


By Tom Michaud, DC
Dr. Michaud is in chiropractic practice in Newton, Massachusetts, and is the author of Human Locomotion: The Conservative Management of Gait-Related Disorders. He discloses that he is the owner of www.humanlocomotion.org, where the Toe Strength Dynamometer discussed in this article is sold.
LER: It seems to be a pervasive belief among recreational athletes that improving flexibility lessens the risk of injury. Does stretching have a considerable impact on the injury rate?
TM: When nearly 100 experienced recreational runners were recently asked to name the most common cause of running-related injuries, the vast majority cited “failure to stretch regularly.”1 The authors of this study were concerned because runners seemed to be unaware of the overwhelming body of research showing that stretching does not alter the injury rate.2,3
To make matters worse, the belief that stretching protects you from injury is becoming more prevalent.4
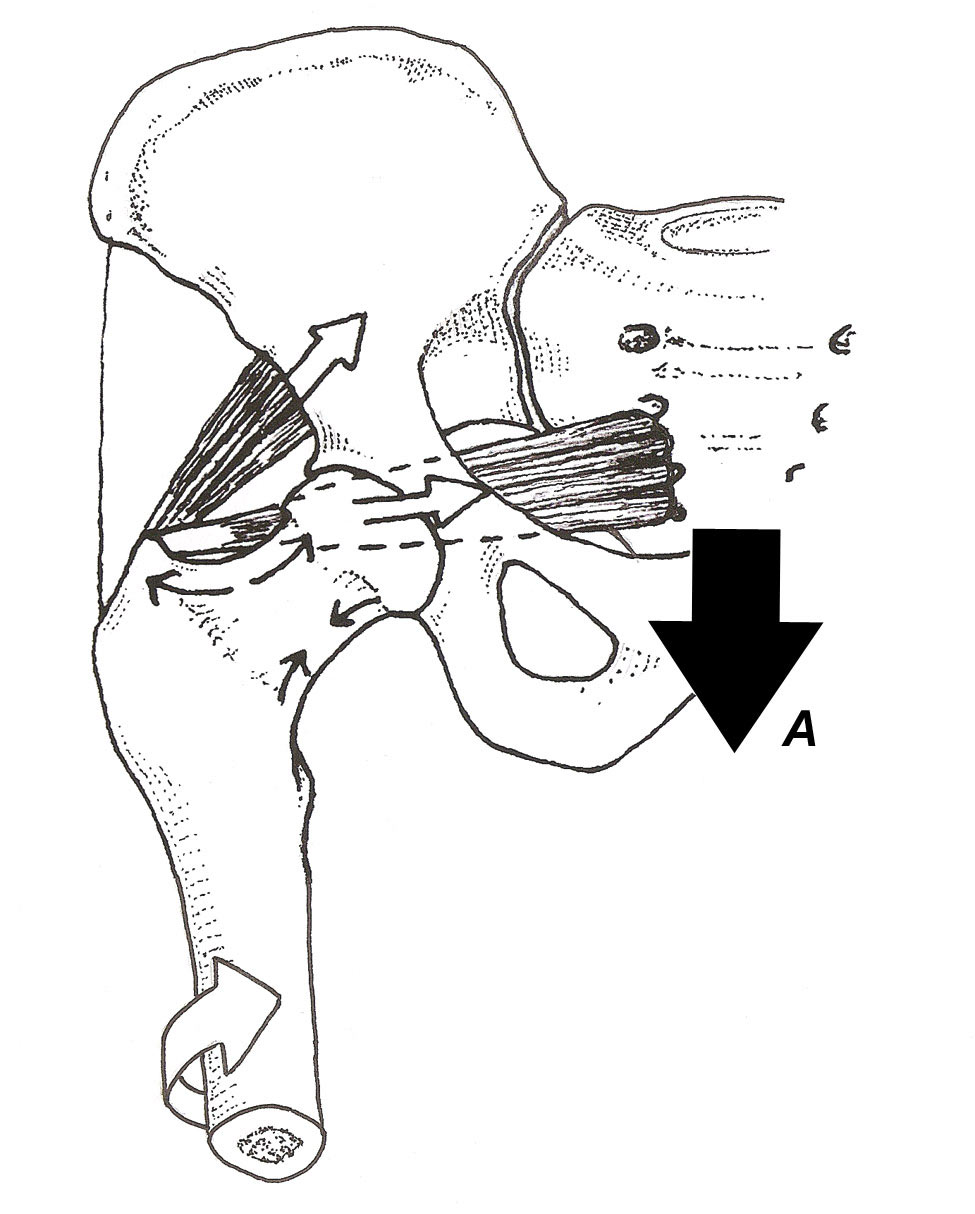
Figure 1. The piriformis and gluteus medius muscles create a powerful compressive force that prevents the femoral neck (A) from fracturing.
