explore possible explanations for the outcomes we see with their application.
Foam Rolling and Roller Massage
The most accessible approach to lower-body myofascial manipulation for most clients is myofascial rolling using a foam roller or a hand-held roller massager (or “stick”). Since they are typically touted as recovery tools, rollers and sticks are often used after (or between bouts of) exercise. Massage with a foam roller involves rolling along the length of the targeted muscle or fascia on the device, using body weight to dictate the treatment pressure.3 The same concept applies to using a roller massager, except the pressure is applied using the upper limbs.
While myofascial rolling has become entrenched as common practice in training, rehabilitation, and physiotherapy, its efficacy is still being investigated in the literature, and the results remain far from clear. This ambivalence is due in part to substantial variability in the available data. The tools themselves vary widely in terms of their construction; they are available in a wide variety of shapes, sizes, densities, and textures. The dose of myofascial rolling inevitably varies with subcutaneous fat mass, as a thicker layer of subcutaneous fat hinders access to the deep fascia and distributes pressure over a larger surface area (Figure 1). In addition, the field is complicated by a lack of consensus on best practices; factors such as effective duration and timing of treatment targeting different regions remain ill-defined.
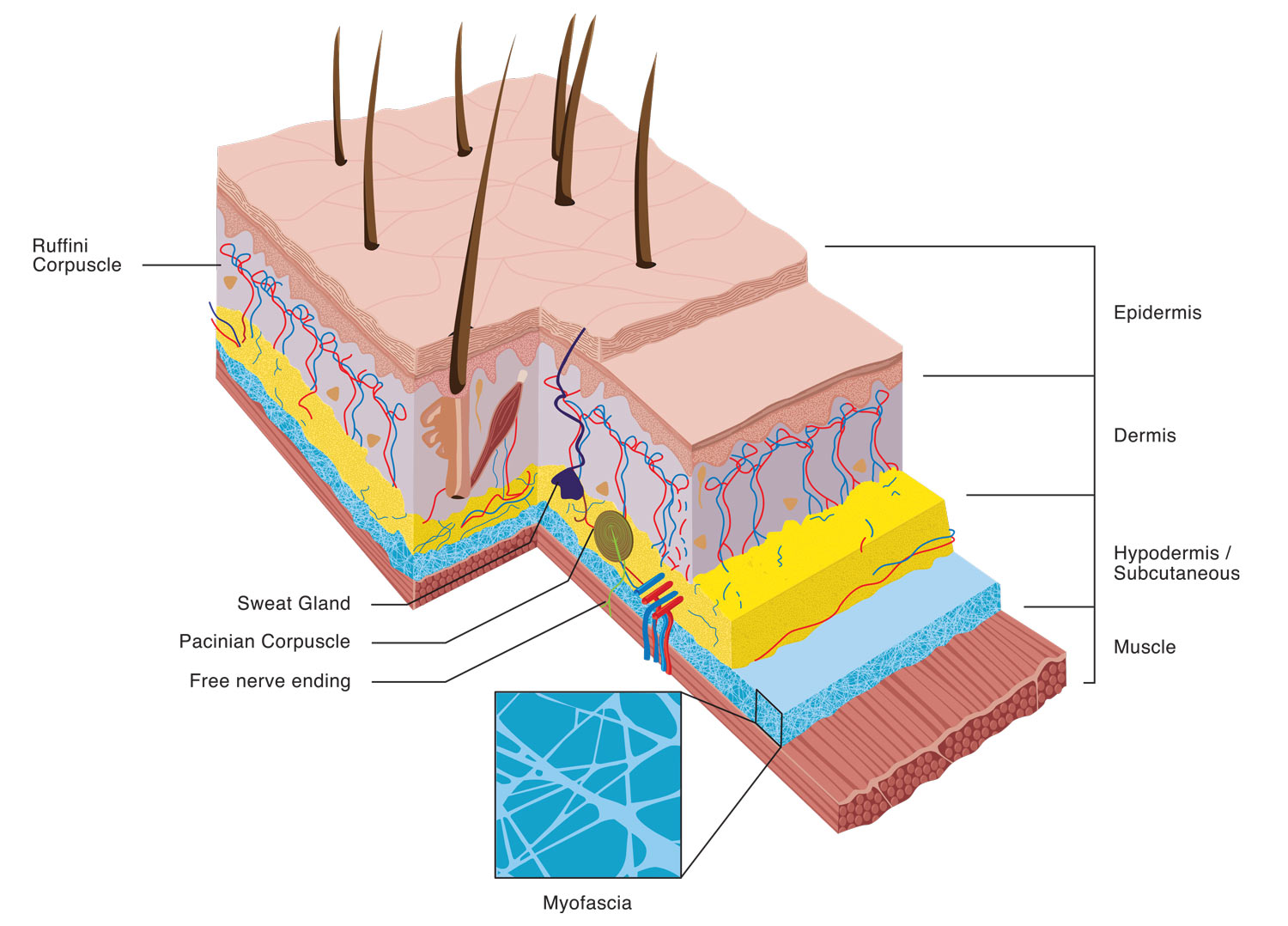
Figure 1. A schematic illustration of the skin and muscle, indicating the relative position of the myofascia, as well as specialized sensory end organs and free nerve endings. (Drawn and designed by Sam Wallbank.)
