
 Because power in baseball pitchers is generated from the feet through the core to the throwing arm, the study of stride length and its impact on pitching performance may help define an optimum technique that better protects pitchers from upper extremity injuries.
Because power in baseball pitchers is generated from the feet through the core to the throwing arm, the study of stride length and its impact on pitching performance may help define an optimum technique that better protects pitchers from upper extremity injuries.
By Ryan L. Crotin, PhD, and Dan K. Ramsey, PhD
Research focused on baseball pitching biomechanics traditionally concentrates on throwing-arm dynamics, emphasizing joint kinematics and kinetics to describe the throwing motion and related injury mechanisms. Primary etiologies are repetitive high-magnitude moments and forces imparted on the shoulder and medial elbow during the late cocking, acceleration, and deceleration phases of the pitching delivery.1 Despite advances in sport biomechanics that provide a better understanding of throwing-arm dynamics, throwing arm injuries continue to escalate across all levels of competition,2-6 with concomitant increases in the number of surgical interventions and postoperative rehabilitations performed.7-11
A new approach, however, may be to focus the analysis on lower extremity biomechanics, given that joint powers transition up the kinetic chain, beginning with ground contact. Ground reaction forces that are imparted on the drive (trailing) foot and stride (lead) foot sequentially act as principal power generators that transfer up the link segments to the trunk, throwing arm, and hand,12 which are likely influenced by the length of the pitching stride.13 Therefore, the study of stride length and its impact on pitching performance may help define an optimum technique that better protects pitchers from injury.
Stride length and its determination
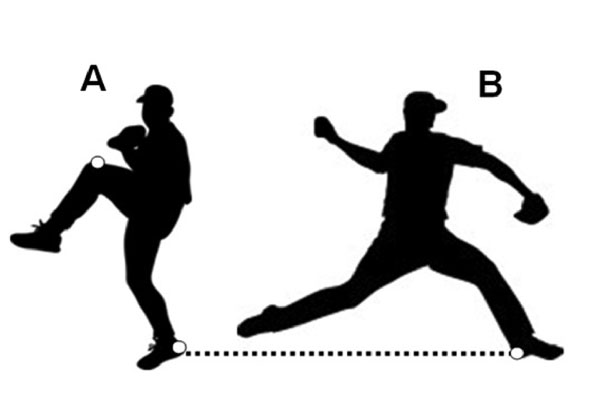
Figure 1. Stride length calculated as the horizontal distance between calcaneal markers from peak knee height (A) to stride foot contact (B). The point at which vertical ground reaction force exceeds 5% of body height is the instant of stride foot contact. (Reprinted with permission from reference 16.)
Stride length is an important component of the baseball pitching delivery for two key reasons: it’s necessary for establishing the timing of kinetic chain events and appropriating mechanical energy from the lower body and transitioning it to the throwing hand.14,15
Commonly described as the horizontal distance from the calcaneus of the trailing foot at peak knee height to the calcaneus of the lead foot at the instant of ground contact, stride length is best measured using a motion-capture system integrated with force plates; assessment of the vertical ground reaction force at landing can accurately depict onset of stride foot contact (SFC)16 (Figure 1). Stride length is also typically normalized to percent of body height (%BH) to enable comparisons across cohorts.16-21
Stride length throughout skill development
Development of overhead throwing proficiency is dependent on stride length. In particular, stride length has been associated with ball velocity, accounting for nearly 70% of variation in ball velocity among novice pitchers.22 Proficient pitching mechanics involve a contralateral stride length greater than 50% of body height, whereas shorter strides and those characterized by an ipsilateral step for initiation of throwing have been shown to reduce ball velocity.22 Strides greater than 50% of body height reportedly influence proximal pelvic-trunk kinematics, as evidenced by higher linear and angular pelvic and trunk velocities and increased hip to shoulder separation angles at stride foot contact, which suggests that greater trunk counter-rotation relative to the pelvis can augment elastic prestretching of the intrinsic musculature from the lead hip to the throwing shoulder prior to maximal external shoulder rotation or cocking of the throwing arm.22

Figure 2. Traditional and lower body pitching delivery phases transitioned by discrete events. Windup to peak knee height initiates the delivery, in which the pitcher generates forward momentum in single support until stride foot contact, which refers to the generation phase. Following foot contact, forward momentum is braced, then transferred to pelvic-trunk rotation prior to maximal external shoulder rotation, which refers to the brace-transfer phase in double support. Following maximal external shoulder rotation, acceleration of the throwing arm occurs until ball release; afterwards, deceleration transitions to follow-through in single support.
