

Shutterstock.com 274158386
The latest paper to challenge biomechanics-based foot orthotic management concepts developed decades ago has revitalized a long-running discussion among foot specialists about how to define normal structure and function and which assessments should be used in prescribing foot orthoses.
By Cary Groner
A recent paper in the Journal of Foot and Ankle Research (JFAR) added fuel to a long-burning controversy over how to assess what’s normal and abnormal in the structure and function of the foot, and how—if at all—those assessments should be used to guide orthotic management.1
Researchers at the University of Salford in the UK evaluated the left foot of 100 asymptomatic individuals using the static biomechanical approach promulgated in the 1970s by Merton Root, DPM,2 then compared those findings with foot motion during gait. They found that none of the “deformities” (abnormal alignment or range of motion) suggested by the Root method correlated with altered foot kinematics, which poses an obvious conundrum for clinicians who base treatment on an assessment using a subtalar joint neutral foot position.
Other experts have reached similar conclusions. For example, Australian researchers reported in 2015 that clinical measures of foot posture explained only a small amount of the variation observed in foot kinematics.3
Andrew Buldt, PhD, a postdoctoral researcher in foot biomechanics at La Trobe University in Melbourne and that paper’s first author, told LER “there was a small relationship, but not enough to make clinical decisions.”
The researchers behind the new paper went further, however, proposing that the Root assessment model was no longer valid for clinical practice, that clinicians should stop using subtalar neutral and other nonweightbearing alignments and movements to define foot “deformities,” and that the method was likely irrelevant for prescribing foot orthoses.
“We measured foot kinematics in what we think is the most accurate way possible,” said lead author Hannah Jarvis, PhD, a postdoctoral researcher at Manchester Metropolitan University in the UK and a fellow at Salford, where she wrote a dissertation that laid the groundwork for the JFAR article. “We attached marker plates to the foot, and were able to capture individual bone movement and compare that to the Root static assessments. Root suggested that the subtalar joint was the key joint in the foot, but our results indicate that all the joints are equally important in their contribution to foot movement.”

Blowback
Responses to the article came from some august quarters, and they were not universally supportive. Tom McPoil, PT, PhD, a professor in the School of Physical Therapy at Regis University in Denver—and one of the original critics of the Root approach—said he pointed out in his peer review that a study using 100 healthy left feet, regardless of quality, was unlikely to provide compelling evidence of issues with the Root model.
Moreover, in response to the paper’s assertion that its results “question the relevance of the Root assessments in the prescription of foot orthoses,” he noted that because the authors didn’t assess the effect of orthoses on foot kinematics, the statement was purely speculative.
McPoil also offered supportive comments, however, calling the manuscript an important addition to the evidence accumulated over the previous 20 years regarding controversies associated with the Root approach.
Some of the evidence McPoil referred to was his own. As early as 1994, he was the first author of a study that reported a disconnect between rearfoot angle in a subtalar neutral position and the actual pattern of rearfoot motion during walking.4

Figure 1. Jarvis et al analyzed the feet of 100 symptom-free participants and found that all were associated with at least two deformities according to a Root-based assessment. (Reprinted with permission from reference 1.)
The next year he was the first author of a paper that acknowledged Root’s contribution to redefining the clinical view of the foot from a static to a dynamic structure, but that also pointed out some of the approach’s conceptual and practical limitations.5 For example, the paper noted that Root’s findings were difficult to reproduce, and that use of the subtalar neutral position to define a “normal” foot created a classification system in which almost everyone’s feet were to some degree abnormal. Moreover, McPoil and his colleagues pointed out that Root’s description of subtalar neutral was based on one first proposed in 1964 by Wright et al,6 but noted that Wright used the term very differently—and in a way that not only agreed closely with McPoil’s findings but also varied significantly from Root’s.
Perhaps most pertinent to the Jarvis paper, in that prescient 1995 article McPoil wrote: “Investigations7,8 … have demonstrated the inability to predict dynamic motion of the rearfoot during walking when using the static foot evaluation procedures as described by Root et al.”5 The 1995 paper went on to propose a “tissue stress model” as a basis for diagnosing and treating foot disorders, which has had a powerful influence on clinical thinking ever since.