Purported benefits of myofascial rolling include improved range of motion, reduced muscle soreness, and improved athletic performance. In an attempt to provide some evidence-based consensus on best practice, we reviewed clinical studies that compared the efficacy of myofascial rolling to a control, using at least one of these three outcome measures.3 The studies that met all of our inclusion criteria (22) examined myofascial rolling applied to the gluteals, the hip flexors, the quadriceps, the hamstrings, the iliotibial band, and/or the plantar flexors.3
In addition to the heterogeneity of the available data, we were struck by the duration of myofascial rolling required to confer measurable benefit: we found that a minimum dose of 90 seconds per muscle was most reliable for reduction of muscle pain/soreness.3 The data on range of motion were less clear; while some evidence of improved range of motion was detected, there was no clear evidence of dose-response, and the variety of tests used to measure range of motion made comparison across studies extremely difficult. For similar reasons, we were unable to detect any effect of myofascial rolling on athletic performance, either detrimental or beneficial. Perhaps most notably, nearly all studies noted that beneficial effects on pain and range of motion were transient (lasting <24–72 hours), strongly suggesting that myofascial rolling produces only short-term recovery.
The issue of whether and how myofascial rolling alters performance remains contentious. In a 2019 study, Laffaye et al examined effects of myofascial rolling immediately following high-intensity interval training (HIIT). On the treated side, participants performed foam rolling over the iliotibial band and the quadriceps, aiming to achieve a 7/10 for pain intensity on the visual analog scale.4 Foam rolling produced a significant reduction in muscle soreness and increased hip range of motion (measured at 48 hours after exercise), but conferred no detectable benefit on recovery of performance.4 This study supports the use of myofascial manipulation for reducing soreness rather than regaining initial performance following HIIT.
Several recent studies address specific questions surrounding myofascial massage. For example, Cheatham and Stull examined the effects of foam roller surface texture.5 They found that two-minutes of quadriceps rolling with a textured (GRID) roller produced larger increases in knee range of motion and quadriceps pressure pain threshold than a less-textured (multi-level) roller or a smooth roller. These effects were measured immediately after foam rolling and without exercise; however, this study provides evidence from a well-controlled setting that the texture of myofascial manipulation tools alters the effects of treatment.5
Recent research is also exploring the efficacy of myofascial rolling as a conjunct recovery practice. Oranchuk and colleagues compared the effects of foam rolling, superficial heat, and both together on hamstring flexibility (measured via passive straight leg raise) in 22 female collegiate lacrosse and soccer athletes.6 Interestingly, they found similar improvements in hamstring flexibility (ie, increased hip flexion) with either superficial heat or foam rolling. Together, combined superficial heat and foam rolling produced the greatest benefits for hamstring flexibility, but the effect was not significantly different than superficial heat applied alone.6 This raises the important question of whether myofascial rolling produces additional benefits over established recovery practices, particularly those that are non-invasive and low-cost (or free).