Stride lengths vary across the spectrum of pitcher ability in part because of differences in physical anthropometry and maturity, in particular, the development after puberty of greater segmental lengths, masses, and muscular strength that combine to lengthen one’s stride.22 Professional baseball pitchers adopt stride lengths between 80% and 85% of body height,20,23 whereas collegiate and amateur pitchers utilize shorter strides,24,25 which may relate to disparities in ball velocity attributes. Curveball pitching, in which the pitcher releases the baseball at a greater height than when a fastball is pitched, elicits a greater downward plane of ball movement20 and has also been associated with reduced stride lengths up to of 5% of body height compared with fastball pitching,23 which suggests pitchers have innate abilities that allow them to vary stride length when throwing different types of pitches.4,26,27 It is unknown how pitchers innately adopt self-selected stride lengths throughout skill development; that process could be related to coaching, biomechanical evaluation, the pitcher’s efforts to generate maximal pitching velocity, or simply height and segment anthropometrics.
Stride length influences on kinematics
Traditional pitching phases occur from onset of the windup through ball release and are separated by five hallmark events: peak knee height (PKH), SFC, maximal external rotation (MER) at the shoulder, ball release (BR), and maximal internal rotation (MIR) at the shoulder.1,15,19,28
During the windup, the stride leg (contralateral to the throwing arm) is lifted to PKH as the pitcher produces mechanical energy through ground reaction forces to direct the center of gravity toward home plate.15 Lower extremity movement continues with the single support phase, or generation phase, of the pitching cycle, in which the drive foot is in contact with the ground while the stride foot is airborne until SFC. This is the phase in which the linear energy generated by the drive leg is greatest, moving the center of mass of the whole body forward.12,13 Longer strides tend to increase the duration of the generation phase (PKH to SFC), whereas shorter strides result in earlier onset of SFC, thereby shortening the time in single support.29 Following SFC, the drive foot and stride foot are both in contact with the ground in the double support, or brace-transfer phase (SFC to MER) of the pitching cycle, in which linear energy generated by the drive leg is braced by the lead leg and then transferred to pelvic-trunk rotation (Figure 2).
As the lower body goes through the single support and brace-transfer phases of the pitching cycle, the arm motion goes through the cocking phase. The early cocking phase refers to the beginning of shoulder external rotation and horizontal abduction, which occurs during single support. The late cocking phase, in which maximum shoulder external rotation is achieved, occurs during double support.
The duration of the brace-transfer phase is inversely related to time spent in single support and, in turn, to stride length. A shorter brace-transfer phase is associated with longer strides, while shortening the stride increases double support time.29
The brace-transfer phase is followed by the acceleration phase, in which the throwing arm moves from maximal external rotation to the point of ball release and the lower body transitions from double support back to single support, this time with the body weight over the stride leg.