The Root of the matter
Contemporaries of McPoil had suggested the basics of the tissue stress model even earlier. Kevin Kirby, DPM, an adjunct associate professor at the California School of Podiatric Medicine at Samuel Merritt College in Oakland, who also maintains a private practice in Sacramento, published his first objections to the Root model in 1990, including a pointed screed titled, “Inaccuracies in podiatric biomechanics dogma.”9
This detailed examination of the Root approach stated nine specific problems—for example, “Inaccuracy #1: The calcaneus must be in the vertical position while in relaxed calcaneal stance position in order for the foot to function normally during gait”—each of which was followed by a terse rebuttal. It was a bit reminiscent of Martin Luther nailing his 95 theses to the church door, and it was received, at first, with similar consternation. It’s important to bear in mind, however, that Kirby was a student of Root’s, knew him personally, and admired his work.
“When he wrote those books—the classic is The Normal and Abnormal Function of the Foot, volume 2,2—he figured that within ten or twenty years all that information would need to be updated,” Kirby said. “He was visionary, the first to start a biomechanics program in any podiatry school in the world, and he started the biomechanics fellowship I completed. His biggest problem was that, instead of saying his model of the foot was a structural ideal, he said it was normal, which has a very different connotation. He also said that there can be many variations from normal with which the foot will still function well, but too much deviation can cause problems.”
In the original text,2 Root wrote, “As noted by the definitions, these neutral positions are purely reference points. They are significant, however, in that they make it possible to measure and define positional and structural variances.”
This doesn’t sound much like pulpit-pounding dogma, which reinforces Kirby’s point about Root’s intentions—even if Kirby was the one to call the results of Root’s proposals “dogma” in the first place.
And Root, to his credit, seemed to anticipate the tissue stress model when he wrote, “ … it becomes obvious that the deformity has its origin in soft tissue tension whenever a triplane position of deformity is observed within the foot.”2 In the next paragraph, however, he added that when the “deformity” is uniplanar, it is caused by an abnormally shaped bone—just the sort of statement that’s led to contention ever since.
Kirby believes Root would have strengthened his legacy if he’d deemphasized rearfoot position and paid more attention to the talar head and neck region.
“The position of the head and neck of the talus relative to the plantar aspect of the foot really determines the subtalar joint axis location,” he said. “Mert didn’t really get into that, and we now know from studies by McPoil and Jarvis that the rearfoot angle doesn’t strongly correlate with function or pathology.”
Such considerations don’t remain in the lofty realm of academic publications, of course, and Kirby explained how they can affect clinical practice.
“I became aware of the problem early on,” he said. “You’d have someone come in with differently shaped feet—a flatter foot on one side which was associated with symptoms—say, posterior tibial tendinitis. The other side, which did not have as flat a foot, didn’t have those symptoms. So, you’d go through the Root measurements and the heels [inversion/eversion] would come out within a degree or two of each other, which is within reasonable measurement error; that meant the measurements weren’t giving you any idea why that person was developing tendinitis on one side. They didn’t take into account the position of the talar head and neck, and didn’t correlate with gait function—with either the kinematics or the pathology I was seeing. When that happens, you’d better develop a better theory.”
Filial duties
Jeff Root, Merton’s son, has found himself in the odd position of defending his father’s legacy while acknowledging that its foundations may require some adjusting given the eroding tides of new data. Although he is not a podiatrist, Jeff Root now owns the Root Laboratory, an orthotic fabrication company in Meadow Vista, CA, and keeps abreast of the issues for obvious reasons.
“When Root was a student, they really didn’t know what caused foot pathologies, which made them very difficult to treat,” he said. “He came up with the concept of subtalar neutral position—where the foot is neither supinated nor pronated—because we needed to establish a convention whereby we could communicate about location and structure. But the foot only passes through subtalar neutral, as it does through many other points, and he was very clear about that; he wanted to promote healthy motion that was not pathological.” Jeff Root also pointed out that podiatry is about more than prescribing orthoses.
“When podiatrists consider surgeries like an Achilles tendon lengthening, they need to assess the range of ankle dorsiflexion and determine whether the surgery is warranted,” he explained.
Clinicians benefit from a common terminology about the structure of the foot in such situations, in other words, even if those terms don’t necessarily relate to kinematics.
