

 By Patrick A. DeHeer, DPM, FACFAS, FASPS, FFPM RCPS (Glasg)
By Patrick A. DeHeer, DPM, FACFAS, FASPS, FFPM RCPS (Glasg)
Equinus is the primary mechanical cause of acquired non-traumatic foot and ankle pathology—plantar fasciitis, AT, and MSS—in running sports.
The three most common lower-extremity overuse injuries among those who participate in running-related sports such as basketball have all been linked to the same risk factor. If what the research suggests is true, treating this risk factor to prevent these injuries should be the standard of care, particularly for elite basketball players in the National Basketball Association (NBA) and Division I of the National Collegiate Athletic Association (NCAA). Athletic trainers and team physicians can reduce the risk of potentially devastating overuse injuries by applying a simple therapeutic measure.
James Amis, MD, former team physician for the Cincinnati Bengals, said, “We are awakening to a new era of understanding the mechanics and function of the human foot and ankle.”1 Contrary to the traditionally held belief that aging and obesity are to blame for the majority of foot and ankle problems, Amis asserts that equinus—through “indirect leveraged means as well as direct forces along the posterior/plantar chain”—is the primary mechanical cause of acquired non-traumatic foot and ankle pathology.1
Dias Lopes et al. conducted a systematic review to examine running-related musculoskeletal injuries.2 Of the 2,924 eligible titles, eight studies qualified for the review (n=3,500 runners). The authors found 28 running-related musculoskeletal injuries. The three most common general running-related musculoskeletal injuries were medial tibial stress syndrome (incidence range 13.6% to 20.0%; prevalence 9.5%), Achilles tendinopathy (incidence range 9.1% to 10.9%; prevalence range 6.2% to 9.5%), and plantar fasciitis (incidence range 4.5% to 10.0%; prevalence range 5.2% to 17.5%).2
Plantar Fasciitis
Plantar fasciitis has sidelined numerous professional and collegiate basketball players for extended periods of time. This disorder accounts for 5% to 11% of running injuries overall2-6 and 25% to 31% of foot injuries specifically.2-7 Given the similarities of movements involved in running and basketball, we can draw parallels between the two. Averaging the rates of plantar fasciitis in these two groups allows us to estimate a 10% to 15% incidence rate in basketball players.
There is a direct relationship between equinus and plantar fasciitis. Patel and DiGiovanni found an underlying equinus deformity in 83% of patients with acute or chronic plantar fasciitis.8 A more recent study by Nakale et al. examining the association between equinus and plantar fasciitis found that 80% of the plantar fasciitis group had an equinus deformity.9 They also found that female gender and age (41 to 64 years) are additional risk factors for plantar fasciitis.9 Given the strong association between isolated gastrocnemius tightness (IGT) and plantar fasciitis, as well as between IGT and other foot and ankle pathologies, the authors recommend that physicians evaluate and treat IGT early, either operatively or non-operatively, when managing these foot and ankle pathologies.9
Obesity is often cited as the cause for plantar fasciitis; however, the Achilles tendon has a much greater influence on the plantar fascia.10 Chueng and colleagues described the link between the two, stating that when tension on the Achilles tendon increases, tension also increases in the plantar fascia. Plantar fascia tension could be relieved, the authors conclude, by lengthening the Achilles tendon.10 It is also interesting to note that tension in the plantar fascia due to equinus places twice the tension on the plantar fascia due to increased body weight.10

While conservative measures are typically sufficient to treat plantar fasciitis, isolated gastrocnemius recession is also associated with excellent outcomes for recalcitrant plantar fasciitis, reinforcing the direct relationship between equinus and plantar fasciitis.11-15

Risks Factors Associated with Plantar Fasciitis
The risk of developing plantar fasciitis among basketball players has not been studied specifically; however, given the similarities between running and playing basketball, the literature assessing the risk for developing plantar fasciitis among runners can provide guidance when estimating the risk for developing plantar fasciitis among basketball players. A study by McNamee, for example, found that for every 1 degree decrease in ankle range of motion (ROM) among runners, the risk for developing plantar fasciitis increased nearly 15%, indicating a significant link between the two.16 The study also found that increased body mass index (BMI) and a pronated foot structure, common risk factors for developing plantar fasciitis, were not associated with an increased risk for developing the disorder among runners.16
Daniel Riddle and colleagues also found limited ankle joint dorsiflexion and increased BMI to be risk factors for developing plantar fasciitis in the general population. They found that those with ankle joint dorsiflexion of ≤ 0 degree were 23.3 times more likely to develop plantar fasciitis than those with ankle joint dorsiflexion of ≥ 10 degrees, and those with a BMI of ≥ 30 kg/m2 were 5.6 times more likely to develop plantar fasciitis than those with a BMI of ≤ 25 kg/m2.17 They also found that those with an active lifestyle were 3.6 times more likely to develop plantar fasciitis than those with a more sedentary lifestyle.17 It’s important to keep in mind that athletes with high muscle mass may have a BMI that categorizes them as obese even though they are not.