Although stride length does not influence timing during the acceleration phase, when the throwing arm is most active from MER until ball release, stride length may affect intersegmental momentum transfer and trunk kinematics prior to maximal cocking of the throwing arm in ways that may, in turn, affect injury risk.30-32
Stride length influences on kinetics
At the origin of the kinetic chain are ground reaction force (GRF) profiles, which have been shown to have a distal effect on linear wrist and ball velocity during pitching.12 Positive correlations were shown among drive leg vertical forces at peak push off (r² = .74), stride foot posterior shear force (r² = .86), and stride foot vertical force at BR (r² = .70).12 The timing of peak drive leg GRF also had an effect on ball velocity, whereby slower throwing pitchers demonstrate earlier GRF peaks during single support.33 Currently unknown is whether or how stride length is associated with timing of peak GRF in the drive leg during the generation phase and the corresponding braking GRF of the stride leg, which can impact distal joint biomechanics in succession.20,22,34,35
The lower extremity kinetics of pitching are not well-documented, and lead knee kinematics during the acceleration phase constitutes the breadth of lower extremity research in baseball pitchers.17-20 During fastball pitching, the bracing kinematics of the lead knee contribute to maximum kinetic energy in the throwing hand and facilitate linked-segment momentum transfers following SFC.20,34 Stride length is anticipated to impact lead knee joint kinematics and kinetics throughout the double support phase, from SFC to ball release.12,14,15,36 Shorter strides (less than 75% of body height), which typically are associated with earlier SFC onsets,29 are believed to result in less effective stride knee mechanics during the brace-transfer phase, altering intersegmental momentum transfers from the ground to the throwing hand, which can ultimately lower ball velocity.19,37 Earlier timing of stride foot contact can have serious injury implications if the angular pelvic-trunk kinematics are affected; latent opening of the pelvis, as well as early opening of the trunk, reportedly can adversely affect shoulder and elbow kinetics.30,31,38
Metabolic cost
Over the course of a game, pitchers may adopt coordinated biomechanical changes to alter their throwing mechanics to maintain or increase fastball velocities. Researchers have suggested these compensations result from tissue microtrauma and elevated physiological costs (overexertion), which has been related to increasing workloads (pitch counts) and pitch frequency (innings, games).2,6,19,26,27,39 It is possible that declines in ball velocity may protect against injury, and that altering throwing mechanics to maintain performance in response to overexertion and pain may increase stress on the throwing arm.2,6,19,26,27,39
When compensatory throwing mechanics alter joint reaction forces such that the magnitude, rate, and frequency of loading are amplified, the internal soft tissues may be overwhelmed.1,3 A 36-fold increase in injury risk has been reported in pitchers who competed in a “fatigued” state,40 further evidence that competing while overexerted likely increases repetitive stress on the throwing arm, which may be linked to biomechanical compensations.

Many pitchers adopt an extended stride to compensate for reduced throwing speed. But new findings suggest that increasing stride length by 25% may be more physiologically demanding than a pitcher’s preferred stride length, as higher perceived exertion scores with concomitant increases in heart rate and salivary alpha amylase concentrations (a common biomarker for stress) reflected greater stress compared with a 25% reduction in stride.16 In contrast, shortening the stride by 25% was associated with a reduction in mean pitching heart rate by 11 beats per minute, a 5% improvement in recovery capacity between innings, and lower salivary cortisol concentrations. Despite these adaptations, linear hand and ball velocities remained equivalent for all three stride lengths, suggesting that pitch velocity performance can be maintained despite energetic differences in compensatory lower body mechanics.
Perhaps these findings have implications for training, given that strides longer than 75% of body height, which are common among Major League Baseball pitchers, require considerable lower extremity conditioning to mitigate fatigue and accompanying biomechanical compensations.
Future direction
The effects of stride length on intrinsic lower extremity mechanics and intersegmental momentum transfers to the pelvis and torso remain unknown, and inconsistencies in stride length could potentially impair synchronous proximal-distal trunk-throwing arm mechanics.14,22 On the other hand, perhaps, by modifying stride length, tensile stress-strain responses affecting the throwing arm can be lessened.37,38,41,42 In light of this, future studies should focus on providing a greater understanding of how stride length impacts the kinetic chain in the context of ground reaction forces, joint biomechanics, and momentum transfer.
Ryan L. Crotin, PhD, is a baseball operations specialist consultant with Major League Baseball’s Baltimore Orioles whose research focuses on injury mechanisms and evidenced-based practices on injury prevention through strength training. Dan K. Ramsey, PhD, is assistant professor in the Department of Exercise and Nutrition Sciences at the University at Buffalo, NY, where his research bridges the gap between prevention and treatment of musculoskeletal injury, disease, and disability.
Disclosure: No external funding or benefits have or will be received from any commercial party related directly or indirectly to the subject of this article. None of the authors report a professional relationship with a company or manufacturer that will benefit from the results of the present study.