Instrument-Assisted Soft Tissue Mobilization
Instrument-assisted soft tissue mobilization (IASTM) refers to a wide range of techniques using metal implements designed to provide a mechanical advantage for deep tissue penetration.7 This practice has its roots in Gua sha, a traditional Chinese therapy that aims to “scrape or rub the surface of the body to relieve blood stagnation.”8 Accordingly, the procedures are often described as “scraping massage,” and are performed using an ever-increasing array of specialized instruments, including commercially available lines such as Graston, Técnica Gavilán, Adhesion Breakers, and many others. The tools for IASTM are expensive, in the price range of thousands of dollars for a 6-piece set; this marketing is often coupled with for-profit continuing education courses.8
Despite its widespread use, there is little evidence-based consensus around any aspect of IASTM, including indications for its use or its efficacy.7 Some research is slowly emerging, but the field is plagued by the same issues that surround foam rolling and roller massage, namely, a variability in tools, techniques, and timing of treatment, as well as treated populations. In addition to these confounds, IASTM (as high-pressure shearing treatment) involves more risk for tissue damage than its rolling counterparts. Recent expert commentary highlights the importance of safety guidelines and contraindications for IASTM; an example of the ongoing debate across practitioners is treatment-induced effects on the skin.7 Some IASTM treatments produce ecchymosis (bruising) and/or petechiae (reddish spotting); in fact, among some practitioners this remains a goal of treatment. However, an increasing number of practitioners regard this as potential iatrogenic tissue damage, which should be avoided or at least healed prior to resuming treatment.7
The data on effects of IASTM have been summarized in 2 recent and comprehensive literature reviews:7,9 in both, the gap between evidence for and implementation of IASTM is obvious. Tentative hypotheses surrounding the benefits of IASTM suggest that it stimulates inflammation and the breakdown of scar tissue, promoting healing and functional normalization.10 However, data demonstrating either mechanistic or clinically meaningful benefits are limited. In fact, a study of human gastrocnemius found no increase in intramuscular inflammatory markers in muscle biopsies collected 24 hours after IASTM.11 Most available evidence of efficacy, while intriguing, is derived from small studies, many conducted with a no-treatment control, rendering the findings ambiguous. When the quality of research design is considered—including discerning between statistically significant and clinically meaningful effects—and the potential for bias is acknowledged,7 the current evidence does not support the use of IASTM as an effective treatment to improve client or patient outcomes. These findings are seemingly contradictory to the claims found on the Graston website which boast that Graston tools are effective in “treating all soft tissue conditions, whether they are chronic, acute or post- surgical… restoring range of motion, eliminating pain, and restoring normal function.”12 While it is clear that more research is required, IASTM will have to emerge as obviously superior to roller massage to justify its high cost and potential for tissue damage. This is epitomized in a recent study that directly compared the effects of IASTM and a roller massage stick on hamstring range of motion and concluded that “IASTM and the roller massage stick were equally effective immediately and over time, but the roller massage stick is more affordable.”13
Percussion Massage
Percussion massage therapy is rapidly gaining popularity among professional and recreational athletes. Multiple tools (or “guns;” Figure 2) have been marketed to, and widely adopted by, athletes to help improve their performance or sport-related recovery. The major companies in this market, including Hyperice Hypervolt, Theragun, and TimTam, have developed percussion massagers for commercial purposes. As a trailblazing technique purported to promote recovery, it is no surprise that percussion massagers are somewhat expensive, typically falling somewhere in-between the relatively affordable tools for myofascial rolling and the high-priced tools and training for IASTM. For example, the TimTam massager is marketed at ~$300, the Hyperice Hypervolt at ~$350, and the Theragun Pro at ~$410.14
In part due to their relatively recent appearance, data demonstrating the clinical benefits or physiological effects of any device for percussion massage are slim-to-none. Dozens of online articles boast that these tools stimulate, inter alia, muscle fibre repair, improve lymphatic and venous flow, and break down intramuscular or myofascial adhesions. However, there is no evidence in the peer-reviewed literature to support any of these claims. There is also no evidence to support the safety of this practice, nor are their guidelines to limit intensity or duration of percussion.