While the McNamee and Riddle studies both found a statistically significant link between the risk for developing plantar fasciitis and limited ankle joint dorsiflexion, high BMI, and a pronated foot structure among physically active individuals, they found that equinus carries a significantly greater risk.16,17 Interestingly, Sullivan and colleagues found that abnormal BMI, decreased ankle joint dorsiflexion, and reduced foot and ankle strength increased the risk of plantar fasciitis in the general population.18
Looking closer at dorsiflexion, Becker and colleagues examined the biomechanics of runners with Achilles tendinopathy (AT) or medial tibial stress syndrome (MTSS) compared to matched uninjured controls.19 There was a statistically significant difference in ankle joint dorsiflexion between the injured groups and the control groups, with the injured groups showing less dorsiflexion.19 There was also a statistically significant difference in standing tibial varus between the injured group and control group, while the remaining nine biomechanical findings showed no difference between the groups.19 The reduced static dorsiflexion in injured patients in this study aligns with previous studies, which have reported a lack of static ankle dorsiflexion to be predictive of developing both MTSS and AT, the authors concluded.19
Equinus and Achilles Tendinopathy
The relationship between equinus and AT is rooted in the evolutionary transformation from quadrupedal gait to bipedal gait that occurred between 2 and 3 million years ago.20,21 For bipedal gait to occur, the calcaneus dropped 70 degrees to sit flat on the ground.20 The GSC, hamstrings, and hip flexors lengthened for this structural change to occur.20 Since this happened later in the evolutionary process, these muscles are the first to tighten as a person ages.20 Theoretically, this results in intratendinous shear strain, which could cause inflammation of the peritenon.21,22
Although all three pathologies can result in significant loss of playing time for an elite basketball player, AT that progresses to Achilles tendon rupture is potentially career-ending. Trofa et al. found 30% of National Basketball Association, National Football League, and Major League Baseball athletes did not return to competition after an Achilles tendon rupture.23 In the first year following a rupture, professional athletes performed at substantially lower levels compared to their pre-injury performance metrics, taking two years to return to pre-injury performance levels.23