That is not to say that stretching should be avoided: Pereles and colleagues proved that runners intuitively know whether or not they should stretch.5 The researchers randomly assigned 2,729 recreational runners to a stretching or nonstretching pre-run routine. Not surprisingly, no significant difference was detected in the injury rate between runners who stretched and runners who did not (this reflects what has been noted in all studies on stretching). If a runner who routinely stretched was assigned to the nonstretching protocol, however, he (she) was nearly twice as likely to sustain a running injury.
Because the number of participants is high, this single study proves that, if you have a patient who finds stretching beneficial, you should encourage that patient to stretch regularly. Stretching the gastrocnemius muscle is particularly important; DiGiovanni et al6 proved conclusively that a tight gastrocnemius muscle correlates with a variety of forefoot and midfoot injuries, including metatarsal stress fracture, plantar fasciitis, and posterior tibial tendon insufficiency.
LER: You’re on record advocating strength training as a preventive to lower-extremity injury. What’s the evidence for your enthusiasm?

TM: Compared to stretching, strength training remains, in my opinion, the most underutilized treatment intervention for treating and preventing a range of lower-extremity injuries. In 2004, Burne and co-workers7 determined that a 10-mm reduction in calf circumference resulted in a 4-fold increase in the incidence of tibial stress fracture. This finding is consistent with research demonstrating that lower-extremity muscles prevent tibial fracture by adjusting to bony vibrations by pre-tensing prior to contacting the ground.8,9
In addition to dampening potentially dangerous bony oscillations following heel strike, certain muscles play a key role in creating compressive forces that allow various bones to resist bending strains present during the gait cycle. For example, the piriformis muscle, often considered to be unimportant during the gait cycle, has been shown to create long-axis compression of the femoral neck that prevents it from bending with the application of vertical forces (Figure 1). Without adequate support from the piriformis and the synergistic lower gluteus medius, a bending force would be created in the femoral neck capable of producing fracture (tension fracture on the superior side or compressive fracture on the inferior side).
Khayambashi and colleagues10 recently proved that a simple strength measurement performed with a handheld dynamometer predicted anterior cruciate ligament injury in college athletes. The authors evaluated hip rotator and abductor strength at the start of the season in more than 500 athletes participating in a range of sports. Athletes who were unable to generate 20% of their body weight with their hip rotators, and 35% of their body weight with their hip abductors, were significantly more likely to have a noncontact anterior cruciate ligament injury. This test takes fewer than 20 seconds to perform and should be a part of every preseason strength evaluation.
LER: What strategies do you recommend in addition to maintaining hip rotator and abductor strength?
TM: It’s also important to keep feet and ankles strong. To evaluate the role that the toe flexors might play in preventing injury, Ferris and colleagues11 embedded strain gauges in the metatarsal shafts of cadaveric feet and evaluated bending forces present during simulated propulsion as the long digital flexor muscles were either tractioned or relaxed with pneumatic actuators (Figure 2). Using this elaborate technique, these researchers determined that, when the digital flexor muscles were relaxed, significant bending strains were present in the metatarsal shafts—which, in real-life, would have created bending force capable of fracturing bone. When the muscles were tractioned, they created a powerful compressive force along the plantar metatarsal shafts that greatly reduced bending strains. The authors speculated that strengthening the digital flexors “may play a role in the prevention of metatarsal stress fractures.”

Figure 2. Cadaveric model evaluating plantar pressures and metatarsal bending strains present during heel lift. Activation of the digital flexors markedly reduces pressure beneath the central forefoot and prevents buckling of the metatarsal shafts. Redrawn from Ferris et al.11
Weak toe flexors have also been correlated with chronic plantar fasciitis. McClinton and co-workers12 recently demonstrated that patients with chronic heel pain are more likely to present with weak intrinsic foot muscles. Additionally, people with the weakest intrinsic muscles are also more likely to be long-term orthosis users. This is not to say the orthoses cause intrinsic foot weakness, as it is likely that people with weak intrinsic muscles respond more favorably to orthotic intervention and are therefore more likely to use orthoses to manage heel pain. Nonetheless, this paper emphasizes the importance of measuring toe strength in patients presenting with chronic heel pain.
LER: What protocol do you use to gauge toe strength?