“My problem with the Jarvis paper is that they’re telling us what we shouldn’t do, not what we should do,” he added.
And, though Jeff Root sees the potential for tissue stress theory to change the field, he wrestles with aspects of it.
“We need a model that’s teachable, that’s reproducible,” he said. “Tissue stress theory is great, but in my opinion, it’s not yet a consistent model. If the goal is to make this a more scientific process, how do you make it more clinically practical? I think that’s where we’re struggling.”
Tissue stress
Kevin Kirby agreed, to a point.
“One problem is that a lot of studies attempt to classify how the foot works, but they don’t really classify pathologies,” he said. “They’re conducted in people without symptoms, and we don’t treat people without symptoms. Hannah Jarvis looked at kinematics, but it’s kinetics—the forces and moments acting on the foot—that cause injuries. Structural deformities might not affect kinematics but could cause changes in kinetics.”
As it happens, however, Jarvis and colleagues did collect kinetic data—they just haven’t been published yet.
“We’re putting together a series of papers following from those data,” she told LER. “We have force-plate data on ground reaction forces to calculate moments. We also have EMG [muscle activation] and plantar pressure data of the foot and lower limb. Our project is to develop an idea about how all those factors and parameters interact with each other to cause foot movement, then hypothesize what is normal and compare that to other studies that have reported data on symptomatic feet. We’re still analyzing that, and we think you can’t just view the foot in one kinematic model; you have to take in lots of different factors, and be sure you’re viewing the foot as a multisegmental model.”
Jarvis herself is a fan of the tissue stress model, it turns out.
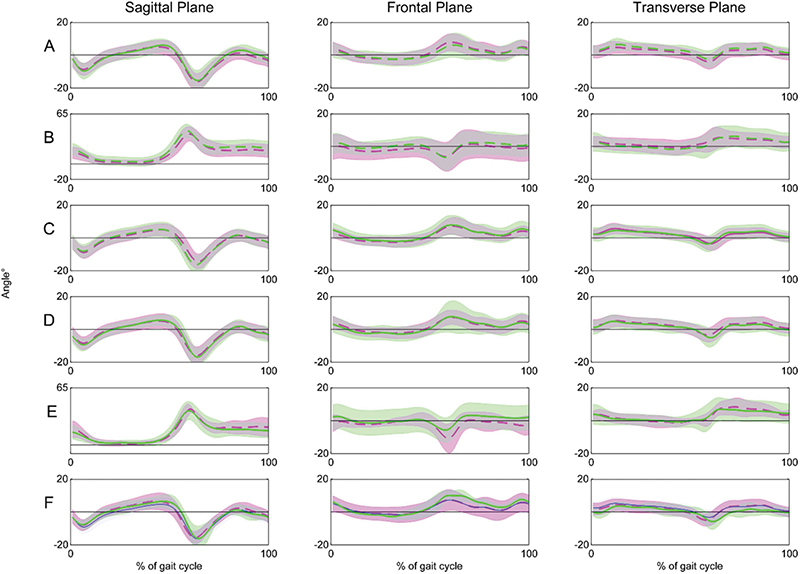
Figure 2. Jarvis et al found few differences in foot kinematics between feet classified with a deformity and those without a deformity. Graphs illustrate foot kinematics in feet with and without the rearfoot, ankle, first ray, forefoot, and hallux deformities that were investigated. Pink or blue refers to the deformity group in all cases; green = no deformity. A = rearfoot motion for ankle equinus vs no equinus deformity; B = hallux- medial forefoot motion for hallux deformity (<65° of dorsiflexion) vs no hallux deformity; C = rearfoot motion for hallux deformity (<65° of dorsiflexion) vs no hallux deformity; D = rearfoot motion for plantar flexed first ray deformity vs no first ray deformity; E = hallux-medial forefoot motion for plantar flexed first ray deformity vs no first ray deformity; F = rearfoot motion for forefoot varus/valgus deformity vs no forefoot deformity. (Reprinted with permission from reference 1.)
“I think it’s the way forward,” she said. “I’ve admired Tom McPoil’s work since I was an undergrad. I think the problem is that there isn’t a treatment rationale associated with it, at least on the orthotics front. With orthoses, you can reduce stresses on the tissues and relieve symptoms; the challenge lies in designing an orthosis based on measurements that relate to dynamic function.”