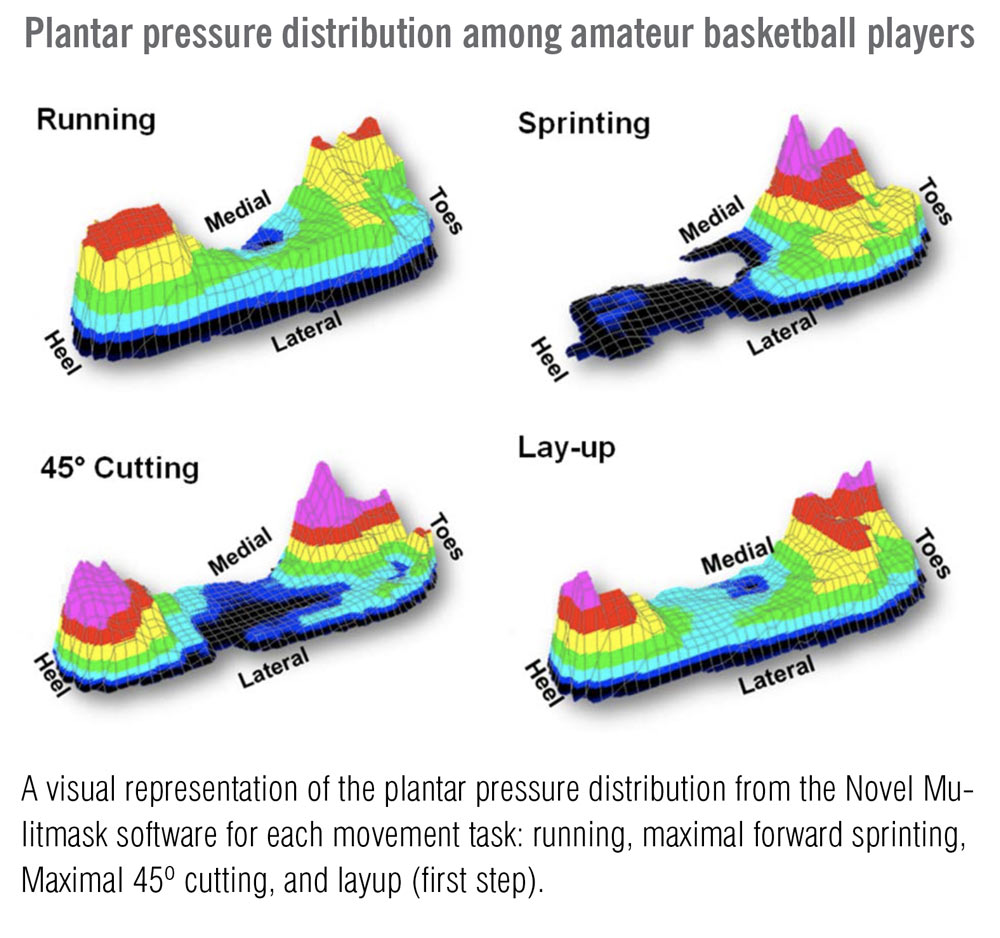
Figure. Kong et al created visual representations of the plantar pressure distribution using the Novel Mulitmask software for each movement task: running, maximal forward sprinting, maximal 45º cutting, and layup (first step). Used with permission of the Journal of the American Podiatric Medical Association. Kong PW et al. J Am Podiatr Med Assoc. 2018;108(3):215-224.
Understanding and Treating Equinus
If the three primary running-related pathologies all have a single common risk factor (equinus), why isn’t therapeutic stretching to reduce injury risk among elite basketball players common practice? Like many things regarding equinus, it may be due to a misunderstanding of stretching terminology and a lack of understanding of the significance of equinus. Given that not everyone with equinus has a pathology, some question whether equinus is a bad thing.24,25 Johnson and Christensen answer this question. “In clinical practice, the early destructive influence of equinus is often not appreciated,” they explained. “Instead, we are usually faced with the end result of equinus effects.”26
The misunderstanding about the benefits of therapeutic stretching in the athlete results from confusion about stretching terminology. The goal of stretching muscles and tendons is to increase ROM, flexibility, and muscle control.27 Static stretching requires holding a stretch in a challenging but comfortable position for a set period of time; dynamic stretching requires a stretch be performed while moving through a challenging but comfortable ROM.28 Stretching can also be passive (using body weight, gravity, another person, or a device) or active (contraction of the muscle in opposition to the muscle a person is stretching).28 Warm-up stretching is done just before athletic participation, while therapeutic stretching is used to help people regain lost function due to diminished ROM and, in some cases, to alleviate pain.29 Many healthcare providers and athletic trainers believe that stretching reduces athletic explosiveness among basketball players, which is only partially correct.