Given the new-found popularity of percussion massage, our laboratory recently purchased one of these devices to investigate its efficacy in recreational athletes. So far, we have only anecdotal (athlete-reported) evidence to support acute percussion massage for reduction of post-exercise muscle soreness. We have institutional ethical approval to investigate this hypothesis, comparing percussion massage to standardized stretching and myofascial rolling, using both range-of-motion and muscle soreness reported via the visual analog scale. We hope these and similar studies will help close this gap between evidence-based therapy and implementation.

Mechanisms of Myofascial Manipulation

Figure 2. Application of percussion massage.
If “myofascial release” is a misnomer, and soft tissue adhesions are not affected by myofascial manipulation, what might underlie the benefits of and/or commitment to these practices? Like many interventions, it is likely that benefits of myofascial manipulations are produced by a combination of effects. Certainly, the painful and/or pleasurable experience of myofascial rolling, IASTM, and percussion massage produces a perceived benefit for some clients. This may produce a placebo effect of treatment, or it may simply be enjoyable, thus improving compliance with some type of active recovery routine. While most studies report that myofascial manipulation is superior to untreated control, data demonstrating benefits beyond well-established approaches to recovery remain limited. This is under-scored in a recent meta-analysis of 26 studies examining acute effects of foam rolling on range of motion: foam rolling was superior to no-exercise control, but comparable to stretching.15
Rather than altering the structural or mechanical properties of the deep fascia, recent data suggest that neural effects of manipulations targeting the myofascia are paramount to changes in perception and range of motion. A detailed discussion of these collective findings and hypotheses is eloquently presented by Wiewelhove and colleagues.16 One proposed mechanism is the cutaneous mechanoreceptor’s contribution to local relaxation.2 A variety of specialized mechanoreceptors—Merkel receptors, Meissner and Pacinian corpuscles, and Ruffini endings—have end-organs in the skin (Figure 1). Unlike the relatively deep myofascia, these cutaneous and subcutaneous receptors are readily accessible to treatment applied to the skin. While these receptors differ in their receptive field size, adaptation patterns, and duration of response, their primary function is facilitating proprioception; it is likely they underlie a neural inhibition response for muscle relaxation.2 Specifically, Ruffini and Pacinian corpuscles may reduce global sympathetic activity, thus decreasing muscle tautness.2 All 4 of these receptors should display increased activity during delivery of myofascial manipulation. Additionally, general massage can activate the parasympathetic nervous system universally. Both this reduction of the sympathetic drive from receptors and increase in parasympathetic from massage, may in part, explain the reduction in pain with myofascial manipulation.2
In addition and intriguingly, recent data demonstrate that the deep fascia itself is innervated, containing peptidergic-free nerve endings (putative nociceptors).17 This raises a crucial question: does myofascial manipulation mobilize the myofascial unit, or does it simply dampen the nociceptive response, allowing those with limited range of motion due to pain to move beyond their baseline measurements? The neural aspects of myofascial manipulation have captured our attention and remain an open and important area of research, with implications for a variety of health practitioners and their clients who engage in these practices at home.
Provided myofascial manipulation does not produce tissue damage or compromise performance (which remains open to debate), the most pressing questions are at least two-fold. First, does any form of myofascial manipulation out-perform well-established recovery practices, including stretching? If so, are low-cost, accessible manipulations (such as myofascial rolling) comparable in efficacy to higher-cost manipulations? Clinically and practically, it is crucial to consider the disadvantages of any ineffective treatment, including costs, safety risks, and delaying access to beneficial treatment. At present, there is little-to-no high-quality evidence demonstrating clear benefits of myofascial manipulation over well-established recovery practices. There are also no evidence-based guidelines for choosing or applying a method of treatment targeting the myofascia. Practitioners and coaches should be transparent with their clients and acknowledge these limitations: myofascial manipulations may confer benefit, but there is no good evidence that this benefit exceeds traditional approaches to recovery.
Linden A. Lechner, BSc, is a Research Assistant in the Department of Biomedical Physiology and Kinesiology, Faculty of Science, at Simon Fraser University in Burnaby, BC, Canada.