1. Fleisig GS, Andrews JR, Dillman CJ, Escamilla RF. Kinetics of baseball pitching with implications about injury mechanisms. Am J Sports Med 1995;23(2):233-239.
2. Conte S, Requa R, Garrick J. Disability days in major league baseball. Am J Sports Med 2001;29(4):431-436.
3. Dick R, Sauers EL, Agel J, et al. Descriptive epidemiology of collegiate men’s baseball injuries: National Collegiate Athletic Association Injury Surveillance System, 1988-1989 through 2003-2004. J Athl Train 2007;42(2):183-193.
4. Fleisig GS, Weber A, Hassell N, Andrews JR. Prevention of elbow injuries in youth baseball pitchers. Curr Sports Med Rep 2009;8(5):250-254.
5. Fleisig GS, Andrews JR, Cutter GR, et al. Risk of serious injury for young baseball pitchers. Am J Sports Med 2011;39(2):253-257.
6. Posner M, Cameron KL, Wolf JM, et al. Epidemiology of major league baseball injuries. Am J Sports Med 2011;39(8):1676-1680.
7. Andrews JR, Whiteside JA, Buettner CM. Clinical evaluation of the elbow in throwers. Oper Tech Sports Med 1996;4(2):77-83.
8. Burkhart SS, Morgan CD, Kibler WB. The disabled throwing shoulder: spectrum of pathology. Part I: pathoanatomy and biomechanics. Arthroscopy 2003;19(4):404-420.
9. Burkhart SS, Morgan CD, Kibler WB. The disabled throwing shoulder: spectrum of pathology. Part II: evaluation and treatment of SLAP lesions in throwers. Arthroscopy 2003;19(5):531-539.
10. Burkhart SS, Morgan CD, Kibler WB. The disabled throwing shoulder: spectrum of pathology Part III: The SICK scapula, scapular dyskinesis, the kinetic chain, and rehabilitation. Arthroscopy 2003;19(6):641-661.
11. Osbahr DC, Swaminathan SS, Allen AA, et al. Combined flexor-pronator mass and ulnar collateral ligament injuries in the elbows of older baseball players. Am J Sports Med 2010;38(4):733-739.
12. MacWilliams B, Choi T, Perezous M, et al. Characteristic ground-reaction forces in baseball pitching. Am J Sports Med 1998;26(1):66-71.
13. Werner SL, Guido JA, McNeice RP, et al. Biomechanics of youth windmill softball pitching. Am J Sports Med 2005;33(4):552-560.
14. Lin HT, Su FC, Nakamura M, Chao EYS. Complex chain of momentum transfer of body segments in the baseball pitching motion. J Chinese Inst Eng 2003;26(6):861-868.
15. Seroyer ST, Nho SJ, Bach BR, et al. The kinetic chain in overhand pitching: its potential role for performance enhancement and injury prevention. Sports Health 2010;2(2):135-146.
16. Crotin RL, Kozlowski K, Horvath P, Ramsey DK. Altered stride length in response to increasing exertion among baseball pitchers. Med Sci Sports Exerc 2014;46(3):565-571.
17. Dun S, Fleisig GS, Loftice J, et al. The relationship between age and baseball pitching kinematics in professional baseball pitchers. J Biomech 2007;40(2):265-270.
18. Escamilla R, Fleisig G, Barrentine S, et al. Kinematic and kinetic comparisons between American and Korean professional baseball pitchers. Sports Biomech 2002;1(2):213-228.
19. Escamilla RF, Barrentine SW, Fleisig GS, et al. Pitching biomechanics as a pitcher approaches muscular fatigue during a simulated baseball game. Am J Sports Med 2007;35(1):23-33.
20. Escamilla RF, Fleisig GS, Barrentine SW, et al. Kinematic comparisons of throwing different types of baseball pitches. J Appl Biomech 1998;14:1.
21. Fleisig GS, Barrentine SW, Zheng N, et al. Kinematic and kinetic comparison of baseball pitching among various levels of development. J Biomech 1999;32(12):1371-1375.