Research on the acute effects of stretching on strength performance shows stretching immediately before a strength activity decreased performance by 4.5% to 28%.30 Static stretching, however, produces significant increases in flexibility (important in equinus) while also increasing eccentric, concentric, and isometric peak torque.26 This is attributed to hypertrophy of the stretched muscles.30
Stone et al.’s systematic review of acute and chronic stretching on athletic performance found consistent reduced performance with warm-up static stretching.31 Seven of the articles reviewed showed that chronic therapeutic static stretching improved athletic performance, and two articles showed no negative or positive effects.31 The authors concluded that chronic therapeutic static stretching generally results in enhanced maximum strength and explosive strength performances. While the degree of enhancement appears to be small, ranging from 3% to 4%, incremental improvements can be significant in high-level sports.31
Ballistic stretching (static or dynamic stretching in a bouncing motion) is sometimes used as warm-up stretching, but Medeiros and Martini concluded that ballistic stretching did not increase dorsiflexion ROM. The authors found that chronic stretching, particularly when it includes a static component, can effectively improve ankle range of motion in healthy individuals.32
Conclusion
Stretching is an effective treatment for equinus. The evidence shows that equinus is the primary risk factor for plantar fasciitis, AT, and MSS in running-related sports. Healthcare professionals caring for elite basketball players with equinus should utilize chronic static therapeutic stretching regardless of symptomology to reduce the risk of running-related injuries.
Dr. DeHeer is a Fellow of the American College of Foot and Ankle Surgeons, and a Diplomate of the American Board of Podiatric Surgery. He is also a team podiatrist for the Indiana Pacers and the Indiana Fever. Dr. DeHeer is in private practice with various offices in Indianapolis and is the founder of Step by Step Haiti.
Disclosure: Dr. DeHeer reports that he is the inventor of The Equinus Brace™ and an owner of IQ Med.
- Amis J. The split-second effect: the mechanism of how equinus can damage the human foot and ankle. Front Surg. 2016;3:38.
- Lopes AD, Hespanhol Junior LC, Yeung SS, Costa, LO. What are the main running-related musculoskeletal injuries? A systematic review. Sports Med. 2012;42(10):891–905.
- Mohseni-Bandpei MA, Nakhaee M, Mousavi ME, et al. Application of ultrasound in the assessment of plantar fascia in patients with plantar fasciitis: a systematic review. Ultrasound Med Biol. 2014;40(8):1737–54.
- Taunton JE, Ryan MB, Clement DB, et al. A retrospective case-control analysis of 2002 running injuries. Br J Sports Med. 2002;36(2):95–101.
- Nielsen RO, Ronnow L, Rasmussen S, Lind M. A prospective study on time to recovery in 254 injured novice runners. PloS One. 2014;9(6):e99877.
- Hoffman MD, Krishnan E. Health and exercise-related medical issues among 1,212 ultramarathon runners: baseline findings from the Ultrarunners Longitudinal TRAcking (ULTRA) Study. PloS One. 2014;9(1):e83867.
- Di Caprio F, Buda R, Mosca M, et al. Foot and lower limb diseases in runners: assessment of risk factors. J Sports Sci Med. 2010;9(4):587–96.
- Patel A, DiGiovanni B. Association between plantar fasciitis and isolated contracture of the gastrocnemius. Foot Ankle Int. 2011;32(1):5–8.
- Nakale NT, Stydom A, Saragas MP, et al. Association between plantar fasciitis and isolated gastrocnemius tightness. Foot Ankle Int. 2018;39(3): 271–7.
- Cheung JTM, Zhang M, An KN. Effect of Achilles tendon loading on plantar fascia tension in the standing foot. Clin Biomech. 2006;21(2):194–03.