TM: I use a Toe Strength Dynamometer, a simple modification of the popular paper grip test (Figure 3). The resulting strength score allows practitioner and patient to see clear asymmetries in strength, thus providing objective goals for rehabilitation. Maintaining toe strength is especially important because weak toes have been correlated not just with chronic heel pain but also with falls in the elderly13 and impaired athletic performance.14
LER: One downside to strength training is the high injury rate associated with lifting heavy weights. How do you deal with this obstacle?
TM: According to guidelines issued by the American College of Sports Medicine, the only effective way to build muscle is to perform multiple sets of 8 to 12 repetitions while lifting heavy weights (nearly 90% full effort).15 The theory is that, to stimulate muscle repair, you have to push the muscle to the limit of its capacity.
Fortunately, recent research proves that these guidelines are wrong: It is possible to build muscle mass using light resistance provided by body weight alone.16 In that 2018 study in Japan, 88 men and women (all 70 years and older) participated in a weight-training program in which they performed 2 sets of 10 to 14 repetitions daily for 12 weeks. The subjects used body weight alone and performed movements slowly (4 seconds up, 4 seconds down). At the end of the 12-week training program, in addition to a significant increase in muscle mass, participants had decreased hip and waist circumference and less abdominal fat.
The authors claim that their success was related to the total time that muscles were contracting during the protocol. Although loads were light, the 4-second-up and 4-second-down times resulted in a total of 1,344 seconds of muscle contraction time a week (i.e., 12 repetitions × 8 seconds × 2 sets × 7 times a week). The authors suggest the long total contraction time is what creates muscle mass—not the amount of resistance.
Other nice features of this study are that the seniors involved had no experience with weight training; the exercises were performed at home (taking fewer than 15 minutes each day); and, at the end of the study, only 2 of 88 subjects had dropped out. High compliance and great outcomes associated with this study should make the use of light weight with high repetitions a consideration for almost every exercise prescription.
- Saragiotto BT, Yamato TP, Lopes AD. What do recreational runners think about risk factors for running injuries? A descriptive study of their beliefs and opinions. J Orthop Sports Phys Ther. 2014;44:733-738.
- Saragiotto BT, Yamato TP, Hespanhol Junior LC, Rainbow MJ, Davis IS, Lopes AD. What are the main risk factors for running-related injuries? Sports Med. 2014;44:1153-1163.
- van Gent RN, Siem D, van Middelkoop M, van Os AG, Bierma-Zeinstra SM, Koes BW. Incidence and determinants of lower extremity running injuries in long distance runners: a systematic review. Br J Sports Med. 2007;41:469-480.
- Herbert RD, de Noronha M. Stretching to pre-vent or reduce muscle soreness after exercise. Cochrane Database Syst Rev. 2007;CD004577. www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD004577.pub2/full. Accessed August 11, 2018.
- Pereles D, Roth A, Thompson D, Darby JS, Tho mpson MS. A large, randomized, prospective study of the impact of a pre-run stretch on the risk of in-jury in teenage and older runners. (Report) Indianapolis, IN: USA Track & Field; 2007. http://www.usatf.org/stretchStudy/StretchStudyReport.pdf. Accessed August 11, 2018.
- DiGiovanni CW, Kuo R, Tejwani N, Price R, Hansen ST Jr, Cziernecki J, Sangeorzan BJ. Isolated gastrocnemius tightness. J Bone Joint Surg Am. 2002;84-A:962-970.
- Burne SG, Khan KM, Boudville PB, et al. Risk factors associated with exertional medial tibial pain: a 12 month prospective clinical study. Br J Sports Med. 2004;38:441-445.
- 8. Wakeling JM, Nigg BM. Modification of soft tissue vibrations in the leg by muscular activity. J Appl Physiol (1985). 2001;90:412-420.
- Wakeling JM, Liphardt AM, Nigg BM. Muscle activity reduces soft-tissue resonance at heel-strike during walking. J Biomech. 2003;36:1761-1769.
- Khayambashi K, Ghoddosi N, Straub RK, Powers CM. Hip muscle strength predicts noncontact anterior cruciate ligament injury in male and female athletes: a prospective study. Am J Sports Med. 2016;44:355-361.
- Ferris L, Sharkey NA, Smith TS, Matthews DK. Influence of extrinsic plantar flexors on forefoot loading during heel rise. Foot Ankle Int. 1995;16:464-473.
- McClinton S, Collazo C, Vincent E, Vardaxis V. Impaired foot plantar flexor muscle performance in individuals with plantar heel pain and association with foot orthosis use. J Orthop Sports Phys Ther. 2016;46:681-688.
