

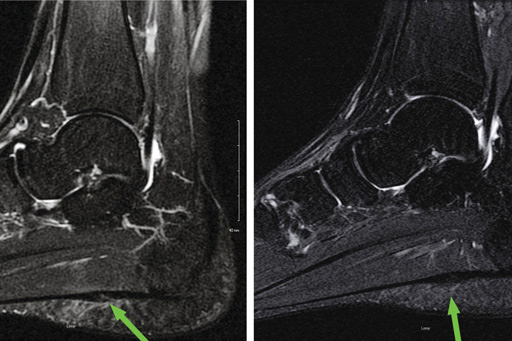
Magnetic resonance images depict a partial tear of the plantar fascia before (left) and after (right) treatment with PRP. (Images courtesy of John J. Wilson, MD, MS.)
By Emily Delzell
Two studies published early this year found platelet-rich plasma (PRP) injection improved pain and function in patients with chronic severe plantar fasciitis who hadn’t responded to conservative treatments.
“This is a group of unhappy patients with disabling levels of pain that’s not doing well with conventional treatment and who otherwise might be facing some type of surgical solution,” said Rocco Monto, MD, author of a randomized controlled trial epublished in January by Foot & Ankle International comparing PRP injection with corticosteroid injection (CSI).
PRP is theorized to promote healing through delivery of a concentrated cocktail of cytokines and growth factors, but there is little consistent evidence supporting its use in patients with tendon and ligament pathologies. (See “Platelet-rich plasma: An option for tendinopathy,” October 2013.)
Monto, an orthopedic surgeon in private practice in Nantucket, MA, randomized 40 patients (23 women) with heel pain for at least four months despite receiving standard nonoperative treatment to receive a single injection of either 3 cc of PRP or 40 mg methylprednisolone at the injury site. For two weeks after injection patients used a cam walker brace, engaged in physical activity as tolerated, and followed a home eccentric exercise and calf- and arch-stretching regimen.
Monto measured patients’ heel pain and function with American Orthopaedic Foot and Ankle Society (AOFAS) hindfoot scoring at baseline and three, six, 12, and 24 months after injection.
As Monto noted, participants’ baseline AOFAS score were low, averaging 52 (out of 100) in the CSI group and 37 in the PRP group. Both groups showed early improvements, with scores in the CSI and PRP groups rising at three months to 81 and 95, respectively. Scores declined for the CSI group thereafter, falling to 74 at six months and dropping to near baseline by 12 and 24 months.
The PRP group had a more durable response, with scores of 95, 94, 94, and 92 at three, six, 12, and 24 months, respectively.
The durability of PRP injection—and its lack with CSI—surprised Monto, who noted he’s largely abandoned steroid injection as a first-line treatment for the 10% to 15% patients with chronic plantar fasciitis who don’t respond to conventional therapy.

“It’s not a ‘platelet-rich panacea,’ but for this group of patients it’s part of multimodal approach that includes exercise and taking care with activities that returns them from a poor level of function to a fairly high level of activity,” he said.
A second study, a prospective series of 24 consecutive cases of plantar fasciopathy (22 patients, 13 women) treated at University of Wisconsin (UW) sports medicine clinics, also reported efficacy with PRP injection. The study authors noted that they prefer the term “plantar fasciopathy” to plantar fasciitis as the former better describes the degenerative pathology of the condition.
Participants had plantar fasciopathy of at least three months duration and hadn’t responded to three months or more of physician-recommended conservative therapy, including physical therapy, bracing, and orthotic use.
Investigators treated patients with a single injection of approximately 3 ml of PRP and compared results of the Foot and Ankle Ability Measure (FAAM), Foot–Single Assessment Numeric Evaluation (Foot-SANE), and several other measures of patient-reported pain, function, and satisfaction at baseline and 32 weeks postinjection.
Clinicians immobilized the injected foot in a boot for one week and encouraged patients to resume their previous physical therapy regimens within two weeks of the procedure.
At 32 weeks, patients showed statistically significant and clinically meaningful improvement on all measures, including the primary outcomes, FAAM subscores for activities of daily living and sports-related function, which improved 32% and 82%, respectively. Patients also reported significant improvements in Foot-SANE scores, which are generated by asking them to rate their foot as a percentage of normal, with 100% being normal. Mean Foot-SANE scores improved an average of 37.2%, from 49.30 ± 19.38 at baseline to 67.66 ± 25.10 at 32 weeks.
“For patients with chronic, difficult-to-treat plantar fasciitis, PRP effectively reduced pain and symptoms without surgery, so it’s a viable alternative in that group,” said John J. Wilson, MD, MS, assistant professor of orthopedics and family medicine at UW-Madison and lead author of the study, which was published in February in Foot & Ankle Specialist.
“We didn’t analyze subjects in terms of imaging morphology of the ligament, so we don’t know if the clinical improvement we saw will also translate into improvements in the tissue, but, in theory, that’s one of the benefits of PRP,” he said.
He also noted PRP injection avoids potential harms of CSI, which can weaken tissue and has been associated with an elevated risk of tendon and ligament rupture (see “Evidence on corticosteroid injection could change the way you practice,” April 2011, page 13).
Like Monto, Wilson is trending away from steroid injection for chronic plantar fasciopathy, though he said many insurers don’t yet cover PRP injection, and out-of-pocket costs can be as high as $1000.
“When patients have to choose between [a procedure covered by insurance] and one they have to pay for, they often opt for the one that costs less,” he said.
Wilson and colleagues are building on data from this case series with a randomized controlled trial comparing CSI and PRP injection. The investigators are preparing the final data and imaging analyses prior to publication later this year, but Wilson presented preliminary
results at the 2013 annual meeting of the American Medical Society for Sports Medicine.
The 37 participants (27 women) had experienced plantar fasciopathy symptoms for more than six months and had not responded to at least two conservative treatments. Patients were not blinded to their injection type and those in the CSI group had the option to cross over to plasma injection if their pain returned to baseline at eight or 16 weeks. Six patients in the CSI group ultimately crossed over to PRP injection.
Using intention-to-treat analyses, investigators found that both cohorts had clinically and statistically significant improvements in pain and function—but no statistically significant differences between interventions—at 32 weeks.
“Thirty-two weeks may not long enough to realize the full benefits of PRP-generated tissue healing,” Wilson said. “Some literature shows maximal benefits weren’t realized for a year or more.”
Sources:
Monto RR. Platelet-rich plasma efficacy versus corticosteroid injection treatment for chronic severe plantar fasciitis. Foot Ankle Int 2014 Jan 13. [Epub ahead of print]
Wilson JJ, Lee KS, Miller AT, Wang S. Platelet-rich plasma for the treatment of chronic plantar fasciopathy in adults: A case series. Foot Ankle Spec 2014;7(1): 61-67.
Wilson JJ. Platelet-rich plasma for chronic plantar fasciopathy in adults: A randomized controlled trial. Presented at the 22nd Annual Meeting of the American College of Sports Medicine, San Diego, CA, April 2013.