In the 1995 article that defined the tissue stress model,4 McPoil and coauthor Gary Hunt, PT, DPT, noted that the tissue’s elastic region represents “the normal give-and-take of soft tissues which prevents excessive joint movement as the foot is loaded and unloaded.” When overused, however, tissues can be deformed to the point of injury.
McPoil and Hunt proposed a four-step examination and management protocol:
(1) identifying the tissues being excessively stressed;
(2) applying controlled stresses to those tissues as well as palpation, range of motion, and muscle function/strength assessments;
(3) determining whether the patient’s complaint is secondary to excessive mechanical loading; and
(4) instituting a management protocol emphasizing reduced tissue stress through rest, footwear, and orthoses; healing of the tissues; and restoration of flexibility and muscle strength.
Kevin Kirby explained that tissue stresses may be due to compression loading (pressing together), tension loading (pulling apart), or shear loading (side-to-side movement), and that, ideally, an orthosis will help perform the function of the injured tissue during weightbearing activities.
“For example, the plantar fascia is a tension load-bearing structure that helps hold up the arch,” he said. “If it’s under too much tension, you have to make the orthotic duplicate that function. If you have posterior tibial tendinitis, you need the orthotic to help raise the arch; it creates an external force on the foot that duplicates the internal function of those structures. That reduces the load, decreases pain, speeds healing, and ideally lets the patient function better.”
Orthoses
One of the problems with discussing foot orthoses—as Jarvis mentioned and as LER has previously reported10—is that even though they are often effective for relief of symptoms, no one really knows the mechanisms involved.
“You can get many patients more comfortable by using something that has basically the same shape as the foot,” Kirby said. “You don’t need an exact fit to improve symptoms.”
As noted in that earlier LER article, the idea that orthoses actually correct structural alignment in the lower extremities has fallen into disfavor.11 Tissue stress theory—that the orthosis takes some of the strain off of the foot structure it mimics—is another plausible explanation.
Moreover, Benno Nigg, DrScNat, a professor emeritus of biomechanics at the University of Calgary in Canada, has suggested the central nervous system (CNS) may be the most important actor in the play of forces under examination. Nigg has proposed that impact forces during heel strike may constitute an input signal to which muscles respond with a “tuning strategy” that minimizes soft tissue vibration.12 This adaptation, in turn, supports a “preferred movement path”;13,14 orthoses that support that path would decrease muscle activity, but those that counteract it would increase that activity.
“Benno Nigg says that the CNS is going to control the motion of the foot regardless,” Kirby said. “I don’t think his theory is completely accurate, but I think it’s headed in the right direction. But, again, we don’t treat motion; we treat injuries caused by abnormal internal forces. So, should we quit doing all measurements? I think we need to do some—maybe not the Root measurements, but we should do the research to see if there is a correlation between ground reaction forces, foot deformities, and loading.”
There is, too, an inherent tension between the work of researchers—who need conditions to be as standardized as possible to draw conclusions about asymptomatic individuals—and the work of clinicians, who increasingly are managing symptomatic patients with treatments that are as individualized as possible, regardless of what the theories say.
“I see no value to subtalar neutral in terms of clinical decision-making,” Gross said. “To me, it’s a matter of what tissue has the pathology, why it has the pathology, and what’s driving the stress. Once you understand those things, what do you do about it? If a patient is having trouble because tissue is getting stressed too much, what’s driving that tensile stress?”
For Gross, it’s as much art as science; sometimes there’s simply no explanation for why people move the way they do.
“You can have two people with the exact same structure and static standing posture, who look similar but who move very differently,” he said. “Sometimes I can explain it by things I see when they’re on the table—say, soft-tissue extensibility—and sometimes I can’t explain it at all. I’ve gotten to the point that when I see people walking, I can see if they have forefoot varus; I’m looking for that instant when the forefoot makes initial contact with the ground, and I can see it happening just on the lateral aspect of the forefoot. But when they’re standing there with the foot rolled in, you don’t know what’s causing it.”
Moving ahead
According to Andrew Buldt of La Trobe University, an emerging consensus about structure and kinematics is likely to move the field forward with increasing speed.