Michael A. Rosenblat, PT, PhD(c), CEP, is a Lecturer in the Department of Biomedical Physiology and Kinesiology, Faculty of Science, at Simon Fraser University in Burnaby, BC, Canada, and a PhD Candidate in the Department of Exercise Science, Faculty of Kinesiology and Physical Education, at University of Toronto, in Toronto, ON, Canada.
Leanne M. Ramer, PhD, is a Lecturer in the Department of Biomedical Physiology and Kinesiology, Faculty of Science, at Simon Fraser University in Burnaby, BC, Canada.
- Krause F, Wilke J, Vogt L, Banzer W. Intermuscular force transmission along myofascial chains: A systematic review. J Anat. 2016;228(6):910-918.
- Behm DG, Wilke J. Do Self-Myofascial Release Devices Release Myofascia? Rolling Mechanisms: A Narrative Review. Sports Med. 2019;49(8):1173-1181.
- Hughes GA, Ramer LM. Duration of myofascial rolling for optimal recovery, range of motion and performance: a systematic review of the literature. Int J Sports Phys Ther. 2019;14(160):845-859.
- Laffaye G, Da Silva DT, Delafontaine A. Self-myofascial release effect with foam rolling on recovery after high-intensity interval training. Front Physiol. 2019;10:1287.
- Cheatham SW, Stull KR. Roller massage: comparison of three different surface type pattern foam rollers on passive knee range of motion and pain perception. J Bodyw Mov Ther. 2019;23(3):555-560.
- Oranchuk DJ, Flattery MR, Robinson TL. Superficial heat administration and foam rolling increase hamstring flexibility acutely; with amplifying effects. Phys Ther Sport. 2019. doi:10.1016/j.ptsp.2019.10.004
- Cheatham SW, Baker R, Kreiswirth E. Instrument assisted soft-tissue mobilization: a commentary on clinical practice guidelines for rehabilitation professionals. Int J Sports Phys Ther. 2019;40:213-217.
- Nazari G, Bobos P, MacDermid JC, Birmingham T. The effectiveness of instrument-assisted soft tissue mobilization in athletes, participants without extremity or spinal conditions, and individuals with upper extremity, lower extremity, and spinal conditions: a systematic review. Arch Phys Med Rehabil. 2019;100(9):1726-1751.
- Seffrin CB, Cattano NM, Reed MA, Gardiner-Shires AM. Instrument-assisted soft tissue mobilization: A systematic review and effect-size analysis. J Athl Train. 2019;54(7):808-821.
- Kim J, Sung DJ, Lee J. Therapeutic effectiveness of instrument-assisted soft tissue mobilization for soft tissue injury: mechanisms and practical application. J Exerc Rehabil. 2017;13(1):12-22.
- Vardiman JP, Siedlik J, Herda T, et al. Instrument-assisted soft tissue mobilization: effects on the properties of human plantar flexors. Int J Sports Med. 2015;36(3):197-203.
- Graston Technique, LLC. https://grastontechnique.com/Patients/. Accessed May 7, 2020.
- Lee J, Young A, Erb NJ, Herzog VW. Acute and Residual Effects of IASTM and Roller Massage Stick on Hamstring Range of Motion. J Allied Health. 2020;49(1):e51-e55..
- Capritto A. Theragun, Hypervolt, TimTam: The best percussive massage gun for 2020. CNET:Health and Wellness. Available at https://www.cnet.com/health/best-percussive-massage-gun-2020-theragun-hypervolt-tim-tam/. Accessed May 7, 2020.
- Wilke J, Müller AL, Giesche F, Power G, Ahmedi H, Behm DG. Acute effects of foam rolling on range of motion in healthy adults: a systematic review with multilevel meta-analysis. Sports Med. 2020;50(2):387-402.
- Wiewelhove T, Döweling A, Schneider C, et al. A meta-analysis of the effects of foam rolling on performance and recovery. Front Physiol. 2019;10:376.
- Mense S. Innervation of the thoracolumbar fascia. Eur J Transl Myol. 2019;29(3):8297.