- Mickle KJ, Caputi P, Potter J, Steele JR. Efficacy of a progressive resistance exercise program to increase toe flexor strength in older people. Clin Biomech (Bristol, Avon). 2016;40:14-19.
- Kokkonen J, Bangerter B, Roundy E, Nelson A. Improved performance though digit strength gains. Res Q Exerc Sport. 1988;59:57-63.
- American College of Sports Medicine. ACSM’S Guidelines for Exercise Testing and Prescription. Philadelphia, PA: Lippincott Williams & Wilkins; 2006.
- Tsuzuku S, Kajioka T, Sakakibara H, Shimaoka K. Slow movement resistance training using body weight improves muscle mass in the elderly: A randomized controlled trial. Scand J Med Sci Sports. 2018;28:1339-1344.
- Endo M, Ashton-Miller JA, Alexander NB. Effects of age and gender on toe flexor muscle strength. J Gerontol A Biol Sci Med Sci. 2002;57:M392-M397.
- Menz HB, Zammit GV, Munteanu SE, Scott G. Plantarflexion strength of the toes: age and gender differences and evaluation of a clinical screening test. Foot Ankle Int. 2006;27:1103-1108.
- Mickle KJ, Angin S, Crofts G, Nester CJ. Effects of age on strength and morphology of toe flexor muscles. J Orthop Sports Phys Ther. 2016;46:1065-1070.
- Mickle KJ, Munro BJ, Lord SR, Menz HB, Steele JR. ISB Clinical Biomechanics Award 2009: toe weakness and deformity increase the risk of falls in older people. Clin Biomech (Bristol, Avon). 2009;24:787-791.
- Mickle KJ, Nester CJ. Morphology of the toe flexor muscles in older adults with toe deformities. Arthritis Care Res (Hoboken). 2018;70:902-907.
- Jung DY, Koh EK, Kwon OY. Effect of foot orthoses and short-foot exercise on the cross-sectional area of the abductor hallucis muscle in subjects with pes planus: A randomized controlled trial. J Back Musculoskelet Rehabil. 2011;24:225-231.
- Kelikian H. Hallux Valgus, Allied Deformities of the Forefoot and Metatarsalgia. Philadelphia, PA: W.B. Saunders Company; 1965.
- England MD. The problem of hallux valgus. Chiropodist. 1954;9:275.
- Kato T, Watanabe S. The etiology of hallux valgus in Japan. Clin Orthop Related Res. 1981;157:78-81.
- Radford JA, Landorf KB, Buchbinder R, Cook C. Effectiveness of calf muscle stretching for the short-term treatment of plantar heel pain: a randomised trial. BMC Musculoskelet Disord. 2007;8:36.
- Sullivan J, Burns J, Adams R, Pappas E, Crosbie J. Musculoskeletal and activity-related factors associated with plantar heel pain. Foot Ankle Int. 2015;36:37-45.
- Rasenberg N, Riel H, Rathleff MS, Bierma-Zeinstra SM, van Middelkoop M. Efficacy of foot orthoses for the treatment of plantar heel pain: a systematic review and meta-analysis. Br J Sports Med. 2018;52:1040-1046.
- Allen RH, Gross MT. Toe flexors strength and passive extension range of motion of the first metatarsophalangeal joint in individuals with plantar fasciitis. J Orthop Sports Phys Ther. 2003;33:468-478.
- Chang R, Kent-Braun JA, and Hamill J. Use of MRI for volume estimation of tibialis posterior and plantar intrinsic foot muscles in healthy and chronic plantar fasciitis limbs. Clin Biomech (Bristol, Avon). 2012;27:500-505.
- Cheung RT, Sze LK, Mok NW, Ng GY. Intrinsic foot muscle volume in experienced runners with and without chronic plantar fasciitis. J Science Med Sport. 2016;19:713-715.
- Mølgaard CM, Rathleff MS, Andreasen J, et al. Foot exercises and foot orthoses are more effective than knee focused exercises in individuals with patellofemoral pain. J Science Med Sport. 2018;21:10-15.
- Bennell K, Wee E, Coburn S, et al. Efficacy of standardised manual therapy and home exercise programme for chronic rotator cuff disease: randomised placebo controlled trial. BMJ. 2010;340:c2756.
- Helmhout PH, Witjes M, Nijhuis-Van Der Sanden RW, Bron C, van Aalst M, Staal JB. The effects of lumbar extensor strength on disability and mobility in patients with persistent low back pain. J Sports Med Phys Fitness. 2017;57:411-417.