“The biomechanical techniques we’re using in the lab are becoming a lot more sophisticated, and that has allowed us to challenge some of the paradigms we have used for a long time,” Buldt said. “The challenge is to adapt those in a way that’s usable in a clinical situation. The strength of the Root model was that it was something a clinician could understand and apply in the clinic. You didn’t need a sophisticated understanding of motion analysis, and in that sense, it’s been a good tool and should be acknowledged as such.”
Even as research continues to suggest foot function is more complex than once thought,3,15-17 the need to make such findings clinically relevant and useful is as vital as ever.
“The challenge for us is to use the kinematic and plantar pressure techniques we’ve developed to break down the foot into its constituent segments. We’re getting away from viewing the foot as one functional unit that’s controlled by what happens at the subtalar joint. We understand now that the foot has a number of interdependent functional units that have their own characteristics,” Buldt said. “So that’s our challenge: to come up with a model to understand the movements of those segments—what’s normal, what’s abnormal, and what leads to tissue stress and pathology.”
Cary Groner is a freelance writer in the San Francisco Bay Area.
- Jarvis HL, Nester CJ, Bowden PD, Jones RK. Challenging the foundations of the clinical model of foot function: further evidence that the Root model assessments failed to appropriately classify foot function. J Foot Ankle Res 2017;10:7.
- Root ML, Orien WP, Weed JH. Normal and Abnormal Function of the Foot. Vol 2. Los Angeles, CA: Clinical Biomechanics Corp; 1977.
- Buldt AK, Murley GS, Levinger P, et al. Are clinical measures of foot posture and mobility associated with foot kinematics when walking? J Foot Ankle Res 2015;8:63.
- McPoil T, Cornwall MW. Relationship between mutual subtalar joint position and pattern of rearfoot motion during walking. Foot Ankle Int 1994;15(3):141-145.
- McPoil T, Hunt G. Evaluation and management of foot and ankle disorders: present problems and future directions. J Orthop Sports Phys Ther 1995;21(6):381-388.
- Wright DG, Desai SM, Henderson WH. Action of the subtalar and ankle-joint complex during the stance phase of walking. J Bone Joint Surg Am 1964;46:361-382.
- Hamill J, Bates BT, Knutzen KM, Kirkpatrick GM. Relationship between selected static and dynamic lower extremity measures. Clin Biomech 1989;4(4):217-225.
- McPoil TC, Cornwall MW. The relationship between static measurements of the lower extremity and the pattern of rearfoot motion during walking. Phys Ther 1994;74:S141.
- Kirby K. Foot and lower extremity biomechanics: a ten year collection of Precision Intricast newsletters. Payson, AZ: Precision Intricast; 1990.
- Groner C. In search of a mechanism for foot orthoses’ effects. LER 2011;3(4):29-33.
- Kolata G. Close look at orthotics raises a welter of doubts. New York Times website. http://www.nytimes.com/2011/01/18/health/nutrition/18best.html. Published January 17, 2011. Accessed June 1, 2017.
- Nigg BM. The role of impact forces and foot pronation: a new paradigm. Clin J Sport Med 2001;11(1):2-9.
- Nigg BM, Vienneau J, Smith AC, et al. The preferred movement path paradigm: influence of running shoes on joint movement. Med Sci Sports Exerc 2017 Mar 8. [Epub ahead of print]
- Nigg BM, Baltich J, Hoerzer S, Enders H. Running shoes and running injuries: mythbusting and a proposal for two new paradigms: ‘preferred movement path’ and ‘comfort filter’. Br J Sports Med 2015;49(20):1290-1294.
- Ferber R, Hettinga BA. A comparison of different over-the-counter foot orthotic devices on multi-segment foot biomechanics. Prosthet Orthot Int 2016;40(6):675-681.
- Nester CJ, Jarvis HL, Jones RK, et al. Movement of the human foot in 100 pain free individuals aged 18-45: implications for understanding normal foot function. J Foot Ankle Res 2014;7(1):51.
- Lundgren P, Nester C, Liu A, et al. Invasive in vivo measurement of rear-, mid- and forefoot motion during walking. Gait Posture 2008;28(1):93-100.