- Abbassian A, Kohls-Gatzoulis J, Solan MC. Proximal medial gastrocnemius release in the treatment of recalcitrant plantar fasciitis. Foot Ankle Int. 2012;33(1):14–9.
- Ficke B, Elattar O, Naranje SM, et al. Gastrocnemius recession for recalcitrant plantar fasciitis in overweight and obese patients. Foot Ankle Surg. 2017;epub June 17.
- Hoefnagels E, Weereheijm L, Louwerens JW, et al. Chronic therapy resistant plantar fasciitis, the effect of lengthening the gastrocnemius muscle. Foot Ankle Surg. 2016;22(2):58.
- Avila A, Monteagudo M, Martinez-Albornoz P, Maceira E. Medial gastrocnemius proximal release in chronic plantar fasciitis. Prospective study of 75 cases. Foot Ankle . 2016;22(2):24¬–25.
- Monteagudo M, Maceira E, Garcia-Virto V, Canosa R. Chronic plantar fasciitis: plantar fasciotomy versus gastrocnemius recession. Int Orthop. 2013;37(9):1845–50.
- McNamee MJ. 2016. Analysis of plantar fasciitis risk factors among intercollegiate and recreational runners: a matched case-control study (master’s thesis). Texas State University.
- Riddle DL, Pulisic M, Pidcoe P, Jonson RE. Risk factors for plantar fasciitis: a matched case-control study. J Bone Joint Surg Am. 2003;85(5):872–7.
- Sullivan J, Burns J, Adams R, et al. Musculoskeletal and activity-related factors associated with plantar heel pain. Foot Ankle Int. 2015;36(1):37–45.
- Becker J, James S, Wayner R, et al. Biomechanical factors associated with achilles tendinopathy and medial tibial stress syndrome in runners. Am J Sports Med. 2017;45(11):2614–21.
- Amis J. The gastrocnemius: a new paradigm for the human foot and ankle. Foot Ankle Clin. 2014;19(4):637–47.
- Malvankar S, Khan WS. Evolution of the Achilles tendon: The athlete’s Achilles heel? Foot. 2011;21(4):193–7.
- Järvinen TA, Kannus P, Maffulli, et al. Achilles tendon disorders: etiology and epidemiology. Foot Ankle Clin. 2005;10(2):255–66.
- Trofa DP, Miller JC, Jang ES, et al. Professional athletes return to play and performance after operative repair of an Achilles tendon rupture. Am J Sports Med. 2017;45(12):2864–71.
- Kirby KA. Equinus deformity: too many questions, not enough answers. Podiatry Today. 2017;30(12):58.
- Jarvis HL, Nester CJ, Bowden PD, et al. Challenging the foundations of the clinical model of foot function: further evidence that the root model assessments fail to appropriately classify foot function. J Foot Ankle Res. 2017;10(1):7.
- Johnson CH, Christensen JC. Biomechanics of the first ray part V: the effect of equinus deformity. J Foot Ankle Surg. 2005;44(2):114–20.
- Weerapong P; Hume PA, Kolt, GS. “Stretching: Mechanisms and Benefits for Sports Performance and Injury Prevention”. Phys Ther Rev. 2004;9(4):189–206.
- Blahnik J. Full body flexibility. 2nd ed. Champagne, Il:Human Kinetics; 2010. http://www.humankinetics.com/excerpts/excerpts/types-of-stretches.
- Lederman E. Therapeutic stretching. Towards a functional approach. London, England: Churchill Livingstone; 2013.
- Rubini EC, Costa AL, Gomes PS. The effects of stretching on strength performance. Sports Med. 2007;37(3):213–24.
- Stone M, Ramsey MW, Kinser AM, et al. Stretching: acute and chronic? The potential consequences. Strength Cond J. 2006;28(6):66.
- Medeiros DM, Martini TF. Chronic effect of different types of stretching on ankle dorsiflexion range of motion: systematic review and meta-analysis. Foot. 2018;Mar(34):28–35.