22. Stodden DF, Langendorfer SJ, Fleisig GS, Andrews JR. Kinematic constraints associated with the acquisition of overarm throwing Part I: Step and trunk actions. Res Q Exerc Sport 2006;77(4):417-427.
23. Elliott B, Grove JR, Gibson B, Thurston B. A three-dimensional cinematographic analysis of the fastball and curveball pitches in baseball. Int J Sport Biomech 1986;2(1):20-28.
24. Dun S, Loftice J, Fleisig G, et al. A biomechanical comparison of youth baseball pitches: is the curveball potentially harmful? Am J Sports Med 2008;36(4):686-692.
25. Fleisig GS, Kingsley DS, Loftice JW, et al. Kinetic comparison among the fastball, curveball, change-up, and slider in collegiate baseball pitchers. Am J Sports Med 2006;34(3):423-430.
26. Gandhi J, ElAttrache NS, Kaufman KR, Hurd WJ. Voluntary activation deficits of the infraspinatus present as a consequence of pitching-induced fatigue. J Shoulder Elbow Surg 2011;21(5):625-630.
27. Murray TA, Cook TD, Werner SL, et al. The effects of extended play on professional baseball pitchers. Am J Sports Med 2001;29(2):137-142.
28. Dillman CJ, Fleisig GS, Andrews JR. Biomechanics of pitching with emphasis upon shoulder kinematics. J Orthop Sports Phys Ther 1993;18(2):402-408.
29. Crotin RL. A kinematic and kinetic comparison of baseball pitching mechanics influenced by stride length. [dissertataion] Buffalo: State University of New York at Buffalo; 2013.
30. Aguinaldo AL, Chambers H. Correlation of throwing mechanics with elbow valgus load in adult baseball pitchers. Am J Sports Med 2009;37(10):2043-2048.
31. Aguinaldo AL, Buttermore J, Chambers H. Effects of upper trunk rotation on shoulder joint torque among baseball pitchers of various levels. J Appl Biomech 2007;23(1):42-51.
32. Matsuo T, Fleisig GS. Influence of shoulder abduction and lateral trunk tilt on peak elbow varus torque for college baseball pitchers during simulated pitching. J Appl Biomech 2006;22(2):93-102.
33. Elliot B, Grove JR, Gibson B. Timing of the lower limb drive and throwing limb movement in baseball pitching. Int J Sports Biomech 1988;4(1):59-67.
34. Matsuo T, Escamilla RF, Fleisig GS, et al. Comparison of kinematic and temporal parameters between different pitch velocity groups. J Appl Biomech 2001;17(1):1-13.
35. Stodden DF, Fleisig GS, McLean SP, Andrews JR. Relationship of biomechanical factors to baseball pitching velocity: within pitcher variation. J Appl Biomech 2005;21(1):44-56.
36. Urbin M, Fleisig GS, Abebe A, Andrews JR. Associations between timing in the baseball pitch and shoulder kinetics, elbow kinetics, and ball speed. Am J Sports Med 2013;41(2):336-342.
37. Marshall R, Elliott B. Long-axis rotation: the missing link in proximal-to-distal segmental sequencing. J Sports Sci 2000;18(4):247-254.
38. Wight J, Richards J, Hall S. Influence of pelvis rotation styles on baseball pitching mechanics. Sports Biomech 2004;3(1):67-83.
39. Mullaney MJ, McHugh MP, Donofrio TM, Nicholas SJ. Upper and lower extremity muscle fatigue after a baseball pitching performance. Am J Sports Med 2005;33(1):108-113.
40. Olsen SJ 2nd, Fleisig GS, Dun S, et al. Risk factors for shoulder and elbow injuries in adolescent baseball pitchers. Am J Sports Med 2006;34(6):905-912.
41. Reid M, Elliott B, Alderson J. Lower-limb coordination and shoulder joint mechanics in the tennis serve. Med Sci Sports Exerc 2008;40(2):308-315.
42. Wang LH, Lin HT, Lo KC, et al. Comparison of segmental linear and angular momentum transfers in two-handed backhand stroke stances for different skill level tennis players. J Sci Med Sport 2010;13(4):452-459.






Trackbacks/Pingbacks